
記住我



Panic disorder (PD) is characterized as one of the common types of anxiety disorders that affect at least 5% of the global population at any point of their lifetime (Roy-Byrne et al., 2006). Besides, PD has known pathological connections with increased predispositions to cardiovascular diseases and associated deaths (Albert et al., 2005; Smoller et al., 2007), which can extremize the suffering and economic burden of patients and their caregivers (Greenberg et al., 1999). Therefore, revealing the etiopathological factors and strategizing targeted treatment options are urgently required for this disorder.
In preclinical studies, conditional deletions of mutant brain-derived neurotrophic factor (BDNF) variants in response to stress-inducing environmental or physiological stimuli, such as anxiety, have been linked to hyperactivity in the experimental animal model (Rios et al., 2001). In the clinical examination, serum concentrations of BDNF are significantly higher in PD patients compared with age-matched healthy control subjects and are found to be associated with high levels of anxiety susceptibility and sensitivity, symptomatic severity, and poor clinical outcomes, as well (Karege et al., 2002; Shimizu et al., 2005; Ströhle et al., 2010; Kurita et al., 2012), suggesting that the BDNF gene products may have etiological linkage to PD crisis. The reduced BDNF activity in PD has been correlated with a single-nucleotide polymorphism (SNP) at Val66Met of exon XIII, resulting in a G (Val) to A (Met) substitution in the coding sequence of the exon XIII, which may impact the structure-function relationship of the BDNF protein, contributing to the susceptibility of several neuropsychiatric disorders, including PD (Egan et al., 2003a; Chen et al., 2004; Zhao et al., 2015; Chen et al., 2017).
Although the correlation of BDNF Val66Met with PD onset and aggressiveness has been explored in subjects from a wide range of ethnic backgrounds; however, these findings are inconsistent or inconclusive due to multiple confounding factors such as different ethnic backgrounds, small sample sizes, and inconsistent sampling strategies. To overcome these shortcomings, we conducted a meta-analysis testifying to the correlative strength of BDNF SNPs with PD susceptibility.
Methods Search strategywe used full-text searching of the terms “Panic Disorder(PD)” OR “Panic Attacks” AND “brain-derived neurotrophic factor (BDNF)” OR “Brain-derived neurotrophic factor” OR “BDNF” and “Val66Met” OR “G196A” OR “rs6265.” Databases/online libraries mainly used for searching articles were PubMed, Medline, Web of Science, APA, Cochrane, and Embase. The search deadline was 9 November 2022, and the review-type articles were further searched and included in the analysis.
Inclusion criteriaStudy reports were included if they had (a) mentioned diagnostic criteria (e.g. International Classification of Diseases-10, Diagnostic and Statistical Manual of Mental Disorders-4th edition, Diagnostic and Statistical Manual of Mental Disorders-5th edition), (b) detailed genotyping and gene frequency data, (c) reported genotypes met the Hardy-Weinberg equilibrium principle, and (d) proper case-controls.
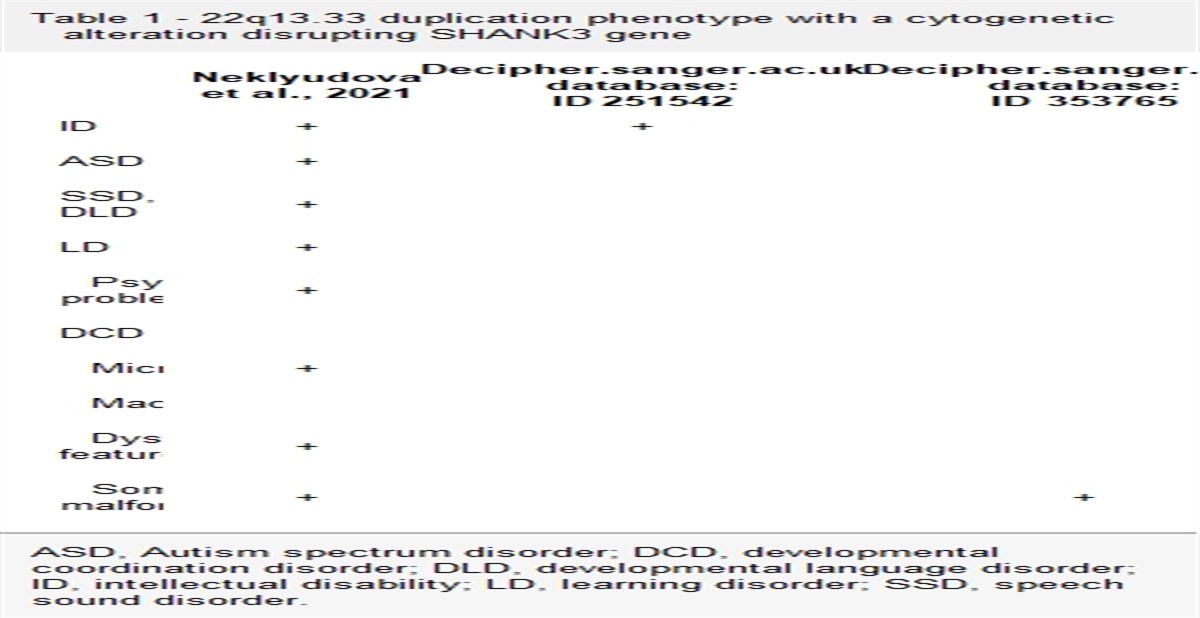
Data extractionBasic demographic information including age, sex, and race; sample sizes; study results; study-specific inclusion and exclusion criteria, diagnostic criteria, and severity assessment criteria; numbers of genotyped samples, and allelic distributions in both case and control groups were extracted from the included reports (Tables 1,2 and 3).
Table 1 - Genotype and allele frequency in the included studies Authors Year Race Diagnostic criteria Results Case Control Case Control Total Val/Val Val/Met Met/Met Total Val/Val Val/Met Met/Met Val Met Val Met Lam et al. 2004 China DSM-IV No association 103 30 53 20 180 34 107 39 113 93 175 185 Shimizu et al. 2005 Japan DSM-IV No association 109 33 56 20 178 59 91 28 122 96 209 147 Lim et al. 2007 Korean DSM-IV No association 106 28 46 32 160 47 82 31 102 110 176 144 Ishii et al. 2009 Japan DSM-IV Association 138 42 56 40 242 55 145 42 140 136 255 229 Otowa et al. 2009 Japan DSM-IV No association 638 223 294 121 589 200 283 106 740 536 683 495 Konishi et al. 2014 Japan DSM-IV No association 470 158 216 96 458 159 221 78 532 408 539 377 Han et al. 2015 Korean DSM-IV No association 136 42 63 31 263 81 135 47 147 125 297 229 Zou et al. 2019 China DSM-IV No association 223 47 118 58 218 60 104 54 212 234 224 212 Wang et al. 2020 China DSM-V No association 85 34 33 18 91 32 36 23 101 69 100 82 Yang et al. 2021 China DSM-V No association 79 24 41 14 76 25 36 15 89 69 86 66 Chu et al. 2022 China DSM-V No association 116 42 48 26 99 35 45 19 132 100 115 83DSM-IV, Diagnostic and Statistical Manual of Mental Disorders-4th edition.
DSM-V, Diagnostic and Statistical Manual of Mental Disorders-5th edition.
Statistical software STATA version 15.0 (Stata Corp. 2015. Stata Statistical Software, Release 15, College Station, Texas, USA) was used for data analysis, following the procedure published elsewhere (Zhao et al., 2013).
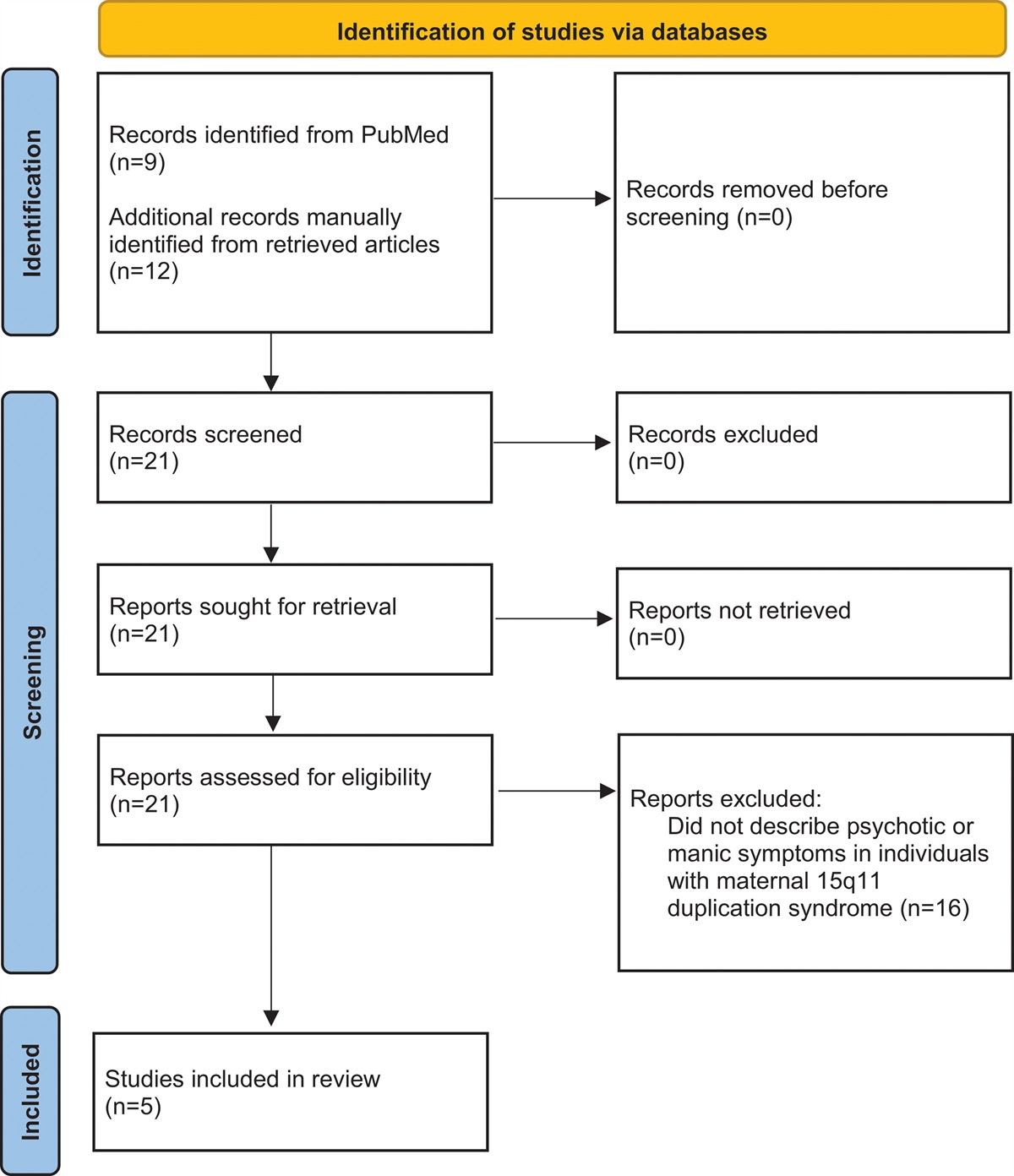
ResultsRelating BDNF Val66Met and PD association, a total of 95 articles were initially retrieved from the selected databases. Among these, 39 articles were further screened to eliminate duplicated searches. Finally, there were only 11 articles that met the inclusion criteria with available data (Lam et al., 2004; Shimizu et al., 2005; Lim et al., 2007; Ishii et al., 2009; Otowa et al., 2009; Konishi et al., 2014; Han et al., 2015; Zou et al., 2019; Wang et al., 2020; Yang et al., 2021; Chu et al., 2022), involving 2203 cases and 2554 controls. The flow chart of literature selection is shown in Fig. 1.
 Fig. 1:
Fig. 1: Flow chart of literature selection process.
Concerning the 11 included articles, detailed clinical characteristics, patients’ demographics, and other relevant information can be identified from Tables 1 and 2. We assumed that the Val66Met allele could be the primary risk factor for PD onset, and then six genetic models of allelic distributions were explored to reveal the relationship between this particular missense mutation and PD susceptibility, as follows: Val versus Met, Val/Met versus Met/Met, Val/Val + Val/Met versus Met/Met, Val/Met versus Val/Val + Met/Met, Val/Val versus Val/Met, and Val/Val versus Met/Met. According to the results of heterogeneity, first, the fixed-effects model was adopted in this meta-analysis to measure the combined odds ratio (COR), and corresponding 95% confidence intervals (CIs) evaluating the genetic association in PD, otherwise, the random-effects model was tested. The study heterogeneity analysis revealed that the effect size in each study was NS (I2 = 0.00%; P = 0.71). The COR derived from these studies was 0.94 (95% CI, 0.87−1.02; z = 1.45; P = 0.15) (Fig. 2), suggesting marginal significant association between the Val66Met allele and PD pathogenesis. Likewise, other models also yield significant genetic correlations with PD. In the Val/Met versus Met/Met model, OR was 0.81 (95% CI, 0.70–0.95; z = 2.67; P = 0.01; Fig. 3). For the Val/Val + Val/Met versus Met/Met model, OR was 0.84 (95% CI, 0.73–0.97; z = 2.42; P = 0.02; Fig. 4); and for the Val/Met versus Val/Val + Met/Met model, OR was 0.88 (95% CI, 0.78–0.98; z = 2.23; P = 0.03; Fig. 5). In contrast, other models yield no significant genetic correlations with PD. In the Val/Val versus Val/Met model, OR was 1.08 (95% CI, 0.95–1.24; z = 1.16; P = 0.25; Fig. 6); for the Val/Val versus Me/Met model, OR was 0.88 (95% CI, 0.75–1.04; z = 1.47; P = 0.14; Fig. 7). Results from the six genetic models demonstrated that the Met/Met genotype might be a susceptibility factor for PD onset.
 Fig. 2:
Fig. 2: Results of the fixed analysis for the BDNF Val66Met allele (Val vs. Met) in the PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
 Fig. 3:
Fig. 3: Results of the fixed analysis for the BDNF Val66Met genotype (Val/Met vs. Met/Met) in PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
 Fig. 4:
Fig. 4: Results of the fixed analysis for the BDNF Val66Met genotype (ValVal + Val/Met vs. Met/Met) in PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
 Fig. 5:
Fig. 5: Results of the fixed analysis for the BDNF Val66Met genotype (Val/Met vs. ValVal + Met/Met) in PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
 Fig. 6:
Fig. 6: Results of the fixed analysis for the BDNF Val66Met genotype (Val/Val vs. Val/Met) in PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
 Fig. 7:
Fig. 7: Results of the fixed analysis for the BDNF Val66Met genotype (Val/Val vs. Met/Met) in PD and control groups. BDNF, brain-derived neurotrophic factor; PD, panic disorders.
Sensitivity analysisSensitivity analysis showed that the estimated value was 0.81, and the 95% CI was in the range of 0.70–0.95, which did not affect the analysis results.
Publication bias testingThe Begg-Mazumdar rank correlation test was used to verify the publication bias, which showed z = 1.09 and P = 0.28, indicating no incidence of publication bias in this analysis.
DiscussionThis updated meta-analysis suggests that the BDNF allele frequencies and genotype distributions are significantly different between healthy controls and PD patients and that the Val66Met mutation in BDNF is a risk factor for PD, which are consistent with the previous meta-analysis (Chen et al., 2017). Moreover, our study, including 11 full-length reports involving 2203 cases and 2554 controls, presented a relatively larger sample size than that of previous investigations(involving 1230 cases and 1612 controls) and, thus, might indicate precise and validated results.
Previous studies have demonstrated that the BDNF Met/Met carriers exhibit an increased not only the sensitivity to anxiety but also the severity of clinical features of panic attacks compared with those of Val/Val or Val/Met carriers (Monteleone et al., 2006; Elzinga et al., 2011). Similarly, the Met allele is believed to play a role in anxiety-associated personality trait disorders, such as higher levels of trait anxiety as well as higher mean neuroticism scores (Sen et al., 2003; Lang et al., 2005). The Egan et al.’s (2003b) report shows that, compared with the BDNF Val allele, the Met allele has a significant negative impact on the activity-dependent secretion of BDNF. Furthermore, a meta-analysis has revealed that the Met allele carriers might have diminished hippocampal volumes compared with that in Val/Val homozygotes (Molendijk et al., 2012). Therefore, the Met/Met homozygous genotype can modulate the activity of BDNF, resulting in a decreased number of hippocampal neuroblasts, as observed in PD patients.
This finding has been further verified in animal studies, consistently showing that the disruption of BDNF’s brain-specific activities could be involved in altered hippocampus structure and associated anxiety disorder phenotypes (Dias et al., 2014).
Based on these results, we may speculate that the reduced activity of BDNF Val66Met may induce hippocampal volume changes in patients with PD, as well, thus, involved in the cause of PD.
As per previous findings, the discrepancy in the BDNF mutation and PD onset could be explained as follows. First, the linkage disequilibrium between the Val66Met and another SNP within the BDNF gene could be causally related to PD pathogenesis, but this condition may not be similarly applicable across the diverse ethnic populations, which may partly explain the reason for inconsistent findings in various studies. Second, the Met allele distribution frequency largely depends on the ethnic background of an individual and most likely varies across diverse ethnic populations influencing the statistical power of the study. For example, Ishiguro et al. (Ishiguro et al., 2011) have reported that the genotypic distribution of rs6295G/G is 3.1%, whereas that in the Yevtushenko et al.’s (2010) study is 19.6%. Shimizu et al. (2004) have proposed that the ethnic difference-based distribution variation of the BDNF G196A (Val66Met) allele may help explain the reason for differential prevalence rates of illness in different ethnic populations. Third, BDNF Met/Met carriers are reportedly more sensitive to stress. The early life stress exposure in this population may predict elevated anxiety levels and its association with panic attacks (Chen et al., 2006; Elzinga et al., 2011). Thus, future studies should consider genetic factors, recent stress exposures, childhood abuse, and age at onset to accurately analyze their roles in the cause of PD.
One major drawback of this study was the small number of included articles and their limited sample sizes. Hence, we could not assess multiple subclinical factors as well as sex differences to elucidate their roles in the etiopathology of PD, warranting further studies to comprehensively analyze their effects. Additionally, we were not able to include the combined effects of BDNF G196A polymorphism versus environment factors’ interactions in PD pathology. It is shown that the gene-environment interactions are critical players in the onset of complex psychiatric disorders, such as PD.
In summary, this updated meta-analysis could identify pathological linkage between the BDNF Val66Met mutation and the cause of PD patients. However, further studies with statistically larger sample sizes and involving individuals from different ethnic backgrounds with additional clinical factor assessments are needed to precisely elucidate the nature of this etiopathology.
AcknowledgementsThe authors would like to thank all the volunteers for taking part in this study. This study was supported by the Young Teacher Foundation of CMU (XZR20160010) for Dr. Yinglin Huang.
Conflicts of interestThere are no conflicts of interest.
References Albert CM, Chae CU, Rexrode KM, Manson JE, Kawachi I (2005). Phobic anxiety and risk of coronary heart disease and sudden cardiac death among women. Circulation 111:480–487. Chen Z-Y, Patel PD, Sant G, Meng C-X, Teng KK, Hempstead BL, et al. (2004). Variant brain-derived neurotrophic factor (BDNF)(Met66) alters the intracellular trafficking and activity-dependent secretion of wild-type BDNF in neurosecretory cells and cortical neurons. J Neurosci 24:4401–4411. Chen Z-Y, Jing D, Bath KG, Ieraci A, Khan T, Siao C-J, et al. (2006). Genetic variant BDNF (Val66Met) polymorphism alters anxiety-related behavior. Science 314:140–143. Chen K, Wang N, Zhang J, Hong X, Xu H, Zhao X, et al. (2017). Is the Val66Met polymorphism of the brain-derived neurotrophic factor gene associated with panic disorder? A meta-analysis. Asia Pac Psychiatry 9. Chu L, Sun X, Jia X, Li D, Gao P, Zhang Y, et al. (2022). The relationship among BDNF Val66Met polymorphism, plasma BDNF level, and trait anxiety in Chinese patients with panic disorder. Front Psychiatry 13:932235. Dias GP, do Nascimento Bevilaqua MC, da Luz ACDS, Fleming RL, de Carvalho LA, Cocks G, et al. (2014). Hippocampal biomarkers of fear memory in an animal model of generalized anxiety disorder. Behav Brain Res 263:34–45. Egan MF, Kojima M, Callicott JH, Goldberg TE, Kolachana BS, Bertolino A, et al. 2003a). The BDNF val66met polymorphism affects activity-dependent secretion of BDNF and human memory and hippocampal function. Cell 112:257–269. Egan MF, Weinberger DR, Lu B (2003b). Schizophrenia, III: brain-derived neurotropic factor and genetic risk. Am J Psychiatry 160:1242–1242. Elzinga BM, Molendijk ML, Voshaar RCO, Bus BA, Prickaerts J, Spinhoven P, et al. (2011). The impact of childhood abuse and recent stress on serum brain-derived neurotrophic factor and the moderating role of BDNF Val 66 Met. Psychopharmacology (Berl) 214:319–328. Greenberg PE, Sisitsky T, Kessler RC, Finkelstein SN, Berndt ER, Davidson JR, et al. (1999). The economic burden of anxiety disorders in the 1990s. J Clin Psychiatry 60:427–435. Han EJ, Kim YK, Hwang JA, Kim SH, Lee HJ, Yoon HK, et al. (2015). Evidence for association between the brain-derived neurotrophic factor gene and panic disorder: a novel haplotype analysis. Psychiatry Investig 12:112–117. Ishiguro S, Watanabe T, Ueda M, Saeki Y, Hayashi Y, Akiyama K, et al. (2011). Determinants of pharmacodynamic trajectory of the therapeutic response to paroxetine in Japanese patients with panic disorder. Eur J Clin Pharmacol 67:1213–1221. Ishii T, Akiyoshi J, Hanada H, Ishitobi Y, Tanaka Y, Tsuru J, et al. (2009). Association between the obestatin and BDNF gene polymorphism and panic disorder, and depressive disorder. Psychiatr Genet 19:159. Karege F, Perret G, Bondolfi G, Schwald M, Bertschy G, Aubry JM (2002). Decreased serum brain-derived neurotrophic factor levels in major depressed patients. Psychiatry Res 109:143–148. Konishi Y, Tanii H, Otowa T, Sasaki T, Tochigi M, Umekage T, et al. (2014). Gene× gene× gender interaction of BDNF and COMT genotypes associated with panic disorder. Prog Neuropsychopharmacol Biol Psychiatry 51:119–125. Kurita M, Nishino S, Kato M, Numata Y, Sato T (2012). Plasma brain-derived neurotrophic factor levels predict the clinical outcome of depression treatment in a naturalistic study. PLoS One 7:e39212. Lam P, Cheng CY, Hong CJ, Tsai SJ (2004). Association study of a brain-derived neurotrophic factor (Val66Met) genetic polymorphism and panic disorder. Neuropsychobiology 49:178–181. Lang UE, Hellweg R, Kalus P, Bajbouj M, Lenzen KP, Sander T, et al. (2005). Association of a functional BDNF
留言 (0)