
記住我









Phacoemulsification began with the single-handed engraving technique and evolved into the divide-and-conquer technique by Gimbel in 1991, the phaco-chop technique by Nagahara in 1993, and the prechop technique by Akahoshi in 1994.1–3 Many other variations of phacoemulsification techniques have been described.4–8 The use of ultrasonic oscillation energy increases the risk for injury to the corneal endothelial cells.9 Therefore, all these techniques are intended to decrease the total ultrasound time and energy used during nucleus emulsification and reduce the stress on the zonular fibers and capsule.
Akahoshi first developed the prechop technique in 1992 and presented it at the American Society of Cataract and Refractive Surgery Film Festival in 1994.10 The prechop technique manually divides the nucleus under a ophthalmic viscosurgical device before phacoemulsification.10 Compared with conventional grooving, divide-and-conquer, and phaco-chop techniques, the total ultrasound energy is drastically reduced, and the aspiration time and volume of the fluid used are significantly lower. However, the prechop technique is extremely difficult to perform and is rarely used globally. The prechopper tip is large and difficult to manipulate in the anterior chamber and is also dull, making it difficult to insert into the lens nucleus. In addition, the thick tip of the prechopper adds to the difficulty of insertion into the lens nucleus because of its resistance after insertion. This may be because only 4 articles, to the author's knowledge, have been published on the prechop technique in the past 30 years, with the exception of the study by Akahoshi.11–14
I have been using the prechop technique in cataract surgeries since 2000, and I developed the 8-chop technique in 2002. This is characterized by the division of the lens nucleus into 8 segments, instead of only 4 as in the prechop technique. I presented the 8-chop technique at the 32nd Annual Meeting of the Japanese Society of Ophthalmic Surgery in 2009.15 The Lance-chop technique is an 8-chop technique that uses the Lance-chopper and nucleus sustainer for cases with a hard lens nucleus. Since the Eight-chopper I and the Eight-chopper II cannot be inserted into a hard lens, the Lance-chop technique is used to divide the lens nucleus by inserting the Lance-chopper into the lens nucleus while supporting the lens equator with the nucleus sustainer and avoiding stress on zonular fibers. I presented this at the 42nd Annual Meeting of the Japanese Society of Ophthalmic Surgery in 2019.16
The aim of this study was to determine the operative time, phaco time, cumulative dissipated energy (CDE), and volume of the fluid used in the 8-chop technique and confirm its superiority over previous techniques. If the 8-chop technique, which is an improved version of the prechop technique, is found to be less invasive, it may become the technique of choice for more cataract surgeons.
METHODSIn this study, the efficiency and safety of the 8-chop technique were estimated. This study comprised eyes of patients with cataracts who had undergone phacoemulsification and posterior chamber intraocular lens (IOL) implantation between June 2018 and March 2022. Patients who had visited the clinic with a diagnosis of cataracts were enrolled in the study. The exclusion criteria were corneal disease or opacity, uveitis, pupillary dilation problem, and previous trauma or surgery. The data that support the findings of this study are available on request from the corresponding author.
The study protocol adhered to the tenets of the Declaration of Helsinki and was approved by the review board. Informed consent for participation in this study was obtained from each patient. Preoperatively, all patients underwent slitlamp and retinal examinations, and their corrected distance visual acuity (CDVA) and intraocular pressure (IOP) were measured. Endothelial cell density (cells/mm2) was measured using a noncontact specular microscope (EM-3000, Topcon Corp.). The firmness of the nucleus was graded using the Emery classification, based on which the patients were classified into 1 of 3 groups (Grade II, Grade III, or Grade IV).17 As an exception, the Grade IV group included Grade IV and V cataracts. Phacoemulsification was performed by the same surgeon, who was experienced in the 8-chop technique, using the Centurion phacoemulsification unit (Alcon Laboratories, Inc.).
Three new surgical instruments were designed and developed to perform the 8-chop technique (Figure 1). The research team designed these eight-choppers and requested a manufacturing company to produce them. The Eight-chopper I (SP-8193, ASICO LLC) has a smaller tip than that of the conventional prechopper, with a length and width of 3.2 mm and 1.4 mm, respectively, as well as a sharper leading edge, and was used for the Grade II group. The Eight-chopper II (SP-8402, ASICO LLC) has a smaller tip (2.5 mm long and 0.8 mm wide) that is angled so that it can be inserted vertically into the lens nucleus for the Grade III group. For the Grade IV group, the tip of the Lance-chopper (SP-9989, ASICO LLC) was 3.0 mm long and 1.3 mm wide, and the leading edge was sharper.
 Figure 1.:
Figure 1.: Eight-choppers and Universal II prechopper. a: the Eight-chopper I (SP-8193); b: the Eight-chopper II (SP-8402); c: the Lance-chopper (SP-9989); and d: The Universal II Prechopper (AE-4192).
In all surgeries, a temporal, clear, corneal incision was formed using a 3.0 mm steel keratome. After the injection of sodium hyaluronate into the anterior chamber, a 6.2 to 6.5 mm continuous curvilinear capsulorrhexis (CCC) was created with a capsule forceps. The soft-shell technique was used in the Grade III and IV groups.18 Brilliant blue G (0.025%) was used to improve visualization of the capsule in cases with dense cataracts or corneal opacity. Hydrodissection was performed with a 27-gauge cannula; however, hydrodelineation was never performed. The lens nucleus was cracked into 8 segments using the Eight-chopper I in the Grade II group, the Eight-chopper II in the Grade III group, and the Lance-chopper in the Grade IV group (Figures 2 and 3; Videos 1 and 2 available at https://links.lww.com/JRS/A801 and https://links.lww.com/JRS/A802). A 1 side-port incision was made using the 23-gauge microvitreoretinal knife 90 degrees from the main incision in the Lance-chop technique. The 8 segments were phacoemulsified and aspirated at the depth of the iris plane. The capsular bag was aspirated with the irrigation/aspiration tip to remove the cortical material. A ophthalmic viscosurgical device was injected, and a foldable IOL (Alcon Laboratories, Inc.) with polymethyl methacrylate haptics was inserted in the capsular bag with an injector system. The ophthalmic viscosurgical device was then aspirated. The Centurion phacoemulsification unit was used in all cases and had a flow rate of 32 mL/min, a maximum ultrasound power of 80%, and a 1.1 mm tip. The wound was sealed using stromal hydration if necessary. At the end of the operation, the anterior chamber was replaced by balanced salt solution containing moxifloxacin (0.5 mg/mL).
 Figure 2.:
Figure 2.: a: First, the lens nucleus is divided into hemispheres using the Eight-chopper. b: Then, the lens nucleus is rotated 90 degrees and divided into quadrants. c: The lens nucleus divided into quadrants is rotated 45 degrees and divided into 6 segments. d: Finally, the remaining quadrants of the lens nucleus are also divided to complete the eight segmentation.
 Figure 3.:
Figure 3.: a: First, the lens nucleus is divided into hemispheres using the Lance-chopper, while the nucleus sustainer (AE-2530) is inserted through the side port to support the equator of the lens nucleus. b: Then, the lens nucleus is rotated 90 degrees and divided into quadrants. c: The lens nucleus divided into quadrants is rotated 45 degrees and divided into 6 segments. d: Finally, the remaining quarter of the lens nucleus is also divided to complete the eight segmentation.
The intraoperative outcome measures were phaco time (seconds), CDE, operative time (minutes), volume of fluid used (milliliters), and the rate of intraoperative complications. The operative time was measured from the beginning of the corneal incision to the end of ophthalmic viscosurgical device aspiration. Patients were followed up on postoperative days 1 and 2 and at postoperative weeks 1, 3, 7, and 19. The postoperative outcome measures were CDVA, IOP measurements, and endothelial cell density (cells/mm2). Data on the outcome measures at 7 and 19 weeks postoperatively were used to conduct this study.
Statistical analyses were performed to compare the results between the groups using either 1-way analysis of variance (ANOVA) or 1-way ANOVA followed by the Bonferroni post hoc test using Excel Toukei (v. 7.0, Esumi Co. Ltd.). The preoperative and postoperative results of the 3 groups were analyzed using 2-way ANOVA using Excel Toukei (v. 7.0). The variance of each group was confirmed to be equally distributed using the Bartlett test. P < .05 was considered statistically significant.
RESULTSThis study comprised 150 eyes of 107 patients with cataract who had undergone phacoemulsification and posterior chamber IOL implantation. Each cataract density group (Grade II, III, and IV) included 50 eyes. A total of 113 eyes could be followed up to 19 weeks postoperatively: 34 in the Grade II group, 42 in the Grade III group, and 37 in the Grade IV group. The patients' characteristics and intraoperative parameters are given in Table 1. There were significant differences in the mean ages among the groups (P < .01, 1-way ANOVA). The mean operative time in the Grade II group was significantly shorter than that in the Grade III and IV groups (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The mean operative time in the Grade III group was also significantly shorter than that in the Grade IV group (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The mean phaco time in the Grade II group was significantly shorter than that in the Grade III and IV groups (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The mean phaco time in the Grade III group was also significantly shorter than that in the Grade IV group (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The CDE in the Grade II group was significantly lesser than that in the Grade III and IV groups (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The CDE in the Grade III group was also significantly lesser than that in the Grade IV group (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The volume of the fluid used in the Grade II group was significantly lesser than that used in the Grade III and IV groups (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test). The volume of the fluid used in the Grade III group was also significantly lesser than that used in the Grade IV group (P < .01, 1-way ANOVA followed by the Bonferroni post hoc test).
Table 1. - Preoperative characteristics and intraoperative parameters Parameters Grade II Grade III Grade IV P value n 50 50 50 Age (y), mean ± SD 72.8 ± 5.6 77.5 ± 7.2 77.1 ± 8.8 <.01* Sex, n (%) M/F 19 (38)/31 (62) 16 (32)/34 (68) 29 (58)/21 (42) Operative time (min), mean ± SD 3.72 ± 0.45 5.42 ± 1.05 9.63 ± 2.15 <.01* Phaco time (s), mean ± SD 11.6 ± 4.1 20.2 ± 5.4 28.7 ± 8.5 <.01* CDE, mean ± SD 5.00 ± 1.88 9.24 ± 2.00 14.81 ± 5.20 <.01* Volume of fluid used (mL), mean ± SD 22.9 ± 6.1 33.3 ± 6.5 44.1 ± 8.4 <.01*CDE = cumulative dissipated energy
*Statistically significant (1-way ANOVA)
The CDVA (logMAR) preoperatively, at 7 weeks, and 19 weeks postoperatively in the Grade II group were 0.081 ± 0.13 (mean ± SD), −0.054 ± 0.043, and −0.048 ± 0.047, respectively. The CDVA preoperatively, at 7 weeks, and 19 weeks postoperatively in the Grade III group were 0.30 ± 0.34, −0.024 ± 0.095, and −0.023 ± 0.096, respectively. The CDVA preoperatively, at 7 weeks, and 19 weeks postoperatively in the Grade IV group were 0.52 ± 0.58, −0.039 ± 0.22, and 0.027 ± 0.23, respectively. There were significant differences in the CDVA among the groups preoperatively, at 7 weeks, and 19 weeks postoperatively (P < .01, P < .01, and P = .038, respectively, 1-way ANOVA). The CDVA differed significantly between the groups preoperatively and at 7 weeks postoperatively (P < .01, 1-way ANOVA). The CDVA between the groups also differed significantly preoperatively and at 19 weeks postoperatively (P < .01, 1-way ANOVA).
The changes in the corneal endothelial cell density in each group are given in Table 2. The preoperative corneal endothelial cell density did not differ significantly among the groups (P = .30, 1-way ANOVA) nor did it differ at 7 and 19 weeks postoperatively (P = .60, P = .18, respectively, 1-way ANOVA). Furthermore, the corneal endothelial density did not differ significantly among the 3 groups, even at 7 and 19 weeks postoperatively (P = .22, P = .09, respectively, 2-way ANOVA).
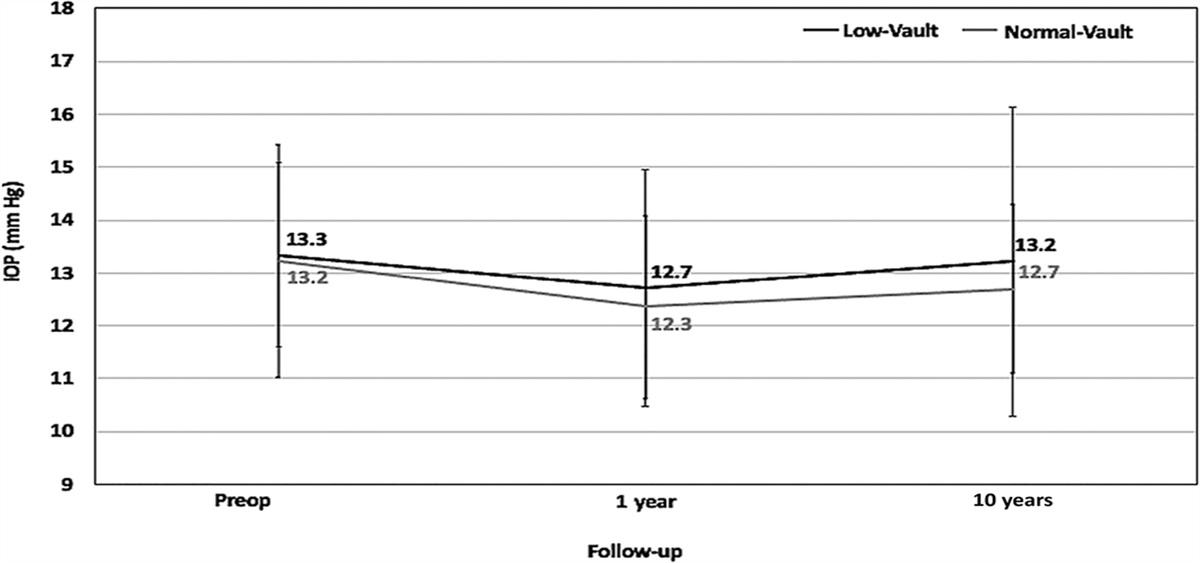
Table 2. - Preoperative and postoperative corneal endothelial cell density measurements (cells/mm2) Parameters Grade II Grade III Grade IV P value Preop 2579 ± 234 2502 ± 290 2565 ± 260 .30 7-wk postop 2456 ± 358 2390 ± 392 2448 ± 303 .60The changes in the IOP of each group are given in Table 3. There were no significant differences in the preoperative IOP among the groups (P = .19, 1-way ANOVA). The IOP was significantly lower at 7 and 19 weeks postoperatively than the preoperative IOP in all 3 groups (P < .01, P < .01, respectively, 2-way ANOVA). The IOPs of the 3 groups did not differ significantly at 7 and 19 weeks postoperatively (P = .83, P = .69, respectively, 1-way ANOVA). No intraoperative complications were observed, and no capsulorrhexis tears occurred in the 3 groups.
Table 3. - Preoperative and postoperative IOP measurements (mm Hg) Parameters Grade II Grade III Grade IV P value Preop 13.9 ± 2.0 14.6 ± 1.9 14.4 ± 2.1 .19 7-wk postop 12.3 ± 2.3 12.1 ± 2.1 12.1 ± 2.3 .83* 19-wk postop 11.7 ± 2.5 12.0 ± 2.0 11.9 ± 2.2 .69**Statistically significant P <.01 (2-way ANOVA)
This study revealed that the operative time of the eight-chop technique was 4 to 6 minutes in the Grade II and III groups, which is extremely short compared with that of other techniques that have been reported to take 10 to 19 minutes.18–24 Even in cases with hard lens nuclei, the Lance-chop technique can be completed in less than 10 minutes, which may be shorter than the phaco-chop technique, which reportedly takes 12 minutes.25 The 8-chop technique had a lower phaco time and CDE than other techniques; it also had an extremely low volume of fluid, that is, one-third to one-fourth of that used for other techniques.18–21,23–26 In particular, the use of a low volume of fluid means that ultrasound and irrigation/aspiration tips are inserted into the eye for a short period, which may have little impact on ocular tissues other than corneal endothelial cells.
Corneal endothelial cell density represents the true summation of intraocular insult during surgery, and its assessment is the key to its comparison between various techniques.27 Previous studies have reported a 5% to 16% decrease in corneal endothelial cell density after cataract surgery in the first few postoperative months; however, in this study, the decrease was 0.9%, 1.0%, and 5.3% in the Grade II, III, and IV groups, respectively, with no significant difference after 19 weeks in all groups.18,19,21,24–26,28 These results indicate that the 8-chop technique may be advantageous in surgical invasion of the intraocular tissue.
A decrease in the IOP after cataract surgery has been reported in both nonglaucoma and glaucoma patients.29–32 Similarly, in this study using the 8-chop technique, the postoperative IOP decreased by 2.2 to 2.5 mm Hg in all 3 groups. By comparing the 8-chop technique with other techniques, it may become clear whether the 8-chop technique is effective in IOP reduction for cataract patients with concomitant glaucoma.
There are a few differences between the prechop and 8-chop techniques. First, in the prechop technique, the lens nucleus is usually divided into 4 sections, whereas in the 8-chop technique, the lens nucleus is always divided into 8 sections.10,33 This is the advantage of the 8-chop technique over the prechop technique because the smaller divided pieces of the lens nucleus allow for more efficient phacoemulsification and aspiration.
The second difference is the development and use of special choppers with sharper and more delicate tips, such as the Eight-chopper 1, Eight-chopper 2, and Lance-chopper. These surgical instruments facilitate the eight-piece division of the lens nucleus, which is very difficult with the surgical instruments used in the prechop technique. Furthermore, these instruments are very useful in difficult cases because they reduce stress on the zonular fibers and lens capsule.
Third, in the 8-chop technique, the CCC is enlarged for safety. In the prechop technique, a CCC diameter of just <5 mm is recommended for a 5.5 mm diameter IOL and a CCC with a diameter of 5 mm is ideal for a 6 mm diameter IOL.10,33 In the 8-chop technique, a 6 mm diameter IOL is used and the CCC diameter is 6.2 to 6.5 mm. Creating a larger CCC reduces friction between the lens capsule and lens nucleus and facilitates rotation of the lens nucleus. In addition, phacoemulsification of the lens nucleus can be performed safely because it is not obstructed by the anterior lens capsule. Similarly, the lens cortex can also be aspirated safely and efficiently. The other major problem with small-radius CCCs is the development of capsule contraction syndrome. The radius of the CCC shrinks to 86% after surgery.34 However, a large CCC can impair the shrink wrap effect on IOL and cause IOL to tilt. This tilt can have a greater impact on visual function in toric and presbyopia-correcting IOLs than in monofocal lenses, and one should be cautious in its use.
Fourth, the Lance-chop technique is more ideal than the counter prechop technique for difficult cases, such as those with a hard lens nucleus or loose zonular fibers because it minimizes the stress on the posterior capsule and zonular fibers. The counter prechop technique is also used for dense cataracts in the prechop technique; however, the Lance prechopper is smaller and sharper than the Akahoshi Universal II prechopper (AE4192, ASICO LLC), allowing the lens nucleus to be divided safely and efficiently.10 Furthermore, it is not possible to eliminate the stress on the posterior capsule and zonular fibers with the divide-and-conquer and phaco-chop techniques.
The prechop and 8-chop techniques have features not possessed by other techniques. The prechop and 8-chop techniques can distinguish both the division and phacoemulsification of the lens nucleus, allowing the surgeon to concentrate on each individual procedure. In other techniques, such as the divide-and-conquer and phaco-chop techniques, wherein lens nucleus division and phacoemulsification are performed simultaneously, the accuracy of each procedure may be compromised. If one procedure is given more attention, lens nucleus division and phacoemulsification and aspiration can be performed with more certainty.
Another advantage of both the prechop and 8-chop techniques is that the ultrasound handpiece is held with both hands, allowing for delicate manipulation. In the divide-and-conquer and phaco-chop techniques, a hook or phaco-chopper is held in one hand and the ultrasound handpiece in the other, making it less stable compared with handling it with both hands. However, the study has some limitations. Even with the 8-chop technique, cases with weak zonular fibers, corneal opacity, mature cataract, and small pupil require difficult procedures; thus, each case must be prepared for, and all possible precautions must be taken preoperatively.
The prechop technique has the potential to reduce operative time but is rarely used because of its difficulty. The 8-chop technique is a more advanced technique and has the advantages of the prechop technique while eliminating its difficulties. Many cataract surgeons have abandoned the use of the prechop technique because of its difficulty, and even today, most cataract surgeons use the divide-and-conquer technique. A recent study using the divide-and-conquer technique reported a mean operative time of 19 min, a volume of fluid used of 360 mL, and a decrease in the corneal endothelial cell count of 8.5% at 3 weeks postoperatively.24 In the future, the effectiveness of the eight-chop technique may be confirmed by comparing it with the divide-and-conquer and phaco-chop techniques.
A 3 mm corneal incision used in this study needs to be considered in induced astigmatism because the size of the incision in modern cataract surgery is usually around 2.4 mm. The Eight-choppers used in this study can also be used with a corneal incision width of 2.6 mm, so it is possible to perform the 8-chop technique with a smaller corneal incision width.
In conclusion, to our knowledge, this is the first study to report that the 8-chop technique, in which the lens nucleus is always divided into 8 sections before phacoemulsification and aspiration, followed by efficient processing of the lens nucleus, has a very short-operative time and less CDE and volume of fluid used, as well as minimal corneal endothelial cell loss. This study did not compare the results with the prechop, phaco-chop, or divide-and-conquer techniques, and this should be fully considered when evaluating the present results. However, many other studies have been conducted using the phaco-chop and divide-and-conquer techniques, and we believe it is possible to partially evaluate the safety and efficiency of the 8-chop technique by comparing it with those results. In particular, the Lance-chop technique can safely divide the hard lens without stressing the zonular fibers, making it possible to perform phacoemulsification surgery even in cases in which division of the lens nucleus is very difficult. If more surgeons are able to perform the Lance-chop technique, it may be possible to provide safer phacoemulsification surgery to patients who have previously undergone intracapsular or extracapsular cataract extraction because of difficulties.WHAT WAS KNOWN Phacoemulsification began with the single-handed engraving technique and evolved into the divide-and-conquer, the phaco-chop, and the prechop technique. Previous studies have reported a 5% to 16% decrease in corneal endothelial cell density after cataract surgery.
WHAT THIS PAPER ADDS The eight-chop technique which divides the lens nucleus into 8 segments is safe and effective in phacoemulsification. The corneal endothelial cell density loss was 0.9% to 5.3%, with no significant difference after 19 weeks in this study. The Lance-chop technique is ideal technique for a hard lens nucleus or loose zonular fibers, as it minimizes the stress on the posterior capsule and zonular fibers. REFERENCES 1. Gimbel HV. Divide and conquer nucleofractis phacoemulsification: development and variations. J Cataract Refract Surg 1991;17:281–291 2. Chang DF. Why learn chopping? In: Chang DF, ed. Phaco Chop and Advanced Phaco Techniques. Thorofare, NJ: SLACK Inc.; 2013:3–9 3. Akahoshi T. Phaco prechop: manual nucleofracure prior to phacoemulsification. Operat Tech Cataract Refract Surg 1998;1:69–91 4. Koch PS, Katzen LE. Stop and chop phacoemulsification. J Cataract Refract Surg 1994;20:566–570 5. Vasavada AR, Desai JP. Stop, chop, chop, and stuff. J Cataract Refract Surg 1996;22:526–529 6. Aslan BS, Müftüoglu O, Gayretli D. Crater-and-split technique for phacoemulsification: modification of the crater-and-chop technique. J Cataract Refract Surg 2012;38:1526–1530 7. Vanathi M, Vajpayee RB, Tandon R, Titiyal JS, Gupta V. Crater-and-chop technique for phacoemulsification of hard cataracts. J Cataract Refract Surg 2001;27:659–661 8. Arshinoff SA. Phaco slice and separate. J Cataract Refract Surg 1999;25:474–478 9. Zetterström C, Laurell CG. Comparison of endothelial cell loss and phacoemulsification energy during endocapsular phacoemulsification surgery. J Cataract Refract Surg 1995;21:55–58 10. Akahoshi T. Phaco prechop. In: Chang DF, ed. Phaco Chop and Advanced Phaco Techniques. Thorofare, NJ: SLACK Inc.; 2013:55–76 11. Kongsap P, Wiriyaluppa C. A comparison of patient pain during cataract surgery with topical anesthesia in prechop manual phacofragmentation versus phacoemulsification. J Med Assoc Thai 2006;89:959–966 12. Yang K, Li J, Zhang W, Liu Z, Song C, Zhao Y. Comparison of pre-chop technique using a reverse chopper and classic stop-and-chop technique in the treatment of high myopia associated with nuclear cataract. BMC Surg 2022;22:206 13. Zhao J, Li Z, Liu Y, Han X, Huang S. Application of prechop technique in phacoemulsification for cataract patients with highly liquefied vitreous: a retrospective study. BMC Ophthalmol 2022;22:167 14. Zhao Y, Li J, Yang K, Zhu S. A prechop technique using a reverse chopper. J Invest Surg 2019;32:199–207 15. Sato T. The usefulness of the new Eight-chopper. Oral presented at: The 32nd Annual Meeting of the Japanese Society of Ophthalmic Surgery; January 23, 2009; Kobe, Japan 16. Sato T. The usefulness of the Lance-chopper. Oral presented at: The 42nd Annual Meeting of the Japanese Society of Ophthalmic Surgery; February 1, 2019; Yokohama, Japan 17. Emery JM. Kelman phacoemulsification; patient selection. In: Emery JM, Mclyntyre DJ, eds. Extracapsular Cataract Surgery. St Louis, MO: CV Mosby; 1983:95–100 18. Miyata K, Nagamoto T, Maruoka S, Tanabe T, Nakahara M, Amano S. Efficacy and safety of the soft-shell technique in cases with a hard lens nucleus. J Cataract Refract Surg 2002;28:1546–1550 19. Sato M, Sakata C, Yabe M, Oshika T. Soft-shell technique using Viscoat and Healon 5: a prospective, randomized comparison between a dispersive-viscoadaptive and a dispersive-cohesive soft-shell technique. Acta Ophthalmol 2008;86:65–70 20. Helvacioglu F, Yeter C, Tunc Z, Sencan S. Outcomes of torsional microcoaxial phacoemulsification performed by 12-degree and 22-degree bent tips. J Cataract Refract Surg 2013;39:1219–1225 21. Storr-Paulsen A, Norregaard JC, Ahmed S, Storr-Paulsen T, Pedersen TH. Endothelial cell damage after cataract surgery: divide-and-conquer versus phaco-chop technique. J Cataract Refract Surg 2008;34:996–1000 22. Wong T, Hingorani M, Lee V. Phacoemulsification time and power requirements in phaco chop and divide and conquer nucleofractis techniques. J Cataract Refract Surg 2000;26:1374–1378 23. Helvacioglu F, Yeter C, Sencan S, Tunc Z, Uyar OM. Comparison of two different ultrasound methods of phacoemulsification. Am J Ophthalmol 2014;158:221–226.e1 24. Igarashi T, Ohsawa I, Kobayashi M, Umemoto Y, Arima T, Suzuki H, Igarashi T, Otsuka T, Takahashi H. Effects of hydrogen in prevention corneal endothelial damage during phacoemulsification: a prospective randomized clinical trial. Am J Ophthalmol 2019;207:10–17 25. Abdelmotaal H, Abdel-Radi M, Rateb MF, Eldaly ZH, Abdelazeem K. Comparison of the phaco chop and drill-and-crack techniques for phacoemulsification of hard cataracts: a fellow eye study. Acta Ophthalmol 2021;99:e378–e386 26. Park J, Yum HR, Kim MS, Harrison AR, Kim EC. Comparison of phaco-chop, divide-and-conquer, and stop-and-chop phaco techniques in microincision coaxial cataract surgery. J Cataract Refract Surg 2013;39:1463–1469 27. Upadhyay S, Sharma P, Chouhan JK, Goyal R. Comparative evaluation of modified crater (endonucleation) chop and conventional crater chop techniques during phacoemulsification of hard nuclear cataracts: a randomized study. Indian J Ophthalmol 2022;70:794–798 28. Vajpayee RB, Kumar A, Dada T, Titiyal JS, Sharma N, Dada VK. Phaco-chop versus stop-and-chop nucleotomy for phacoemulsification. J Cataract Refract Surg 2000;26:1638–1641 29. Irak-Dersu I, Nilson C, Zabriskie N, Durcan J, Spencer HJ, Crandall A. Intraocular pressure change after temporal clear corneal phacoemulsification in normal eyes. Acta Ophthalmol 2010;88:131–134 30. Steuhl KP, Marahrens P, Frohn C, Frohn A. Intraocular pressure and anterior chamber depth before and after extracapsular cataract extraction with posterior chamber lens implantation. Ophthalmic Surg 1992;23:233–237 31. Tennen DG, Masket S. Short-and long-term effect of clear corneal incisions on intraocular pressure. J Cataract Refract Surg 1996;22:568–570 32. Chen PP, Lin SC, Junk AK, Radhakrishnan S, Singh K, Chen TC. The effect of phacoemulsification on intraocular pressure in glaucoma patients: a report by the American Academy of Ophthalmology. Ophthalmology 2015;122:1294–1307 33. Akahoshi T. Phaco Prechop: Re-evaluation of single-handed phacoemulsification using a new nucleofracture technique. Atarashii Ganka 1999;16:1219–1233 34. Park TK, Chung SK, Baek NH. Changes in the area of the anterior capsule opening after intraocular lens implantation. J Cataract Refract Surg 2002;28:1613–1617
留言 (0)