
記住我
Colorectal cancer refers to a development of malignancy occurring within the digestive system. According to the latest statistics acquired from the International Agency for Research on Cancer, colorectal cancer was the third most common form of cancer in 2020, with approximately. 1.93 million new cases of colorectal cancer and a total of 930,000 deaths recorded worldwide. Subsequently, colorectal cancer has risen to be the second leading cause of cancer death in the world.1 Following the diagnosis of colorectal cancer, numerous patients require colostomy or ileostomy when undergoing surgery, which may be either temporary or permanent.2 Further, nearly 1 million patients with permanent colostomy have been recorded in China, with an estimated 100,000 new patients each year, signifying a rapidly rising trend in the application of these procedures.3
The benefits of colostomy or ileostomy include a significantly prolonged survival period for the patient. However, because this surgical procedure definitively alters the patient’s defecation method and associated lifestyle behaviors, it can result in damage to the patient’s self-image, emotional processing, physical health, and overall quality of life (QoL).4,5 Patients with permanent colostomy experience lifelong involuntary bowel movements, exposure of the intestinal mucosa, fecal leakage, and unpleasant odors.6 Moreover, 70% of patients with ostomies develop complications such as stoma infection, bleeding, and stricture due to improper stoma care.7 Research has shown that patients with ostomies feel anxious, panicked, helpless, and stressed to the extent that they are reluctant to participate in normal social activities.8,9
Nursing staff play an important role in patient recovery. However, patients are often hospitalized for only 1 week following stoma surgery, and many patients are not proficient in the necessary knowledge and skills for colostomy self-care. As emphasized in the 2020 World Council of Enterostomal Therapists international ostomy guide, the role of enterostomal nurses should be to engage in patient follow-up and education and serve as part of the interprofessional team.10
Many patients experience complications because of improper stoma care, such as stoma infection, bleeding, and stenosis.11,12 As an extension and continuation of inpatient care, the continuous care model can provide long-term care guidance for patients with a colostomy or ileostomy, thereby assisting patients in confidently reintegrating into society faster after discharge and subsequently achieving a better QoL.13
In this study, the authors carried out online stoma nursing training to explore the effect of continuous nursing on reducing ostomy complications, improving patients’ self-care ability, and improving patients’ anxiety and QoL.
METHODS DesignThis cross-sectional study was carried out between May and October 2021 and is reported based on the STROBE (STrengthening the Reporting of OBservational studies in Epidemiology) checklist.
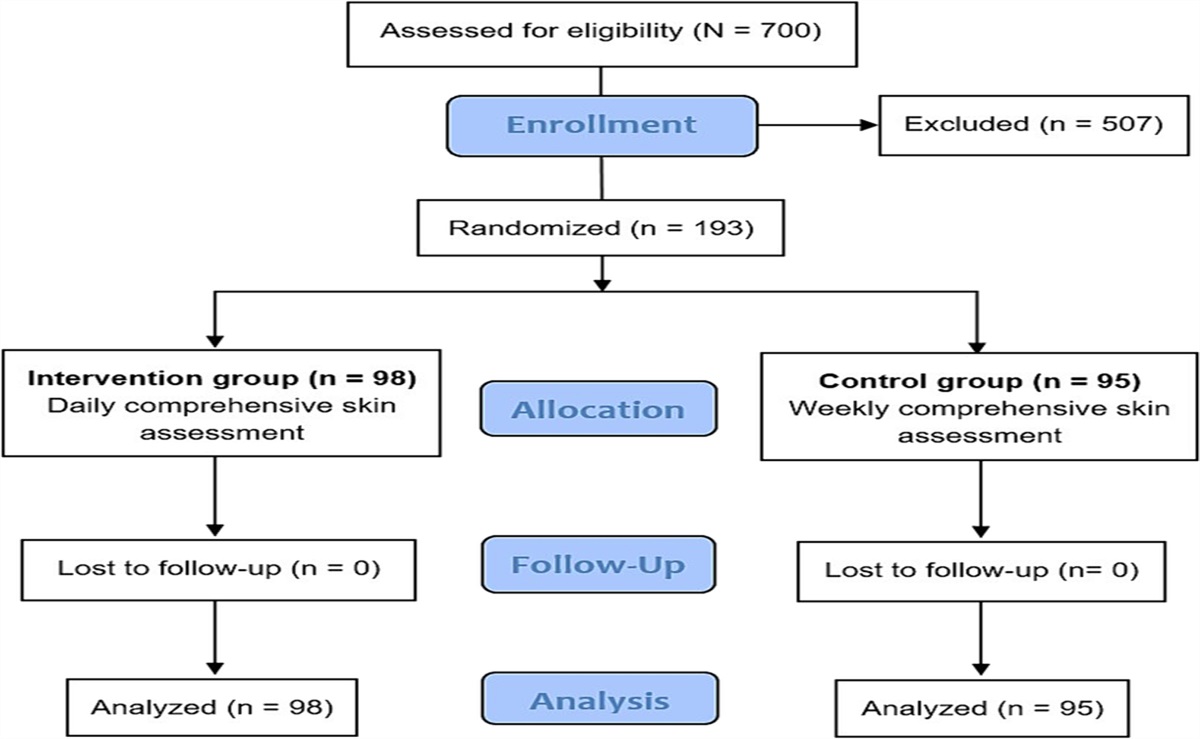
ParticipantsResearchers recruited a total of 100 patients who underwent colostomy or ileostomy procedure in the Department of Colorectal Surgery at Harbin Medical University Cancer Hospital. The participants were randomly divided into two groups according to their surgery date, with 50 participants in the experimental group and 50 participants in the control group.
The inclusion criteria were: (1) patients were diagnosed with colorectal cancer and underwent colostomy or ileostomy; (2) age 18 years or older; (3) no tumor recurrence or metastasis; (4) signed informed consent form agreeing to participate and complete the questionnaires; and (5) voluntary participation in the colostomy or ileostomy nursing training according to the schedule. Participants were excluded if they had severe heart, liver, kidney, or other organ dysfunction or blood and immune system diseases; had a history of mental illness, difficulty in communication or comprehension, or dyslexia; had intestinal obstruction or perineal and abdominal incision infection; or had high-output stomas.
Control Versus Experimental GroupsThe control group received standardized routine care, including health guidance upon discharge, regular hospital visits, and routine follow-up by telephone. The experimental group received the same treatment but also used WeChat, Tencent QQ, and Tencent conference software (Tencent Technology Co Ltd) to carry out continuous nursing training. Both the control group and the experimental group were followed up with regular telephone calls once a week; both groups completed the relevant questionnaires 1 week after discharge and again at 3 months postdischarge.
Continuous Nursing CareThe investigators established a continuous care nursing team that consisted of one deputy chief physician of colorectal surgery, one chief nurse, two chief nurses who had obtained a title certificate, and three nurses. Specific subjects in the patient training content included the identification and prevention of colorectal cancer stoma complications, guidance on the process of changing colostomy or ileostomy bags and selecting stoma products, health education, and psychological counseling and communication skills for patients after colostomy or ileostomy.
The implementation of continuous care was threefold.
Investigators established WeChat and QQ stoma exchange groups. The continuous care nursing team encouraged patients and their families to post daily self-care methods and photographs or videos of existing problems to the group. Patients were also encouraged to communicate with each other to relieve psychological pressure. The nursing team reviewed the questions raised during patient care every week, answered patients’ questions at a designated time, and provided guidance on appropriate treatment methods. The continuous care nursing team held a video call once a month to monitor and understand changes in the patient’s psychological and emotional state to provide timely psychological counseling, correct bad living habits, suggest improved exercise methods, and offer personalized nursing guidance according to the patient’s recovery phase. The team invited patients and their families to participate in video lectures every month. These presentations described the latest progress in colostomy- or ileostomy-related treatment and the use of new ostomy products and related introductions. The team aimed to closely track the recovery of discharged patients. They organized online stoma nursing operation skills competitions; answered vital questions regarding the daily nursing of patients; and informed patients of relevant nursing precautions, such as regular cleaning, avoiding excessive cleaning, and emergency treatment of complications. Investigators set up a public account and published nursing materials every day, including correct chassis and pouch replacement operation videos after colostomy or ileostomy, daily dietary guidance, swimming and other exercise guidance, bathing guidance, inspirational videos, humorous jokes, successful self-care experiences, and social and sexual knowledge. With these posts, the investigators aimed to help alleviate patients’ nervousness and anxiety, build self-confidence, and help them return to family and social life. Instruments Basic Information Scale for Colostomy or Ileostomy PatientsResearchers extracted the following information from patients’ medical records: age, sex, educational attainment, occupation, family monthly income, medical insurance, and site of stoma.
Stoma Care Self-efficacy ScalePatients’ self-efficacy was measured using the Stoma Care Self-efficacy Scale. Created by Bekkers and colleagues14 in 1996, the scale contains 28 items and two dimensions. All items are rated on a 1- to 5-point Likert-type scale (1 = not confident, 2 = somewhat confident, 3 = confident, 4 = more confident, 5 = very confident), with total scores ranging from 28 to 140. Based on the scores obtained, patients were classified as one of the following three levels: low self-efficacy level (score of 65 points or lower), moderate level of self-efficacy (66 to 102 points), and high self-efficacy (103 points or higher).
Exercise of Self-care Agency Scale (ESCA)Researchers used this scale developed by Yamashita15 to assess patients’ self-care ability before and after treatment. The ESCA scale includes four dimensions: self-care responsibility, self-concept, health knowledge, and nursing skills. It contains 43 items and has a total possible score of 172 points. The higher the score, the better the patient’s self-care ability.
State-Trait Anxiety Inventory (STAI)Investigators used the STAI to assess the mental status of patients before and after the intervention. The questionnaire contains 40 items to measure transient and persistent anxiety levels.16 The scale contains 20 items of STAI state anxiety and 20 items of STAI trait anxiety. All items are rated on a 4-point Likert-type scale (1 = minor, 2 = several, 3 = moderate, and 4 = almost always). Some questions are scored in reverse. The higher the score, the more anxious the patient.
Short Form-36 Health Survey Questionnaire (SF-36)This scale is the world’s most widely used QoL assessment tool. It was developed by the Boston Health Research Institute to assess the QoL of patients before and after an intervention.17 The SF-36 contains 36 items across eight dimensions: physical functioning, role-body, physical pain, social functioning, mental health, role-emotion, vitality, and general health.17 The score for each dimension is rated between 0 and 100. The higher the score, the better the QoL. In the present study, the authors evaluated four of the dimensions: physiologic function, vitality, social ability, and mental health.
Postoperative ComplicationsThe incidence of complications within 3 months after discharge was collected through the hospital medical record follow-up system and compared for both patient groups.
Statistical AnalysisData were analyzed using Excel software (Microsoft Inc) and SPSS 26.0 (IBM Corp). The enumeration data were compared using a t test, the measurement data results were expressed as percentages, and the χ2 test was used for comparison. P < .05 indicates statistical significance.
Ethical ConsiderationsThis study was approved by the Research Ethics Committee of the Harbin Medical University Cancer Hospital. The study was conducted in accordance with the Declaration of Helsinki.
RESULTS Patients’ Clinical CharacteristicsPatients in the control group versus the experimental group differed only in their type of medical payment (P < .0001); no other baseline characteristics differed between groups (P > 0.05; Table 1).
Table 1 - PATIENT CHARACTERISTICS Characteristics Control Group (n = 50), n Experimental Group (n = 50), n Cramer V χ 2 P Age, y 0.218 4.744 .093 ≤40 3 0 40–60 22 17 ≥60 25 33 Sex 0.144 2.060 .151 Men 34 27 Women 16 23 Educational attainment 0.137 1.873 .392 Primary school and below 15 16 Junior high school 17 22 High school and above 18 12 Occupation 0.212 4.500 .212 Worker 8 2 Famer 12 12 Other 13 13 Retiree 17 23 Patient medical insurance, CNY ¥ 0.132 1.743 .418 2,001–3,000 2 1 3,001–4,000 15 21 >4,000 33 28 Medical payment type 0.491 24.136 .000 New rural cooperative medical system 7 13 Medical insurance for urban residents 3 1 Municipal medical insurance 15 8 Municipal urban and rural medical insurance 3 4 Medical insurance settled in different places in the province 21 8 At one's own expense 1 16 Site of stoma 0.289 8.331 .080 Small intestine 16 9 Descending colon 2 2 Sigmoid colon 22 34 Ileum 8 2 Transverse colon 2 3Patients who received continuing care recorded higher self-efficacy scores at both 1 week and 3 months postdischarge compared with the control group (Table 2). Both groups increased in self-efficacy over time, with higher mean self-efficacy scores recorded at 3 months postdischarge in comparison with 1 week postdischarge. Further, the continuing care group experienced a greater gain in self-efficacy as measured by their self-efficacy scores at 1 week versus 3 months postdischarge. Between-group difference in scores at 3 months postdischarge (P < .0001) was significantly higher than it was at 1 week postdischarge (P = .029).
Table 2 - BETWEEN-GROUP COMPARISON OF STOMA CARE SELF-EFFICACY Time Control Group (n = 50), Mean (SD) Experimental Group (n = 50), Mean (SD) t df P 1 wk postdischarge 75.34 (7.466) 78.34 (5.999) −2.215 98 .029 3 mo postdischarge 83.60 (10.473) 114.46 (11.427) −14.078 98 .000Compared with patients in the control group, the patients who received continuous nursing had a higher mean self-care responsibility score 1 week after discharge (P = .030), thus exhibiting a stronger sense of self-care responsibility (Table 3). At 3 months postintervention, the ESCA scores of both groups of patients were higher than the scores recorded at 1 week after discharge. However, the ESCA scores of the continuous care group were significantly higher than those of the control group for all four dimensions of the scale (all Ps < .0001, Table 3).
Table 3 - COMPARISON OF EXERCISE OF SELF-CARE AGENCY SCALE Variable Control Group (n = 50), Mean (SD) Experimental Group (n = 50), Mean (SD) t df P Concept of self-care 1 wk postdischarge 21.46 (2.735) 22.06 (1.889) −1.277 98 .205 3 mo postdischarge 25.14 (1.830) 30.98 (2.653) −12.813 98 .000 Self-care skills 1 wk postdischarge 21.92 (2.506) 22.30 (2.384) −0.777 98 .439 3 mo postdischarge 32.00 (2.864) 36.26 (2.554) −7.849 98 .000 Knowledge of self-care 1 wk postdischarge 25.70 (2.234) 25.80 (2.157) −0.228 98 .820 3 mo postdischarge 34.42 (2.524) 38.46 (2.215) −8.507 98 .000 Responsibility for self-care 1 wk postdischarge 20.58 (2.331) 21.56 (2.111) −2.204 98 .030 3 mo postdischarge 27.84 (2.014) 33.18 (2.593) −11.502 98 .000Significant between-group differences in state anxiety and trait anxiety as measured by the STAI occurred at both 1 week and 3 months postdischarge (all Ps < .0001). Compared with patients in the control group, patients receiving continuous care had significantly lower mean STAI scores, indicating lower levels of anxiety (Table 4).
Table 4 - COMPARISON OF STATE-TRAIT ANXIETY INVENTORY (STAI) Variable Control Group (n = 50), Mean (SD) Experimental Group (n = 50), Mean (SD) t df P STAI state anxiety 1 wk postdischarge 60.24 (4.187) 49.02 (3.755) 14.106 98 .000 3 mo postdischarge 44.36 (2.855) 29.28 (3.648) 23.018 98 .000 STAI trait anxiety 1 wk postdischarge 64.86 (4.481) 54.44 (4.190) 12.01 98 .000 3 mo postdischarge 49.54 (3.144) 34.22 (3.616) 22.608 98 .000At 1 week postdischarge, patients in the continuous care group scored significantly higher on the mental health dimension of the SF-36 in comparison with the control group (P < .0001). At 3 months after discharge, both groups’ scores had increased across all four QoL dimensions evaluated in this study (physical function, mental health, vitality, and social function). However, the continuous care group scored higher than the control group on all four dimensions (Ps < .0001; Table 5).
Table 5 - BETWEEN-GROUP COMPARISON OF SHORT FORM-36 HEALTH SURVEY QUESTIONNAIRE Variable Control Group (n = 50), Mean (SD) Experimental Group (n = 50), Mean (SD) t df P Physical functioning 1 wk postdischarge 59.62 (3.994) 60.30 (3.099) −0.951 98 .344 3 mo postdischarge 66.14 (2.673) 70.84 (2.992) −8.284 98 .000 Mental health 1 wk postdischarge 53.12 (1.803) 54.12 (2.106) −4.489 98 .000 3 mo postdischarge 60.48 (3.183) 65.26 (3.231) −7.452 98 .000 Vitality 1 wk postdischarge 25.70 (2.234) 25.80 (2.157) −0.228 98 .820 3 mo postdischarge 34.42 (2.524) 38.46 (2.215) −8.507 98 .000 Social functioning 1 wk postdischarge 42.18 (2.256) 42.96 (2.531) −1.627 98 .107 3 mo postdischarge 52.50 (2.073) 57.00 (2.726) −9.293 98 .000Within 3 months after discharge, the incidence of complications was lower in the continuous nursing group compared with the control group (P < .0001; Table 6).
Table 6 - COMPLICATIONS IN PATIENTS WITH ENTEROSTOMY Complication Control Group (n = 50), n (%) Experimental Group (n = 50), n (%) χ 2 P Irritant dermatitis 15 (30) 6 (12) Allergic dermatitis 11 (22) 4 (8) Fecal dermatitis 5 (10) 3 (6) Avulsive dermatitis 2 (4) 2 (4) Mucosal separation 2 (4) 1 (2) Total occurrence 35 (70) 16 (32) 14.446 .000Colostomy or ileostomy necessitates that patients make lifestyle changes, which usually require professional nursing guidance alongside a long period of adaptation. Because routine discharge guidance does not provide patients with real-time, specific nursing guidance, it therefore has certain limitations. Social media platforms have become the main channels for continuous care processes.18 The continuous nursing model has changed the previous mode of passive nursing education.19 The present findings suggest that continuity in care and availability of information can assist patients in reducing negative emotions and improving self-care and self-efficacy, leading to fewer complications and ultimately a better QoL.
For assessing self-care ability in patients with ostomies, social confidence, competence, and self-efficiency play an important role.20 Patients with high self-efficacy tend to be more confident in their self-management. In accordance with previous research,21 the present results show that at both 1 week and 3 months after discharge, patients who received continuing care demonstrated higher levels of self-efficacy in comparison with the control group. Continuous nursing intervention based on online platforms, including the organization of online video lectures and ostomy operation skills competitions, helped establish a positive, trusting relationship between the nursing staff and the patients. The program has greatly improved patients’ enthusiasm for participating and has enhanced patients’ initiative in improving their overall self-sufficiency.
The ESCA score reflects patient’s level of willingness to participate in self-care and nursing knowledge after returning to society and family. The continuous nursing model improves patients’ self-care ability and helps them integrate into society as soon as possible.22,23 The present study found no difference in the self-care ability of the experimental group and the control group at 1 week postdischarge. However, at 3 months after the intervention, the experimental group had significantly greater self-care ability in comparison with the control group. In the early stage after discharge, patients lack stoma nursing skills and relevant knowledge, so the postdischarge nursing plan mainly depends on the assistance of family members. The continuous nursing model based on the internet platform effectively improved patients’ understanding of self-care and their sense of responsibility by providing nursing-related videos and promoting communication between patients without being limited by time or location. These benefits effectively allow for the mastering of stoma nursing-related knowledge, resulting in an overall improvement of patients’ self-care skills.
Studies have shown that the therapeutic effect of a colostomy or ileostomy is closely related to the patient’s mood and subjective well-being.24 A continuing care model could assist nurses in providing much-needed psychological support to patients undergoing surgery.25 In this study, the two groups of patients showed significant differences in both dimensions of the STAI anxiety score at 1 week and 3 months postdischarge. The patients in the experimental group had lower scores, indicating that the continuous nursing model helps provide patients with timely and effective psychological counseling, reduce stigma, and ease anxiety, thereby helping patients regain self-confidence, face life optimistically, reduce psychological pressure, avoid feelings of inferiority, and reduce interference with normal social activities as a result of the ostomy.
Continuous nursing can assist patients in establishing a comprehensive and effective self-management system after discharge. With continuous nursing care, patients receive health guidance and nursing interventions at each stage of recovery, optimizing patients’ physical, psychological, and social functions to significantly improve the patient’s QoL.26,27 In the present study, QoL scores on the four dimensions of physical function, mental health, life vitality, and social function were significantly higher in the continuous nursing group than in the control group at both 1 week and 3 months after discharge. Patients’ reported QoL often depends on the standardized level of care that they receive. These results show that the continuous nursing model can improve communication between patients and their families, as well as between patients or their families and medical staff through WeChat and QQ groups. The model further assists patients in establishing appropriate eating habits and dressing methods, correcting bad health habits, improving exercise methods, and so on to improve patients’ QoL after colostomy or ileostomy.
Zhang and colleagues28 found that the rate of complications after colostomy or ileostomy was approximately 20%. The incidence of complications can be used to measure the quality and effectiveness of care postsurgery. Colostomy or ileostomy complications affect patients’ daily lives, limiting their social activities, affecting the relationship between patients and their families, and reducing their QoL.29,30 In this study, the incidence of stoma complications in the experimental group was significantly lower than that in the control group. This may be due to the timely response that the online platform provides. When patients felt unwell, they could communicate online at any time, which increases their access to medical resources and improves the efficiency of treatment. Further, the continuous care provided by an online platform can provide personalized guidance for patients according to their specific conditions, reduce the occurrence of skin complications around the stoma, and enable patients with colorectal cancer to obtain an improved prognosis.
LimitationsLimitations of this study include the small sample size, the lack of comparison among patients in the same group, and the short postoperative observation time. In the prospective follow-up study, the relevant information will be further improved, and the effect of the continuous nursing model will be further explored, specifically with regard to the impact that this treatment can have on a patient’s long-term outcomes.
CONCLUSIONSContinuous nursing can enhance patients’ self-efficacy and self-care ability, reduce patients’ anxiety, reduce the incidence of postoperative complications after colostomy or ileostomy, and improve patients’ QoL. The effectiveness of online nursing training based on virtual platforms such as WeChat, QQ, and Tencent conference software showed specific time dependence. Extending the duration of nursing training pertaining to self-care would better evaluate the benefits of both continuous nursing and routine nursing, while expanding on their differences.
The results of this study highlight the advantages of a continuous nursing model for clinical applications.
It greatly alleviates the shortage of social medical resources and the uneven distribution of medical resources across various regions. It avoids ineffective medical treatment and reduces the economic burden of care. With standard care, when patients experience mild discomfort, they may choose to travel long distances to the hospital for treatment because they are fearful and lack the relevant professional knowledge. This not only increases economic expenses but also may compromise optimal intervention time.
留言 (0)