
記住我
Background: Schizophrenia is associated with increased risk of experiencing interpersonal violence. Little is known about risk specifically around the time of pregnancy.
Methods: This population-based cohort study included all individuals (aged 15–49 yr) listed as female on their health cards who had a singleton birth in Ontario, Canada, between 2004 and 2018. We compared those with and without schizophrenia on their risk of an emergency department (ED) visit for interpersonal violence in pregnancy or within 1 year postpartum. We adjusted relative risks (RRs) for demographics, prepregnancy history of substance use disorder and history of interpersonal violence. In a subcohort analysis, we used linked clinical registry data to evaluate interpersonal violence screening and self-reported interpersonal violence during pregnancy.
Results: We included 1 802 645 pregnant people, 4470 of whom had a diagnosis of schizophrenia. Overall, 137 (3.1%) of those with schizophrenia had a perinatal ED visit for interpersonal violence, compared with 7598 (0.4%) of those without schizophrenia, for an RR of 6.88 (95% confidence interval [CI] 5.66–8.37) and an adjusted RR of 3.44 (95% CI 2.86–4.15). Results were similar when calculated separately for the pregnancy (adjusted RR 3.47, 95% CI 2.68–4.51) period and the first year postpartum (adjusted RR 3.45, 95% CI 2.75–4.33). Pregnant people with schizophrenia were equally likely to be screened for interpersonal violence (74.3% v. 73.8%; adjusted RR 0.99, 95% CI 0.95–1.04), but more likely to self-report it (10.2% v. 2.4%; adjusted RR 3.38, 95% CI 2.61–4.38), compared with those without schizophrenia. Among patients who did not self-report interpersonal violence, schizophrenia was associated with an increased risk for a perinatal ED visit for interpersonal violence (4.0% v. 0.4%; adjusted RR 6.28, 95% CI 3.94–10.00).
Interpretation: Pregnancy and postpartum are periods of higher risk for interpersonal violence among people with schizophrenia compared with those without schizophrenia. Pregnancy is a key period for implementing violence prevention strategies in this population.
Interpersonal violence is defined as the intentional use of force or power against others, including physical, sexual and psychological abuse perpetrated by strangers, acquaintances, family members or intimate partners.1–5 Around the time of pregnancy, interpersonal violence affects not only the person experiencing it, but also the developing fetus or infant.6 Maternal consequences include acute injuries, chronic pain and psychiatric disorders.7,8 Interpersonal violence is also associated with absent or delayed prenatal care, preterm birth, poor fetal growth, difficulties in maternal–child attachment, and maternal, fetal and neonatal death.9–14
Women with schizophrenia are at high risk of experiencing interpersonal violence during their lifetime from known and unknown perpetrators.15–17 The lifetime prevalence of physical or sexual assault in this population is 20.7%, about 9 times the risk of those without serious mental illness.18 Many women with schizophrenia become pregnant, but little is known about their risk of experiencing interpersonal violence around this time.19,20 In 2 small clinical studies, rates of self-reported interpersonal violence in pregnancy were upward of 20%.21,22 However, these studies had no comparator groups without schizophrenia, included only self-reported risk and did not evaluate postpartum risk.
We sought to compare the risk of an emergency department (ED) visit for interpersonal violence during pregnancy and until 1 year postpartum among people with and without schizophrenia in Ontario. We also sought to compare rates of interpersonal violence screening and disclosure in response to screening in these 2 groups, as well as risk for an ED visit for interpersonal violence in pregnancy or within the first year postpartum among those who did not self-report interpersonal violence. The latter question is important given that people with schizophrenia report being concerned that disclosure of any social issues during the perinatal period could possibly lead to undesirable consequences, such as child apprehension.23,24
MethodsStudy design and data sourcesFor this population-based cohort study, we used linked administrative health and clinical registry data from 2004 to 2018 in Ontario, Canada, (population 14.6 million), where physician and hospital services are provided free of charge to residents. We accessed data at ICES, a nonprofit health care research institute in Toronto that maintains deidentified and linked administrative records for all Ontario residents with a valid health card (Appendix 1, Table S1, available at www.cmaj.ca/lookup/doi/10.1503/cmaj.220689/tab-related-content). The ICES databases are complete and valid for demographic information and primary diagnoses in acute care settings.25 These data are also linked with Ontario’s Better Outcomes Registry and Network (BORN), a prescribed registry where providers enter clinical data into the BORN Information System (BIS) in pregnancy.26 The BIS collects data on screening and disclosure of interpersonal violence in pregnancy. Data from BORN (2012–2014) were securely transferred to ICES under a data sharing agreement, with a linkage success rate of 93.1%.26,27
ParticipantsWe considered all people in Ontario identified as female on their health card who were aged 15–49 years and who became pregnant between Apr. 1, 2004, and Mar. 31, 2018. We excluded nonresidents of Ontario and those without a valid health card as we could not accurately link their information across databases. We identified schizophrenia using a previously validated algorithm requiring at least 1 hospital admission or at least 3 outpatient contacts for schizophrenia or a related psychotic disorder (using codes F20, F25 and F29 in the International Statistical Classification of Diseases and Related Health Problems, 10th Revision [ICD-10]) within 3 years of each other from database inception to the index pregnancy (sensitivity 90.1% and specificity 68.0% v. clinical charts in our data sets).28 We did not include those who received diagnoses of schizophrenia during the pregnancy. All remaining pregnancies formed the reference group. For analyses related to screening and self-reported interpersonal violence, we created a subcohort of patients with data linked to the BIS.
OutcomesThe primary outcome was an ED visit for interpersonal violence during pregnancy or from the person’s delivery date to 365 days postpartum, identified using ICD-10 codes X85-Y09 and Y87.1 in any diagnostic field.29 This approach follows the proposed framework from the United States Centers for Disease Control and Prevention for presenting injury data using ICD-10 codes related to external causes of injury.30 A systematic review of these codes in hospital records found that broad groupings of external causes (as our primary outcome is defined) are 85% accurate.31 We were unable to measure whether interpersonal violence was inflicted specifically by an intimate partner or spouse because use of the ICD-10 codes that identify the perpetrator is not mandatory.
Secondary outcomes included screening for interpersonal violence and disclosure of violence in response to screening. In the BIS clinical registry, health care providers (e.g., midwives, obstetricians, primary care providers) are required to ask about “the self-disclosed threat of or actual physical, sexual, psychological, emotional, or financial abuse” and input the results directly into the patient’s standardized provincial antenatal care record form as follows: “asked, with disclosure,” “asked, with no disclosure,” or “unable to ask.”32 Providers may or may not have used a standardized screening tool when screening women for interpersonal violence as part of this process. We considered responses of “asked, with disclosure” or “asked, with no disclosure” as signifying that a participant was screened for interpersonal violence. Those coded as “unable to ask” and those for whom data were missing were recorded as “not screened.” Among those screened, we determined whether interpersonal violence was disclosed (i.e., “asked, with disclosure”).
CovariatesPotential confounders of the relation between schizophrenia and the outcomes were maternal age, parity, neighbourhood income quintile, urban or rural region of residence, and calendar year at the time of the index delivery, as well as maternal substance use disorders and ED visits for interpersonal violence in the 2 years before conception. We considered participants with no postal code to be unstably housed, and therefore assigned them to the lowest income quintile. To describe the cohort, we also recorded nonpsychotic psychiatric diagnoses (including mood disorders and anxiety disorders) and maternal chronic medical conditions (including asthma, congestive heart failure, HIV, hypertension, diabetes, rheumatoid arthritis) present before pregnancy;33,34 however, we did not consider these covariates to be confounders as their development or exacerbation may be a result of ongoing interpersonal violence, and thus may be a proxy for the outcome.35
Statistical analysisWe used modified Poisson regression using generalized estimating equations and robust error variance to account for clustering of pregnancies to estimate relative risks (RRs) and 95% confidence intervals (CIs) for interpersonal violence, comparing patients with and without schizophrenia.36 We adjusted analyses for maternal age, parity, neighbourhood income quintile, region of residence, year of delivery, maternal substance use disorder and ED visits for interpersonal violence that occurred in the 2 years before pregnancy. We modelled missing data as categories, when applicable. We repeated analyses for outcomes occurring in pregnancy and postpartum (up to 365 days postpartum) separately. As a history of interpersonal violence is such a strong determinant of future interpersonal violence,5,37 we conducted additional analyses in which we added an interaction term (schizophrenia × previous interpersonal violence) and another in which we stratified by preconception ED visits for interpersonal violence.
In the BIS subcohort, we used modified Poisson regression to compare groups as to whether they were screened for interpersonal violence in pregnancy and, among those screened, the likelihood of disclosure. Among those who did not disclose interpersonal violence, we compared the risk of an ED visit for interpersonal violence in pregnancy or postpartum between patients with or without schizophrenia, adjusting for the same covariates as the primary models.
Ethics approvalThe use of data in this study was authorized under section 45 of Ontario’s Personal Health Information Protection Act, which does not require review by a research ethics board. The study was therefore exempt from research ethics approval and was approved by the ICES privacy office. Cell sizes less than 6 were not reported in accordance with Ontario privacy regulations.
ResultsThe final sample (n = 1 802 645) comprised 4470 pregnant people with and 1 798 175 without schizophrenia (Appendix 1, Figure S1). Groups were similar in age (mean 30.62 yr v. 30.26 yr) and parity (43.6% v. 43.7% primiparous) (Table 1). Those with schizophrenia were more likely to reside in a lower income neighbourhood (36.5% v. 22.4% in the lowest income quintile), to have comorbid substance use disorders (15.3% v. 1.7%) and to have an ED visit for interpersonal violence in the 2 years before conception (4.8% v. 0.7%) than those without schizophrenia. They were also more likely to have comorbid psychiatric and chronic medical conditions. Characteristics of the BIS subcohort (n = 254 980) were similar (Appendix 1, Table S2).
Table 1:Characteristics of the main cohort of pregnant people with and without schizophrenia in Ontario between Apr. 1, 2004, and Mar. 31, 2018
Overall, 7735 (0.4%) patients had an ED visit for interpersonal violence in the perinatal period. Of these, 294 visits resulted in hospital admission and 8 resulted in death. For both of these outcomes, numbers were fewer than 6 in the schizophrenia group, so we were unable to comparatively analyze risk for ED visits that resulted in hospital admission or death. Overall, risk for an ED visit for interpersonal violence was higher among those with schizophrenia than among those without it (3.06% v. 0.42%; RR 6.88, 95% CI 5.66–8.37). Younger maternal age, living in a lower income quintile, being multiparous, maternal substance use disorders and a history of an ED visit for interpersonal violence in the 2 years before pregnancy all increased the risk for an ED visit for interpersonal violence (Appendix 1, Table S3). After accounting for all of these variables, the adjusted RR for schizophrenia remained high at 3.44 (95% CI 2.86–4.15) (Table 2). Results were similar when pregnancy and the first year postpartum were analyzed separately (Table 2 and Appendix 1, Tables S4 and S5). The interaction term (schizophrenia × previous interpersonal violence) was statisitically significant (p = 0.02). For those with no history of an ED visit for interpersonal violence before conception, results were similar to those of the main analysis (2.5% among patients with schizophrenia v. 0.4% among those without schizophrenia; adjusted RR 4.01, 95% CI 3.26–4.92) (Figure 1). Those with a history of an ED visit for interpersonal violence had high outcome rates (14.1% among patients with schizophrenia v. 7.5% among those without schizophrenia), with a smaller elevation in risk associated with schizophrenia (adjusted RR 1.65, 95% CI 1.11–2.45).
Table 2:Risk of an emergency department visit for interpersonal violence in pregnancy or within 1 year postpartum, comparing patients with or without schizophrenia
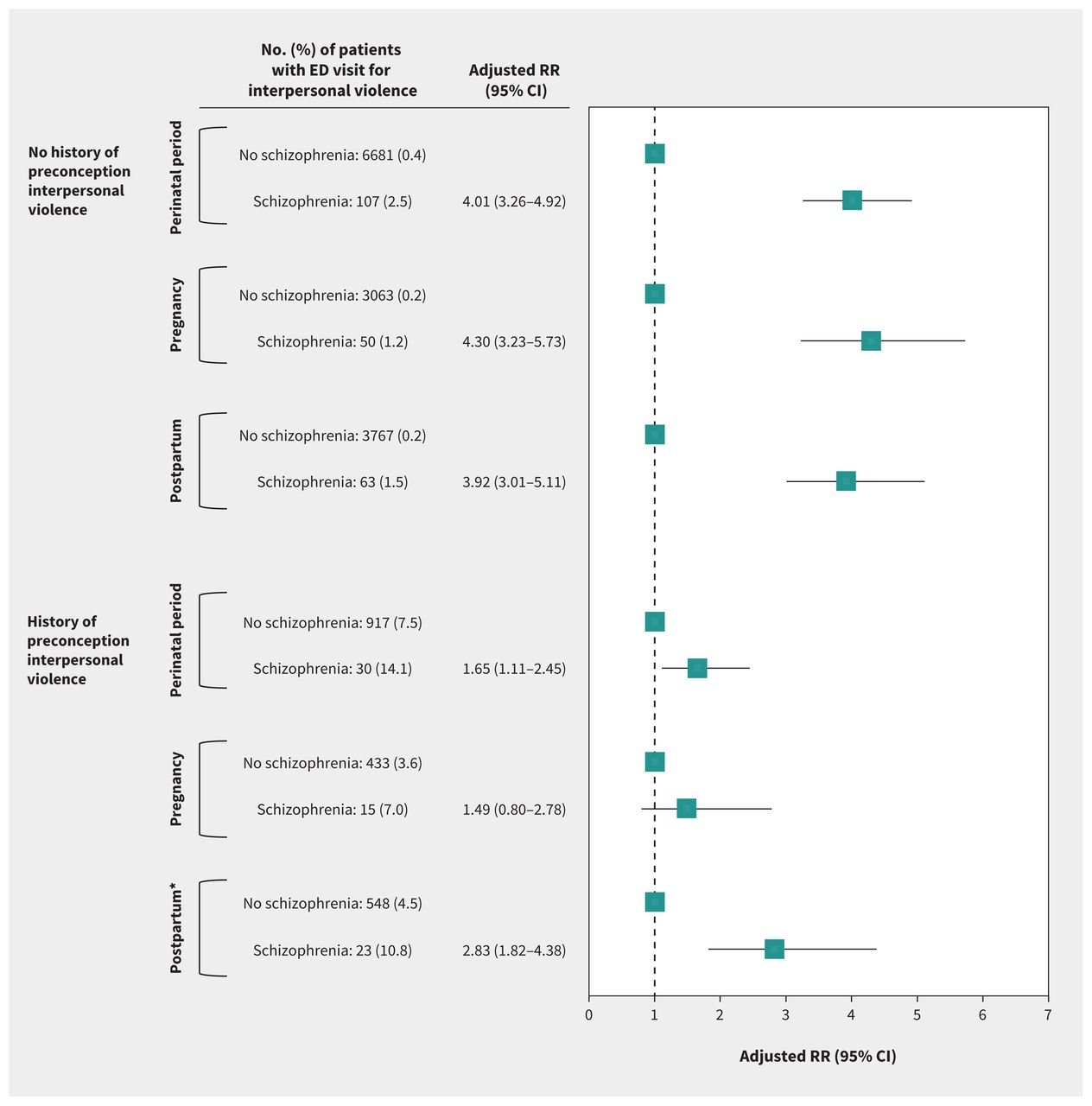 Figure 1:
Figure 1: Risk of interpersonal violence resulting in an emergency department (ED) visit in pregnancy or within 1 yr postpartum, among people with schizophrenia versus those without schizophrenia, further stratified by history of an ED visit for interpersonal violence in the 2 yr before conception. The upper stratum comprises those without a known history of interpersonal violence, and compares 4257 people with schizophrenia to 786 004 people without schizophrenia. The lower stratum comprises those with a known history of interpersonal violence, and compares 213 people with schizophrenia with 12 171 people without schizophrenia. Relative risks were adjusted for maternal age, parity, neighbourhood income quintile, region of residence (urban, rural or missing), year of delivery and maternal substance use disorder, except for the analysis of the postpartum time period among those with a history of interpersonal violence, in which relative risks were adjusted for maternal age, parity, neighbourhood income quintile and region of residence, owing to the small sample size. Note: CI = confidence interval, RR = relative risk.
In the BIS subcohort (n = 254 980, including n = 684 with schizophrenia), 74.3% of patients with schizophrenia were screened for interpersonal violence in pregnancy, which was comparable to 73.8% of those without schizophrenia (adjusted RR 0.99, 95% CI 0.95–1.04). However, those with schizophrenia were more likely to report interpersonal violence when screened (10.6% v. 2.4%; adjusted RR 3.38, 95% CI 2.61–4.38) (Table 3). Among those who did not disclose interpersonal violence, 4.0% of patients with schizophrenia had an ED visit for interpersonal violence during or after pregnancy, compared with 0.4% of those without schizophrenia (adjusted RR 6.28, 95% CI 3.94–10.00) (Table 3).
Table 3:Risk of being screened for interpersonal violence, reporting interpersonal violence and experiencing interpersonal violence that resulted in an ED visit in pregnancy or within 1 year postpartum comparing patients with or without schizophrenia included in the Ontario Better Outcomes Registry and Network Information System
InterpretationIn this population-based study, the risk for an ED visit for interpersonal violence in pregnancy or the postpartum period was threefold higher among those with schizophrenia than among those without schizophrenia. Although those with schizophrenia were just as likely to be screened for interpersonal violence as those without it, they were more than 3 times more likely to report experiencing it. Further, when we combined objective health service use and subjective self-disclosure to provide a more nuanced understanding of violence, schizophrenia was associated with a sixfold increased risk of a perinatal ED visit for interpersonal violence among patients who did not disclose interpersonal violence when screened. Specialized violence prevention, screening and management protocols for pregnant and postpartum patients with schizophrenia are warranted to mitigate this risk.
Our results are consistent with those of 2 single-site studies that quantified risk of intimate partner violence among women with schizophrenia during the perinatal period. In a study of hospital records of 125 pregnant women with schizophrenia who received care at a hospital in western Australia, 22.4% self-reported intimate partner violence during their pregnancy.21 In a second study of 236 pregnant women with schizophrenia spectrum disorders who received care at a psychiatric hospital in London, England, 19.1% self-reported intimate partner violence.22 Although these were not comparative studies, these rates are 3.9 and 2.3 times higher than those reported in the general population in Australia and England, respectively, with relative increases in risk similar to our study.5
We do not know exactly what explains this high relative risk, but people with schizophrenia are disproportionately affected by risk factors for interpersonal violence, including poverty and substance use disorders.5,37 Acute psychosis may result in decreased awareness of personal limits and difficulty with communicating needs and boundaries.38 The cognitive deficits of schizophrenia may reduce a person’s ability to avoid hazardous situations and increase their risk of exploitation by others.39 A qualitative study of staff at domestic violence agencies noted that violent perpetrators specifically targeted individuals with psychiatric conditions who they perceived as more vulnerable.40 Schizophrenia is also associated with social isolation and limited support systems, which may increase vulnerability to entering and remaining in violent relationships.41–43
As rates of routine inquiry about violence among patients with psychiatric disorders are often low,44 it was reassuring that patients with and without schizophrenia were screened for interpersonal violence at a similar rate. These screening questions are part of the standardized form for antenatal care that is used for all pregnant people in Ontario throughout their pregnancy to record their health and health risk factors, a systematic approach to inquiry that may reduce barriers to screening.26 However, barriers to disclosure may disproportionately remain for patients with schizophrenia; we saw high rates of ED visits even among those who did not disclose any interpersonal violence. Research has shown that women with psychiatric disorders often find it difficult to disclose violence during screening for reasons that include fears of violent retaliation from the perpetrator, of not being believed because of their mental illness, and of possible consequences for custody of their child.23,24,44
Although evidence-based guidance to address this specific population’s complex safety needs is limited,43 qualitative studies suggest that positive relationships with health care providers, direct inquiry about violence, a perception that the health care provider is capable of competently responding to disclosure and a confidential setting can facilitate disclosure of interpersonal violence in health care settings.47 Further, best practice is for health care providers to respond to disclosures by conducting an assessment of current risk and offering referral to appropriate services for people experiencing violence, including dedicated shelters, safe housing, safety planning, counselling and legal services.48,49
LimitationsPeople who experienced interpersonal violence but did not present to the ED were not captured. We were unable to determine the perpetrators of the interpersonal violence, although we would expect that a large proportion were known assailants since most violence against pregnant people is by current or former intimate partners. 4,45,46 As is a common limitation of studies using health administrative data, we did not have access to all potential confounders, so we were unable to determine the contribution of key potential factors such as race or ethnicity. Finally, as we did not have access to management plans, we were unable to ascertain clinical management after presentation to the ED for violence or after disclosure of interpersonal violence in pregnancy in the antenatal care setting.
ConclusionWe found that pregnant and postpartum people with schizophrenia are a population at high risk of ED visits for interpersonal violence, suggesting that routine violence screening in antenatal care settings is an important opportunity for intervention to prevent severe physical, psychological and social harm to these patients and their children. Future research is warranted to investigate the specific needs of this population in antenatal care and ED settings, evaluate the effectiveness of different forms of screening and intervention and capture follow-up data in relation to interventions, such as recurrent visits to the ED, injuries and deaths.
AcknowledgementsThe authors thank the Ontario Ministry of Health and the Ontario Ministry of Long-Term Care for their data.
FootnotesCompeting interests: Lucy Barker reports a doctoral award from the Canadian Institutes of Health Research (CIHR). Natasha Saunders reports funding from CIHR and the Ontario Ministry of Health, an honorarium from the BMJ Group (Archives of Diseases in Childhood) and a role on the mental health committee of the Canadian Pediatric Society. Simone Vigod receives royalties from UpToDate and is president-elect (unpaid) for the Marce Society of North America and the Canadian Association for Psychiatric Epidemiology. No other competing interests were declared.
This article has been peer reviewed.
Contributors: Kelly Leslie and Simone Vigod conceived of this work and designed the study. All of the authors contributed to the acquisition, analysis and interpretation of data. Kelly Leslie and Simone Vigod drafted the manuscript. All of the authors revised it critically for important intellectual content, gave final approval of the version to be published and agreed to be accountable for all aspects of the work.
Funding: This study was funded by the Canadian Institutes of Health Research (CIHR PJT-156021). The funder had no role in the design or conduct of the study, or interpretation of the findings.
Data sharing: The data set from this study is held securely in coded form at ICES. Although legal data sharing agreements between ICES and data providers (e.g., health care organizations and government) prohibit ICES from making the data set publicly available, access may be granted to those who meet prespecified criteria for confidential access, available at www.ices.on.ca/DAS (email: dasices.on. ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimer: This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). The opinions, results and conclusions reported in this paper are those of the authors and are independent from the funding sources. No endorsement by ICES or the Ontario MOH or MLTC is intended or should be inferred. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI). However, the analyses, conclusions, opinions and statements expressed herein are those of the authors and not necessarily those of the CIHI. This study is based in part on data provided by Better Outcomes Registry and Network (BORN), part of the Children’s Hospital of Eastern Ontario. The interpretation and conclusions contained herein do not necessarily represent those of BORN Ontario.
Accepted November 28, 2022.This is an Open Access article distributed in accordance with the terms of the Creative Commons Attribution (CC BY-NC-ND 4.0) licence, which permits use, distribution and reproduction in any medium, provided that the original publication is properly cited, the use is noncommercial (i.e., research or educational use), and no modifications or adaptations are made. See: https://creativecommons.org/licenses/by-nc-nd/4.0/
留言 (0)