
記住我


Celiac disease (CeD) is a common gluten-dependent autoimmune condition affecting 1%–2% of the global population (1). In patients with positive serologic markers (IgA anti-transglutaminase 2 [anti-TG2] and antiendomysium [EMA]) and duodenal villous atrophy, the diagnosis of CeD is clear-cut (2). However, 10%–30% of patients evaluated for suspected CeD show only mild histopathologic changes and fluctuating serologic markers, a condition identified as potential CeD, or present with seronegative villous atrophy. In such cases, the diagnosis may remain uncertain (3,4).
Intestinal antitransglutaminase 2 antibodies (I-anti-TG2) are a marker of CeD (5,6). I-anti-TG2 are produced by specific activated B lymphocytes in the small intestinal mucosa before the appearance of serum anti-TG2 or mucosal damage. I-anti-TG2 have high sensitivity and specificity for CeD and identify those patients with potential CeD who are at risk of progression to villous atrophy (3,5,6). Their use in clinical practice could therefore help improve the accuracy of the overall testing strategy for CeD both in patients in whom the diagnosis is equivocal and in patients with potential CeD or seronegative villous atrophy (6,7).
I-anti-TG2 can be detected by double immunofluorescence staining on frozen duodenal sections (deposit technique) (8) or using an endomysial antibody assay in the supernatants of duodenal biopsies after incubation with gliadin fragments for 72 hours (EMA biopsy) (9). The diagnostic accuracy of these techniques is comparable because they both have high sensitivity and specificity. However, their implementation in clinical practice is limited by the fact that they both require experienced operators and equipped laboratories (10–12).
In this study, we evaluated the diagnostic accuracy of an immunochromatographic assay, referred to as Rapid_AntiTG2, to detect I-anti-TG2 in the supernatant obtained after simple mechanical lysis of fresh intestinal biopsy specimens. If accurate, this test could be used to easily detect I-anti-TG2 in any endoscopy unit.
MATERIAL AND METHODS Study design and patient populationThis was a diagnostic test accuracy study conducted at a single tertiary care pediatric gastroenterology center (IRCCS Burlo Garofolo, Trieste, Italy) between July 2020 and January 2022. The study was approved by the institutional review board (IRB-Burlo 06/2021). Written informed consent was obtained from patients or legal guardians. Eligible patients were children and young adults referred for an elective upper esophagogastroduodenoscopy (EGD). Exclusion criteria were gluten-free diet (GFD), bleeding disorders, and no indication for intestinal biopsy as part of the diagnostic process, including patients with suspected CeD who met the criteria for a no-biopsy diagnosis.
CeD status was established as per the European Society of Paediatric Gastroenterology and Nutrition (ESPGHAN) guidelines on the basis of positive serology and histopathology or serology alone in patients with anti-TG2 IgA > ×10 the upper limit of normality and EMA positivity in a second blood sample (2).
Classical CeD was diagnosed in patients with positive serology (anti-TG2 and EMA) and villous atrophy (Marsh classification 2 or 3); potential CeD was diagnosed in patients with positive serology (anti-TG2 and EMA) and normal duodenal architecture (Marsh classification 0 or 1) (2); seronegative CeD was diagnosed in patients with negative serology (negativity of both anti-TG2 and EMA) in the presence of villous atrophy (Marsh classification 2 or 3) and compatible human leukocyte antigen (HLA). Patients with normal duodenal histopathology and negative CeD serology were defined as controls.
Anti-TG2 were determined with a fluoroenzyme immunoassay (EliA immunoassay, Thermo Fisher Diagnostics, Oslo, Norway); negative cutoff value <7 U/mL.
HLA genotyping was determined by polymerase chain reaction (PCR) with allele-specific primers identifying HLA DQ2 and DQ8 haplotypes using Eu-Gen Risk kit (Eurospital Spa, Trieste, Italy). During EGD, 4 biopsies were collected from duodenal bulb (DB) and 4 from distal duodenum (DD). For each sampling site, 2 biopsies were correctly oriented on acetate cellulose filter (Bio-Optica Milan) and were analyzed for standard histopathology, 1 biopsy was cultured to perform EMA biopsy, and 1 biopsy was mechanically lysed to perform the Rapid_AntiTG2.
Testing methods Rapid immunochromatographic assay (Rapid_AntiTG2).One biopsy from each sampling site was placed in a vial with sterile buffer solution and was ground with a pestle. Ninety microliters of supernatant was loaded into the hole of Xeliac Test Professional cassette (Eurospital, Trieste, Italy). A valid positive test shows a blue control line, confirming that the test is working properly, and a red/pink line indicating binding between TG2 on the cassette's membrane and IgA/IgG/IgM anti-TG2 in the biopsy specimen, as shown in Figure 1. The test results were independently interpreted by 2 operators.
 Figure 1:
Figure 1: (a) Schematic representation of how the Rapid_AntiTG2 works. (b) Test results: a, strongly positive; b, slightly positive; c, negative.
EMA biopsy.Two intestinal fragments, one from DB and the other from DD, were cultured for 72 hours at 37 °C with peptic-tryptic digest of gliadin following manufacturer's instructions (Antiendomysium biopsy kit, Eurospital). The culture supernatants were collected and stored at −20 °C until analysis. Intestinal IgA EMA secreted into culture supernatants were detected in undiluted supernatant. Intestinal IgM EMA were investigated in patients with selective IgA deficiency.
Outcome measuresThe primary outcomes were sensitivity, specificity, and likelihood ratios (LR) of the Rapid_AntiTG2 test compared with those of the reference standard (serology and histopathology) for the diagnosis of CeD. The secondary outcome was the agreement of Rapid_AntiTG2 with EMA biopsy.
Statistical analysisA sample size of 98 patients (with CeD, n = 44) was calculated assuming a prevalence of CeD in the reference population (children and young adults undergoing an elective EGD at a Pediatric Gastroenterology Unit) of approximately 45%, choosing alpha = 0.05, and estimating sensitivity = 0.95 and specificity = 0.95 (estimated LR+ = 19), supposing LR+ = 8 as lower bound of confidence interval, for the new diagnostic technique (Rapid_AntiTG2) under investigation (13). Sensitivity of the Rapid_AntiTG2 test was calculated by dividing the number of patients with CeD who had a positive test result by the total number of patients diagnosed with CeD according to current consensus guidelines (see above); to calculate specificity, the number of patients without CeD who had a negative test result was divided by the total number of patients without CeD. Positive LR was calculated as sensitivity divided by 1- specificity; negative LR was calculated as 1- sensitivity divided by specificity.
Cohen Kappa was used to compare the agreement between Rapid_AntiTG2 and EMA biopsy. Categorical variables were summarized by frequencies and were compared across independent groups with the χ2 or Fisher exact test where appropriate; numerical variables with asymmetrical distribution were summarized by median and interquartile range and compared by the Kruskal-Wallis test. P values were calculated 2-tailed, and a P value <0.05 was considered for significance. Statistical analysis was performed using GraphPad Prism, version 8.2.1.
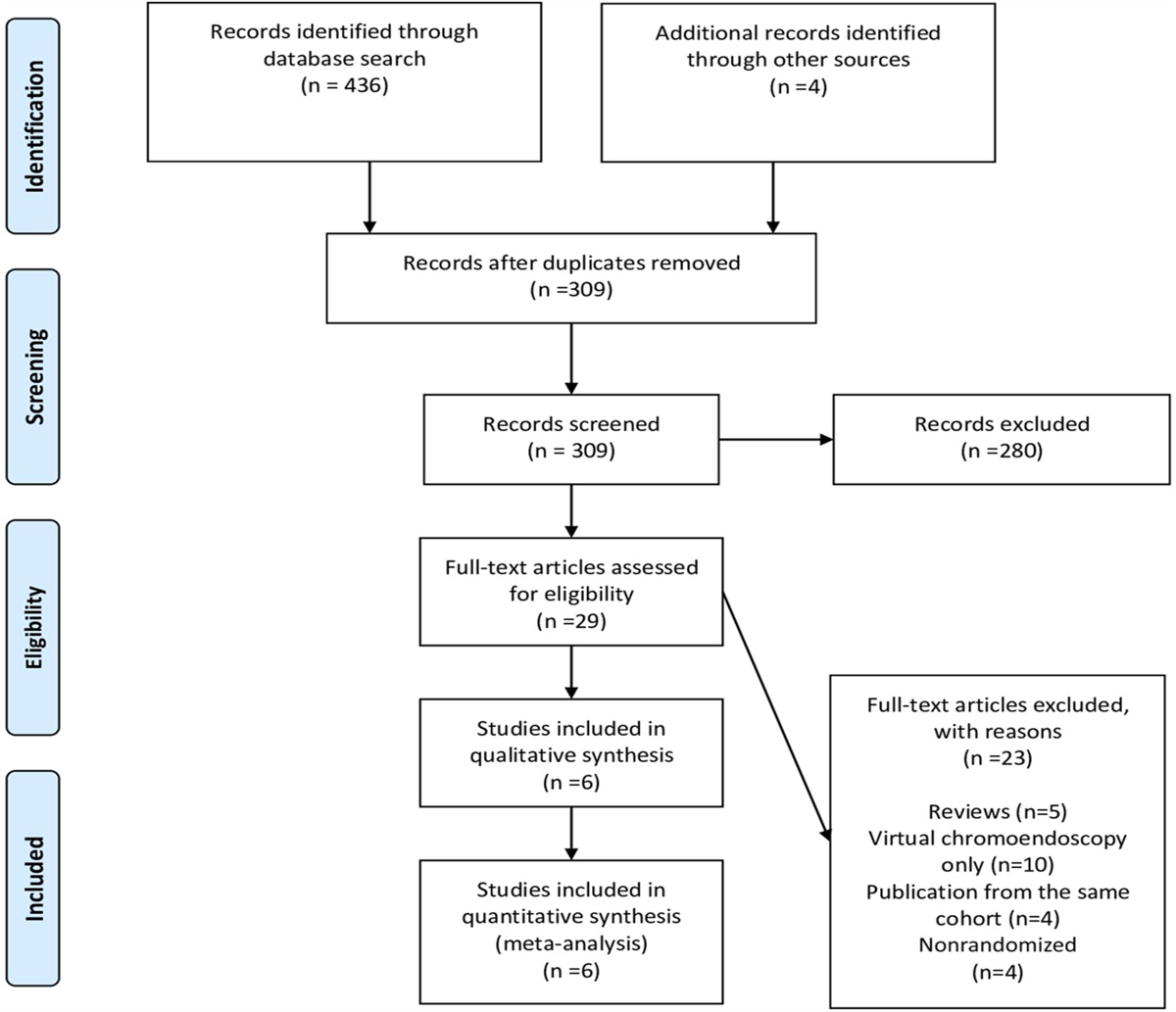
RESULTSBetween July 2020 and January 2022, 213 patients were referred to our Unit for an elective EGD. According to our eligibility criteria, a total of 148 patients were included in the study (Figure 2).
 Figure 2:
Figure 2: Patients' flowchart. GERD, gastro-esophageal reflux disease; GFD, gluten-free diet.
Of the patients included, 79 were diagnosed as those with CeD (64 classical CeD, 13 potential CeD, and 2 seronegative CeD) and 69 patients were identified as controls. The demographic and disease characteristics of patients included in the analysis are reported in Table 1.
 Table 1.:
Table 1.: Demographic and disease characteristics of patients
When considering biopsies both from DB and DD, the Rapid_AntiTG2 test showed positive results in 79 of 79 patients diagnosed as CeD according to current ESPGHAN guidelines, for sensitivity of 100% (95% confidence interval [CI], 94–100). There were 2 false positives among the 69 patients without CeD for specificity 97% (95% CI, 90–100). Of note, one of these patients was reassessed after 6 months and had developed full-blown enteropathy (Marsh 3), had a serology with both anti-TG2 and EMA antibodies positivity and was diagnosed with CeD in the context of an immune dysregulation, polyendocrinopathy, enteropathy, and X-linked syndrome then. The LR+ of Rapid_AntiTG2 was 34.1 (95% CI, 8.7–133.5), whereas the LR− was 0.01 (95% CI, 0.00–0.01), suggesting an excellent predictive ability of the test to identify CeD and its absence.
When the samples from only DB were analyzed, the diagnostic accuracy of Rapid_AntiTG2 remained unchanged (sensitivity 99% and specificity 97%), while in samples from DD, sensitivity dropped to 63% with no change in specificity (97%).
Rapid_AntiTG2 showed a good diagnostic performance also in the subgroups of patients with potential CeD and seronegative CeD. When including biopsies from both DB and DD, the Rapid_AntiTG2 test detected all 13 patients with potential CeD and 2 of 2 patients with seronegative villous atrophy (sensitivity 100%; 95% CI, 78–100).
When considering only samples from DB, the Rapid_AntiTG2 test missed 1 patient with potential CeD (sensitivity 93%; 95% CI, 68–100), while in samples from DD, sensitivity was decreased, identifying only 3 of 13 patients with potential CeD (sensitivity 23%) and 1 of 2 patients with seronegative CeD.
Two patients with CeD and IgA deficiency were included in our cohort, and in both of them, Rapid_AntiTG2 was positive in DB and DD samples. Agreement of Rapid_AntiTG2 with EMA biopsy was almost perfect when considering results from DB + DD and DB alone, as summarized in Table 2. The interoperator agreement in the interpretation of Rapid_AntiTG2 results was 100%.
 Table 2.:
Table 2.: Summary of test results of Rapid_AntiTG2 compared with those of EMA biopsy
In accordance with the ESPGHAN guidelines (2), all patients diagnosed with classical or seronegative CeD were treated with GFD. One patient with seronegative CeD performed a second EGD after 1 year of GFD that showed villous atrophy recovery. The second patient with seronegative CeD has had a resolution of symptoms (severe constipation) after introducing GFD and is awaiting follow-up EGD. For patients diagnosed with potential CeD, treatment was decided on an individual basis, evaluating the presence of gluten-related symptoms and the patients' and families' wishes. Among 13 patients with potential CeD, 7 (53.8%) had gluten-related symptoms and 6 of them started a GFD.
DISCUSSIONIn this study, we found that I-anti-TG2 can be accurately detected using an immunochromatographic assay after simple mechanical lysis of fresh intestinal biopsy samples. In this cohort, the Rapid_AntiTG2 had very high sensitivity and specificity in correctly identifying patients with CeD and had a perfect agreement with the EMA reference test. In addition, although the number of patients was small, its diagnostic accuracy was retained in patients with potential and seronegative CeD and in patients with IgA deficiency, which represents 2%–3% of the CeD population (14).
In those patients who do not meet the criteria for a no-biopsy approach, the diagnosis of CeD relies on a combination of serology and duodenal histopathology showing increased intraepithelial lymphocytes, crypt hyperplasia, and villous atrophy. Despite its high overall accuracy, this diagnostic strategy has some limitations due to several factors. Although serologic markers have excellent sensitivity in the medical literature, their sensitivities often decrease in the real-world clinical setting (15) and, on the contrary, negative serology does not rule out CeD with absolute accuracy due to the possibility of seronegative CeD. Histological confirmation can be challenging: biopsy specimens can be of poor quality and villous atrophy can be patchy (16,17). Although inclusion of biopsy samples from the DB have been shown to increase the sensitivity for villous atrophy identification, and is now recommended in all CeD guidelines, CeD-like mucosal lesions can be found in conditions other than CeD.
I-anti-TG2 are currently not part of the diagnostic approach for the diagnosis of CeD. However, they may be a useful diagnostic marker when conventional serology and histology is inconclusive (18) such as in patients with seronegative villous atrophy in whom I-anti-TG2 identification proved very accurate in separating patients with CeD from controls (12).
Another clinical scenario is that of potential CeD where I-anti-TG2 have very high specificity. One previous observation based on the determination of I-anti-TG2 with the deposits technique has suggested that the presence of I-anti-TG2 can help identify those patients with potential CeD who will progress toward villous atrophy (4). In this study, we identified I-anti-TG2 in all patients with potential CeD using Rapid_AntiTG2.
This observation might suggest higher sensitivity of the technique used here or be a consequence of the fact that we systematically analyzed both the proximal and the DD in each patient, thus maximizing the detection rate of I-anti-TG2. However, additional long-term follow-up studies are needed to clarify whether baseline I-anti-TG2 can differentiate between potential CeD who will evolve to full-blown CeD vs those who will not.
Of interest, the sensitivity of the Rapid_AntiTG2 test was greater in specimens collected from the DB than in those from the DD. This discrepancy was also observed with the EMA biopsy in this study and in previous studies of our group with the deposit technique (19), which could suggest a higher concentration of I-anti-TG2 in the DB.
According to our results, the Rapid_AntiTG2 could add strength to histology, and intestinal specimens for CeD diagnosis could be taken only from the DB, reducing the number of intestinal biopsy samples to be analyzed.
Currently, the investigation of I-anti-TG2 is limited to a few research centers because the techniques for their detection are complex. With the deposit technique, the biopsy sample needs to be cut with a cryotome, a double indirect immunofluorescence is then performed, and IgA anti-TG2 deposits appear as yellow spots below the basement membrane, along the villous and the crypt, and around mucosal vessels. The interpretation of results with the deposit technique is highly dependent on the experience of the operator. The EMA biopsy technique is easier to perform, although it requires trained personnel and it remains confined to few laboratories (19).
The reliability and usefulness of immunochromatography has been previously reported for the detection of I-anti-TG2 in the supernatant of cultured biopsies (20). In this study, we further simplified the procedure by performing a mechanical disruption of the biopsy, thus avoiding culture. With this technique, the test could be performed in the endoscopy room, with a low cost (the cost per test is around 10 vs 100 euros for the EMA biopsy), and results would be available in a few minutes, right at the end of the endoscopy session. Having a simple method for the detection of I-anti-TG2 that is easy to perform would result in the examination being used more frequently in clinical practice. This would mean that the test would be widely available to help in cases of suspected CeD that are difficult to classify. In addition, its easy implementation would allow to design and conduct multisite clinical studies with adequate power to elucidate the prognostic value of I-anti-TG2 in the setting of potential CeD.
A future improvement of the test could be a device able to read the intensity of the test line on the membrane of the cassette to provide a clear answer as test output.
We acknowledge that the number of patients with seronegative CeD and CeD potential in this cohort is small, limiting the interpretation of results and that larger multicenter studies are needed to truly assess the diagnostic accuracy of Rapid_AntiTG2 in these specific populations and demonstrate the applicability of this test in routine CeD diagnostics.
A major strength of the study lies in its design. To avoid potential bias on test accuracy that could have limited the generalizability of the results, the sample size was calculated by anticipating a high prevalence of CeD in a population of children and adolescents referred to a tertiary care pediatric gastroenterology center for an EGD procedure. Moreover, likelihood ratios were preferred over predictive values as a measure of test accuracy because these measures are not affected by changes in disease prevalence.
Intestinal anti-TG2 can be detected in the supernatant obtained after simple mechanical lysis of fresh intestinal biopsy, using an immunochromatographic test (Rapid_AntiTG2), without the need for biopsy culturing. In this observation, the Rapid_AntiTG2 test has very high sensitivity and specificity, and a single biopsy from the DB may be sufficient. If these observations are confirmed, it could be used for an easy and fast detection of I-anti-TG2, with a diagnostic result already available at the end of the endoscopy session.
CONFLICTS OF INTERESTGuarantor of the article: Luigina De Leo, PhD.
Specific author contributions: S.L. coordinated and supervised data collection, drafted the initial manuscript, and reviewed and revised the manuscript. L.D.L., F.Z., B.G., and V.G. collected data, conducted the analyses and interpretation of data, and reviewed and revised the manuscript. M.G. analyzed data and performed statistical analysis. L.D.L. and M.B. performed endoscopy procedures in the study and critically reviewed the manuscript for important intellectual content. T.N., G.D.L., and S.L. conceptualized and designed the study and critically reviewed the manuscript for important intellectual content. V.V. analyzed for histopathology the tissue samples from patients included in the study and critically reviewed the manuscript for important intellectual content. All authors approved the final manuscript as submitted and agree to be accountable for all aspects of the work.
Financial support: This work was supported by the Ministry of Health (Rome, Italy) in collaboration with the Institute for Maternal and Child Health IRCCS Burlo Garofolo (Trieste, Italy) with grant RC34/20.
Potential competing interests: None to report.
Study Highlights
WHAT IS KNOWN ✓ Intestinal antitransglutaminase 2 antibodies are a marker of celiac disease and can be helpful in the diagnosis of equivocal cases. ✓ Their use in clinical practice is limited because they require experienced operators and equipped laboratories. WHAT IS NEW HERE ✓ We evaluated the diagnostic accuracy of a rapid immunochromatographic assay to detect intestinal antitransglutaminase 2 antibodies directly on fresh biopsy specimens. ✓ This rapid test has very high diagnostic accuracy, also in cases of potential or seronegative celiac disease. ACKNOWLEDGMENTSWe thank Eurospital Spa for providing the immunochromatography cassette at no cost. We specify that the company had no role in the design of this study and was not involved in its execution, analyses, interpretation of the data, or decision to submit results. Figure 1 was created with Biorender.com.
REFERENCES 1. Lebwohl B, Sanders DS, Green PHR. Coeliac disease. Lancet 2018;391(10115):70–81. 2. Husby S, Koletzko S, Korponay-Szabò I, et al. European society paediatric gastroenterology, hepatology and nutrition guidelines for diagnosing coeliac disease 2020. J Pediatr Gastroenterol Nutr 2020;70(1):141–56. 3. Auricchio R, Mandile R, Del Vecchio MR, et al. Progression of celiac disease in children with antibodies against tissue transglutaminase and normal duodenal architecture. Gastroenterology 2019;157(2):413–20.e3. 4. Tosco A, Salvati VM, Auricchio R, et al. Natural history of potential celiac disease in children. Clin Gastroenterol Hepatol 2011;9(4):320–5. 5. Maglio M, Troncone R. Intestinal anti-tissue Transglutaminase2 autoantibodies: Pathogenic and clinical implications for celiac disease. Front Nutr 2020;7:73. 6. Not T, Ziberna F, Vatta S, et al. Cryptic genetic gluten intolerance revealed by intestinal antitransglutaminase antibodies and response to gluten-free diet. Gut 2011;60(11):1487–93. 7. Tosco A, Aitoro R, Auricchio R, et al. Intestinal anti-tissue transglutaminase antibodies in potential coeliac disease. Clin Exp Immunol 2012;171(1):69–75. 8. Korponay-Szabó IR, Halttunen T, Szalai Z, et al. In vivo targeting of intestinal and extraintestinal transglutaminase 2 by coeliac autoantibodies. Gut 2004;53(5):641–8. 9. Carroccio A, Di Prima L, Pirrone G, et al. Anti-transglutaminase antibody assay of the culture medium of intestinal biopsy specimens can improve the accuracy of celiac disease diagnosis. Clin Chem 2006;52(6):1175–80. 10. De Leo L, Bramuzzo M, Ziberna F, et al. Diagnostic accuracy and applicability of intestinal auto-antibodies in the wide clinical spectrum of coeliac disease. EBioMedicine 2020;51:102567. 11. Picarelli A, Di Tola M, Sabbatella L, et al. Usefulness of the organ culture system in the in vitro diagnosis of coeliac disease: A multicentre study. Scand J Gastroenterogy 2006;41(2):186–90. 12. Taavela J, Popp A, Korponay-szabo IR, et al. A prospective study on the usefulness of duodenal bulb biopsies in celiac disease diagnosis in children: Urging caution. Am J Gastroenterol 2016;111(1):124–33. 13. Carley S, Dosman S, Jones SR, Harrison M. Simple nomograms to calculate sample size in diagnostic studies. Emerg Med J 2005;22(3):180–1. 14. Pallav K, Xu H, Leffler DA, et al. Immunoglobulin A deficiency in celiac disease in the United States. J Gastroenterol Hepatol 2016;31(1):133–7. 15. Leffler DA, Schuppan D. Update on serologic testing in celiac disease. Am J Gastroenterol 2010;105(12):2520–4. 16. Scott BB, Losowsky MS. Patchiness and duodenal-jejunal variation of the mucosal abnormality in coeliac disease and dermatitis herpetiformis. Gut 1976;17(12):984–92. 17. Goldstein NS. Non-gluten sensitivity-related small bowel villous flattening with increased intraepithelial lymphocytes: Not all that flattens is celiac sprue. Am J Clin Pathol 2004;121(4):546–50. 18. Salmi TT, Collin P, Reunala T, et al. Diagnostic methods beyond conventional histology in coeliac disease diagnosis. Dig Liver Dis 2010;42(1):28–32. 19. De Leo L, Villanacci V, Ziberna F, et al. Immunohistologic analysis of the duodenal bulb: A new method for celiac disease diagnosis in children. Gastrointest Endosc 2018;88(3):521–6. 20. Di Tola M, Marino M, Casale R, et al. One-step immunochromatographic visual assay for anti-transglutaminase detection in organ culture system: An easy and prompt method to simplify the in vitro diagnosis of celiac disease. J Clin Lab Anal 2018;32(1):e22195.
留言 (0)