
記住我









A total of 10,000 beds are available at Taiwan’s CGMH Medical System, which includes four tertiary care hospitals and three major teaching hospitals. The CGMH medical database contains records from 1 to 2001 to 31 March 2021, including diagnoses, laboratory data, medications, echocardiography, imaging, and detailed charts. In spite of the fact that the patient’s identity (i.e. the chart number or national identification number) was encrypted, every patient was assigned a personal identification number (PIN), which could be linked to their medical records. The CGMH medical database is described in greater detail elsewhere [21]. Research protocol approved by CGMH Institutional Review Board (IRB no. 202100393B0C601).
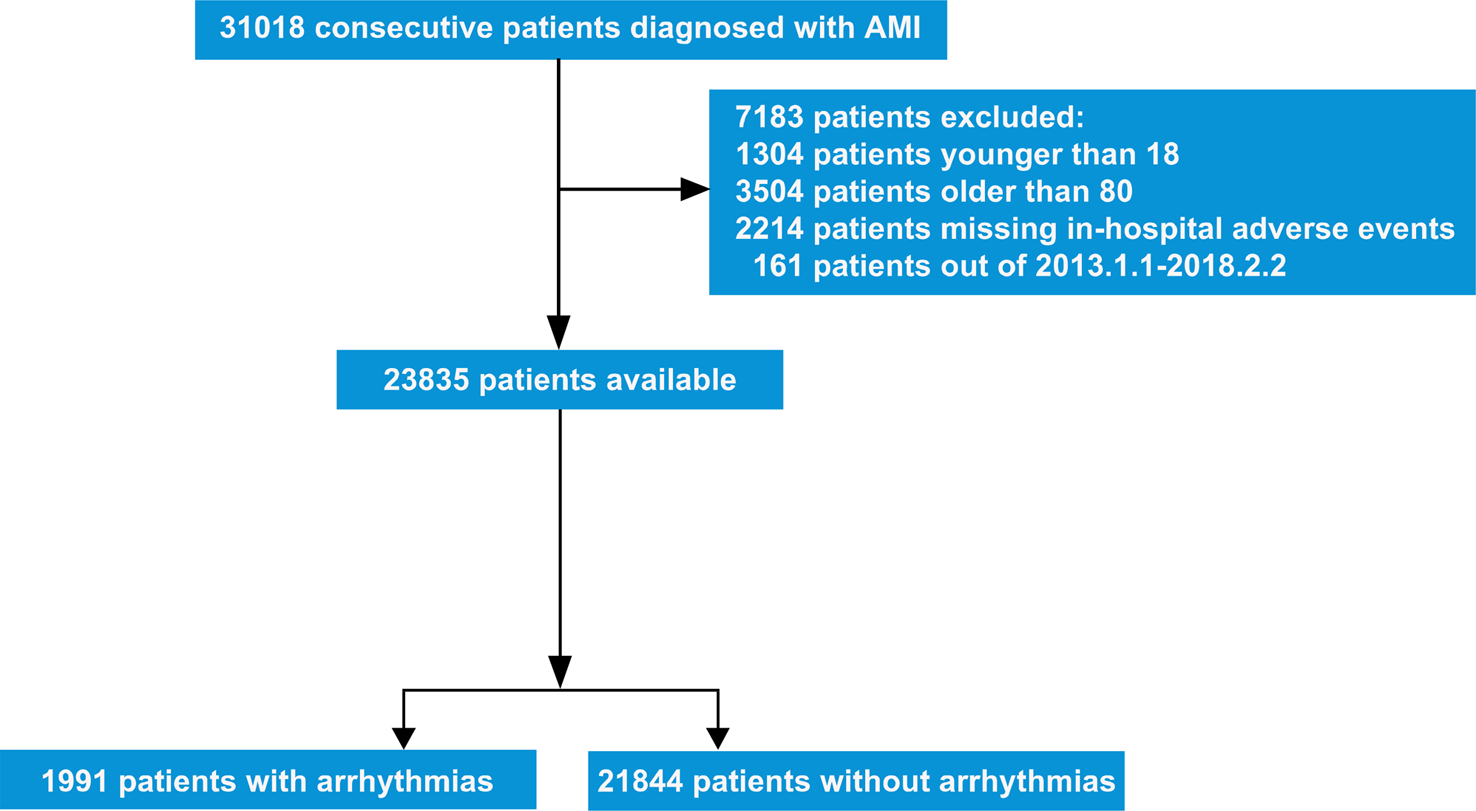
Study designThe retrospective, multicenter cohort study examined 38,069 hospitalized patients with acute decompensated heart failure who were discharged during the period of January 1, 2005, through December 31, 2019. It excludes individuals under the age of 18, type I diabetes mellitus, HIV, malignancy, autoimmune diseases, infective endocarditis, major organ transplants, cardiac resynchronization therapy devices, cardioverter defibrillators (ICD), permanent pacemakers (PPM), and absence of in-hospital echocardiography. The echographic examination and the ESC/AHA guidelines definition [4, 12] was used to classify 12,852 patients into three categories: HFrEF, HFmrEF, and HFpEF (Fig. 1).
Fig. 1
Enrollment and flowchart of the study
Baseline characteristicsThere were a number of HF-related comorbidities present, including hypertension, diabetes, dyslipidemia, atrial fibrillation, peripheral arterial disease, venous thromboembolism, chronic obstructive pulmonary disease, gouty arthritis, gastrointestinal bleeding, intracranial hemorrhage, ischemic heart disease, old ischemic stroke, status following coronary artery bypass surgery, and valve surgery. At least once in the one-year period before discharge, comorbidities were identified from outpatient, emergency, or inpatient records.
Discharge medicationsA review of medications prescribed within six months of discharge was conducted. The drugs prescribed included antiplatelets, oral anticoagulants, renin-angiotensin system inhibitors (RASi), beta-blockers, dihydropyridine calcium channel blockers (DCCB), calcium channel blockers (CCB), mineralocorticoid receptor antagonists (MRA), diuretics, oral glycemic agents (OHA), insulin therapy, and Satin. In accordance with World Health Organization Anatomical Therapeutic Chemical codes and Taiwan National Health Insurance reimbursement codes, guidelines-directed medical therapy (GDMT) includes RASi, beta-blockers, and MRA.
Survival and cardiovascular outcomesThe primary outcomes are cardiovascular death and rehospitalization for heart failure. As well as the primary outcomes of all-cause mortality, individual HF rehospitalizations, CV death, acute myocardial infarction (AMI), and ischemic stroke (IS), secondary outcomes are also evaluated. According to ICD-9-CM and ICD-10-CM diagnostic codes for any inpatient diagnosis (eAppendix 1 in the Additional File), the occurrence of cardiovascular death and heart failure rehospitalization was calculated. As defined by the National Registry of Death, CV death includes death from heart disease, hypertension, and cerebrovascular disease. Among the principal discharge diagnoses of hospitalization were ischemic stroke, acute myocardial infarction, and heart failure rehospitalization. From the index date to the date of an event or death, or March 31, 2021, whichever occurred first, each patient was followed.
Statistical analysisThe characteristics of patients with each HFrEF, HFmrEF, and HFpEF grade were compared in this study. A Chi-Squared test was used to compare categorical variables between HFrEF, HFmrEF, and HFpEF. ANOVA was used to compare continuous variables between HFrEF, HFmrEF, and HFpEF. Over a 5-year follow-up period, Kaplan–Meier plots were constructed comparing the primary outcome, all-cause mortality, CV death, heart failure rehospitalization, AMI and ischemic stroke. Events are defined as the occurrence of the outcomes of interest within five years of discharge. For survival curve analysis, patients with no events and no deaths during follow-up were censored. A Cox proportional hazard model was used to compare the risks of fatal outcomes (all-cause and cardiovascular death). In comparing non-fatal outcomes (HF rehospitalization, AMI, and ischemic stroke) between groups, Fine and Gray subdistribution hazard models were used. SAS version 9.4 (SAS Institute, Cary, NC) was used for all statistical analyses.
留言 (0)