
記住我
Pressure injuries (PIs) are lesions caused by unrelieved pressure and/or shear, resulting in damage to underlying tissues. Pressure injuries represent a major medical and nursing problem that complicates the patient’s outcome.1 According to the National Pressure Injury Advisory Panel, the prevalence of PI in hospitals in the US ranges from 3% to 14%.2 The high incidence of PIs worsens the quality of life of hospitalized patients and increases the length of hospital stay and the cost of treatment, in addition to the risks of infection.3
The goals of a wound dressing are to provide immediate physical protection to the skin, maintain a conducive environment for wound healing, and incorporate active ingredients that enhance the wound-healing process.4 Dressings have been part of wound care since ancient times. Several topical products and components have been developed for this use. Natural and herbal products are popular in the wound-healing process to stop bleeding, prevent infection, and promote tissue regeneration.5
Some products of natural origin are effective in wound healing, such as propolis,6Aloe vera,7 and Calendula officinalis.8,9 However, most studies investigating these products either were performed on animals or were clinical trials with small samples that lacked methodological quality. Thus, this systematic review aimed to describe the controlled clinical trials of topical natural products applied to patients with PIs and verify any phytochemical similarities among these products.
METHODSThe present study is a systematic review prepared according to the scope analysis methodology. Scoping reviews can be used to map the key concepts that underpin a field of research and clarify working definitions and/or the conceptual boundaries of a topic.10,11 The authors used the JBI Manual for Evidence Synthesis12 to provide a transparent and systematic methodology to analyze the articles.
Research QuestionsTwo questions guided this review: (1) Do topical natural products have a wound-healing effect on patients with PIs? And (2) are there any similarities in the phytochemistry of natural products that demonstrate PI wound-healing activity?
Data Sources and Search StrategyControlled trials were searched in the following electronic databases from their inceptions until February 1, 2022: Cochrane Central Register of Controlled Trials, EMBASE, PubMed, SciELO, Science Direct, and Google Scholar. Gray literature was also searched (Google Scholar). Studies in English and Portuguese were included. Keywords for the search were derived from the concepts of the research question and were combined using Boolean operators “AND” and “OR”: pressure ulcers AND (“clinical trial” OR “intervention study”) AND (wound OR injuries) AND healing AND (topical OR topic). To enhance the search sensitivity, MeSH (Medical Subject Heading) terms were incorporated as agreed on by the researchers.
Eligibility Criteria and Study SelectionThe inclusion criteria for the studies were: individuals with PIs, individuals treated with topical natural products and compared with a control treatment (reference medicine or traditional medicine), and outcomes of wound healing or reduction. Only clinical studies (randomized and nonrandomized) available online that answered the questions of this research were eligible.
Exclusion criteria were abstract-only publications (ie, no full-text article available) and articles written in languages other than English and Portuguese. In addition, studies that included only individuals with chronic diseases, such as cancer and diabetes, were excluded.
Search results were stored in the reference manager Mendeley. One author performed the searches. Two investigators reviewed the titles and abstracts of the references and screened eligible studies according to the inclusion and exclusion criteria. Then, the full texts of the eligible studies were downloaded to determine the final selection. Independent reviewers screened the studies, and Cohen κ measured intercoder agreement. The third author arbitrated all discrepancies between the two reviewers through discussion.
Data ExtractionA template data extraction instrument from JBI for tracking source details, study characteristics, and results was adapted and used by the reviewers. Data were independently extracted from all the included studies using a standardized extraction table by two reviewers. Extracted information included authors, year of publication, country of origin, aims/purpose, population and sample size, methods, intervention type, duration of the intervention, outcomes, and key findings related to the scoping review questions.
Data Summary and SynthesisCharacteristics of the included articles were summarized in a table. To ensure reliability, two authors separately reviewed the literature and, after discussion, the results were approved. The outcome synthesis of the studies and the comparison between similar articles were evaluated. In addition, a bibliographic survey was carried out on the phytochemistry of natural products to try to answer the secondary question.
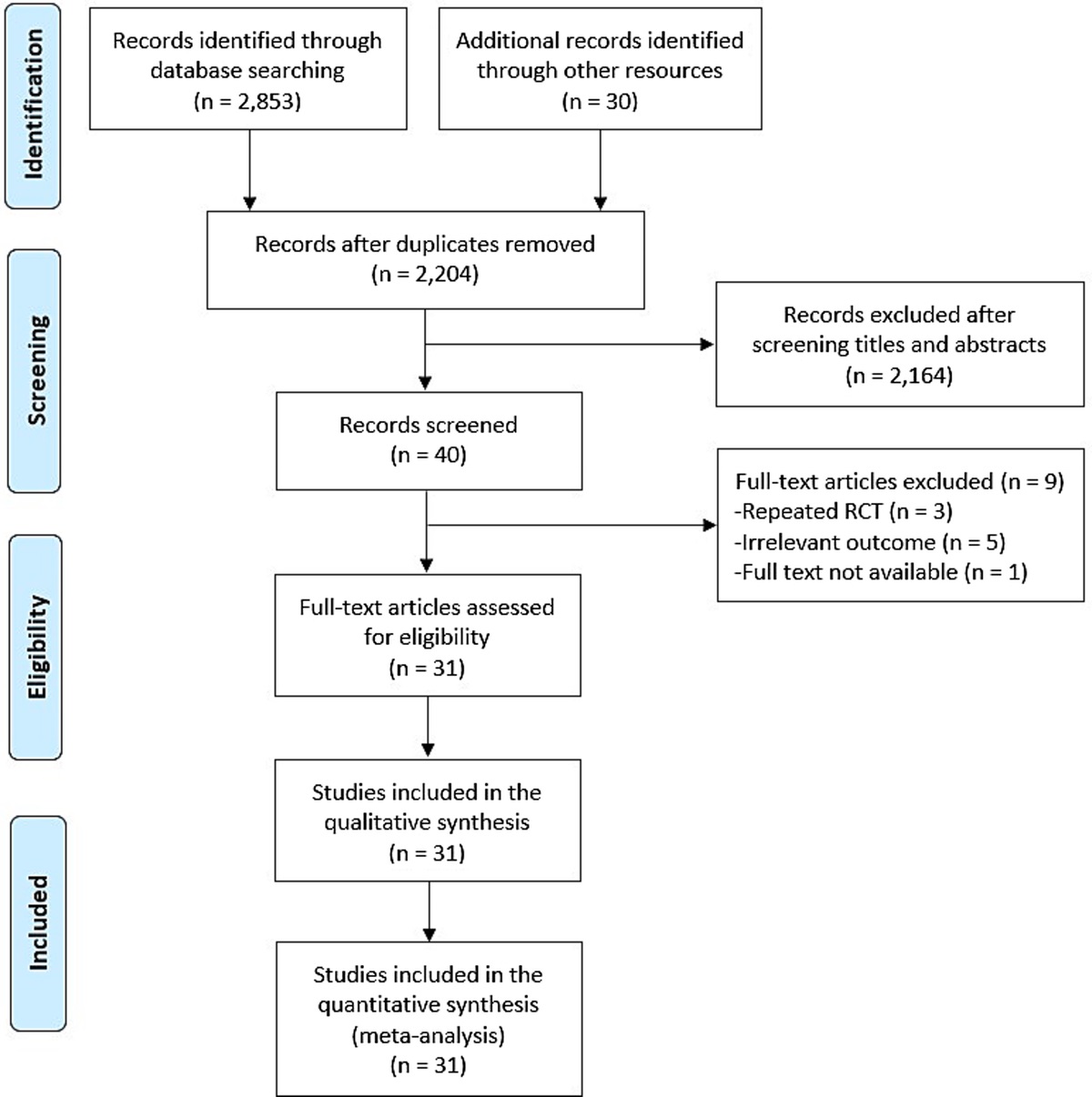
RESULTSThe search identified 1,268 articles (Figure 1). In total, 105 duplicate articles were excluded, followed by the exclusion of 1,140 articles from the title and abstract screen, resulting in the assessment of 23 full-text articles. The common causes of exclusion from studies were wounds other than PIs, uncontrolled studies, reviews, and interventions other than topical application. The authors achieved consensus on the articles selected for the review according to the eligibility criteria. The agreement between the reviewers for the inclusion of studies assessed (Cohen κ statistic) was 0.91, which is a particularly good degree of agreement in screening. In total, six studies were included in this review, of which four were randomized controlled trials (RCTs)13–16 and two were nonrandomized clinical trials.17,18
 Figure 1:
Figure 1: FLOWCHART OF SEARCH STRATEGY AND SCREENING RESULTS
Study CharacteristicsThe Table summarizes the characteristics of the six studies included in this review. One study each was carried out in Australia,17 the US,13 Turkey,14 Thailand,15 Brazil,18 and Iran.16 All six studies were published in English, and the dates of publication ranged from 1991 to 2021. Study participants (N = 265) ranged in age from 18 to 97 years. The duration of the intervention ranged from 6 days to 10 weeks. The studies evaluated the outcomes daily,16 weekly,13,14,17,18 or every 2 weeks.15 These studies evaluated different stages of PIs.
The included studies investigated natural products and their derivatives in healing PIs. The experimental groups evaluated: F14001 cream (extract of barley plant at a strength of 1%),17 acemannan hydrogel (complex carbohydrate derived from A vera),13 honey,14 Thai traditional medicine (TTM; honey or Thai herbal oil [THO] preparation),15A vera (A vera-based gel 0.5%),18 and phenytoin plus Plantago major formulation.16 The frequency of treatment also varied among the included studies (Table).
Table - DETAILS OF STUDIES INCLUDED IN THE REVIEW Intervention Study, Year, Country Purpose Population Methods/Duration Control Experimental Outcomes Key Findings LeVasseur and Helme,17 1991,Abbreviations: CG, control group; EG, experimental group; PI, pressure injury; PUSH, Pressure Ulcer Scale for Healing; RCT, randomized clinical trial; THO, Thai herbal oil; TTM, Thai traditional medicine.
In the studies included in this review, two used the score obtained on the Pressure Ulcer Scale for Healing (PUSH) as the primary outcome;14,15 the other four trials evaluated PIs by measuring lesions and photographic records.13,16–18 The PUSH scale consists of three domains—length times width, exudate amount, and tissue type—and scores can range from 0 to 17.
Summary and SynthesisThe outcomes presented in the trials included in the review suggest that the evaluated natural products have wound-healing activity in patients with PIs. However, each study’s results varied compared with the control groups.
LeVasseur and Helme17 analyzed the efficacy of F14001 cream relative to an inactive placebo cream in older adults (N = 21) with stages 1 and 2 PI. The results showed that both experimental and control groups had a reduction in injury size throughout the trial (P < .001). Patients in the experimental group showed a significant reduction in injury size compared with the control group at week 4 of the trial (P < .05).
Thomas et al13 and Pinheiro et al18 evaluated the effect of A vera and its derivative. Thomas et al13 evaluated the effect of a complex carbohydrate derived from the A vera plant (acemannan) in adults (N = 30; age range, 35–97 years) with stage 2, 3, or 4 PIs. Complete healing of the study injury occurred in 63% of the patients during the 10-week observation period. No difference was observed in complete healing between the experimental and control groups (odds ratio, 0.93; 95% CI, 0.16–5.2). When the healed injuries were stratified by clinical stage, neither stage 2 nor stage 3 injuries differed when treated with the study dressing (Table). No stage 4 injury healed during the trial period.
In contrast, the study by Pinheiro et al18 evaluated the effect of A vera gel versus a conventional gel (Kolagenase). It is worth mentioning that the same patient presented injuries in both group A (injury on the right side of the body or upper torso) and group B (injury on the left side of the body or lower torso). Group A lesions were treated with A vera gel, and group B lesions were treated with Kolagenase gel. However, although this study was an RCT, and the authors reported the healing action of A vera on PIs, qualitative data were not presented.
Güneş and Eşer14 compared the effect of a honey dressing against an ethoxy-diaminoacridine plus nitrofurazone dressing in adults (N = 26) with stage 2 or 3 PIs. Patients managed with honey dressings showed a statistically significant mean decrease in injury size at 5 weeks compared with patients managed with ethoxy-diaminoacridine plus nitrofurazone dressings (56% reduction vs 13% reduction, P < .001). However, only 20% (n = 5) of the patients treated with a honey dressing achieved complete wound healing. No patients in the control group achieved complete wound healing.
Chotchoungchatchai et al15 evaluated the efficacy of honey or a THO for the treatment of PIs based on the TTM wound diagnosis compared with standard practice in adults (N = 66; age range, 18–65 years) with stage 2, 3, or 4 PIs. The primary outcome of this study was PUSH score. The results showed that mean PUSH scores were reduced significantly at 6 weeks. However, when the two groups were compared (experimental and control groups), no significant difference in PUSH score reduction at 6 weeks was detected.
In the last study included in this review, Ghiasian et al16 determined the clinical effect of topical P major on the treatment of patients with stage 1 PI. The experimental group received a topical formulation of phenytoin plus P major, and the control group received phenytoin topical formulation plus placebo. From the beginning to the end of the intervention, patient wound areas were examined daily by a doctor, and observations recorded on a checklist. Over the 14 days of the treatment, the test group had 96% improvement, and the control group had 73% improvement (P < .05).
Only the trials by Günes and Eser14 and Ghiansian et al16 reported that the experimental treatment was more efficient in wound reduction than the respective control group treatment (Figure 2). The other studies13,15,17,18 did not note significant between-group differences.
 Figure 2:
Figure 2: STUDIES THAT SHOWED A SIGNIFICANT DIFFERENCE BETWEEN THE EXPERIMENTAL AND CONTROL GROUPS
DISCUSSIONOverall, the studies included in this scoping review found that natural products contribute to the wound-healing process of PIs. However, only two studies reported a significant difference between the experimental and control groups: one investigated a dressing with honey,14 and the other evaluated P major.16 The study with P major16 included only patients with stage 1 PIs, but the experimental group showed a 96% improvement. As for the trial that evaluated the honey dressing,14 only 20% of the wounds fully healed by the end of the study period; however, this study analyzed stages 2 and 3 PIs.
Barley ExtractBarley (Hordeum species) is mainly used as animal feed and raw material for malt and beer manufacturing. According to some studies, barley can function as an antioxidant and anti-inflammatory agent in vitro and in vivo.19–21 LeVasseur and Helme17 showed that the active F140001 cream, which contains barley plant extract, was significantly beneficial in the fourth week. Their study also demonstrated a significant improvement in injury size throughout the 6-week trial period in both treatment and placebo groups. Few studies have investigated barley plant activity on wound healing. However, the results of Fusté et al22 indicate that the barley β-glucan signal induces an early response in human dermal fibroblasts cells favoring migration versus proliferation and accelerating wound closure in vivo.
Aloe vera and DerivativesAloe vera has traditionally been used to treat skin injuries and digestive problems because of its antimicrobial, anti-inflammatory, and wound-healing properties.23 Some studies have shown fast healing of wounds with A vera treatment in animals24 and in humans.7 A systematic review by Dat et al7 suggested that A vera affects PI wound healing; however, the reviewed studies lacked high-quality clinical trial evidence to support the use of A vera topical agents or A vera dressings as treatments for acute and chronic wounds. Other studies have demonstrated the activity of A vera in PI prevention.25,26 Of the clinical studies included in the present review, Thomas et al13 and Pinheiro et al18 showed that A vera aids PI healing, although it did not differ from the control group results. These findings are similar to those previously presented by Dat et al,7 indicating that the data are insufficient to affirm A vera’s effectiveness in PI wound healing.
HoneyHoney is widely used as a dressing for several types of injuries because of its anti-inflammatory and antibacterial properties.27,28 In 1973, Robert Blomfield29 first described applying honey dressings to patients with PIs. In 2003, two patients with PIs who were treated with honey also had great results, and the author reported that using honey resulted in rapid and complete wound healing.30 These studies corroborate the results obtained in the clinical trials included in the current review. Studies by Günes and Eser14 and Chotchoungchatchai et al15 showed that treatment with honey significantly reduced PIs. In addition, according to Günes and Eser,14 honey resulted in a four-times greater decrease in wound size compared with the control group. The mechanisms for honey’s effectiveness may be related to its antibacterial and anti-inflammatory activities.28,31 In addition, low pH and hyperosmolarity are common to all honeys and contribute to a wide spectrum of antimicrobial effects by making the wound environment unfavorable to microorganisms through acidification and water removal,28 and its anti-inflammatory actions helped reduce the level of pain.
Thai Traditional MedicineThai Traditional medicine is the standardized system that is promoted by the Ministry of Public Health and taught in colleges all over Thailand. This system primarily originated from royal medicine traditions, with significant Western influence.32,33
Although TTM is widely applied in clinical practice, clinical trials showing the activity of TTM in wound healing remain scarce. One such study by Chusri et al34 found that one of the Thai herbal formulas used for wound healing, THR-SK010, has remarkable antibacterial potency and wound healing-related biologic activities. In the study by Chotchoungchatchai et al15 included in this review, researchers observed that applying THO accelerated PI healing. The preparation consists of Clinacanthus nutans Lindau (leaves) and Zingiber montanum Link (rhizome). Clinacanthus nutans is a medicinal plant with promising therapeutic potential because of its antioxidative, antibacterial,35 and anti-inflammatory activities.36,37Zingiber montanum is commonly used to treat inflammations, sprains, rheumatism, and asthma38,39 and has antioxidant activity.40
Plantago majorPlantago major has been used as a traditional medicinal plant in several therapeutic applications.41,42 According to Genc et al,43 isolated constituents from P major may have wound-healing activity. However, a systematic review by Cardoso et al44 found no evidence of the effectiveness of P major for wound healing in vivo.
In the clinical trial carried out by Ghiansian et al,16 the authors observed that the group treated with P major experienced better recovery compared with the control group (P < .05). According to previous studies with P major, its effect on wound healing can be attributed to its antioxidant, anti-inflammatory, antimicrobial, and tissue-repairing effects.45,46
Phytochemistry of the Natural Products Included in This Review BarleyThe phytochemistry of barley extracts shows that this cereal is a rich source of phenolic acids, flavonoids, and anthocyanins.47,48
Aloe veraAloe vera is a succulent, tender plant with a high water content (99%–99.5%). Solid contents range from 0.5% to 1% and consist of various active components.23 The most frequently investigated pharmacologically active compounds isolated from A vera are aloe-emodin, aloin, aloesin, emodin, and acemannan.49
HoneyHoney has a complex composition, and its constituents vary according to geographic and botanical origin, season, and bee management.50,51 Oliveira et al52 identified the major compounds gallic acid and quercetin when analyzing honey produced by different bees in Brazil. Manuka honey, from Australia, contains a high amount of phenolic compounds, such as pinobanksin and quercetin, and other bioactive compounds, such as glyoxal and methylglyoxal.53 In Eucalyptus honeys from central and South America, Europe, and Asia, many phenolic compounds, such as gallic acid and quercetin, have been observed.54
Thai herbal oilThai herbal oil is prepared from C nutans Lindau (leaves) and Z montanum Link (rhizome). Flavonoids, triterpenoids, steroids, phytosterols, and glycosides are the phytochemical classes most likely to be present in C nutans extract when it is prepared with polar solvents.37,55Clinacanthus nutans is a good source of phenolics and flavonoid compounds.55Zingiber montanum includes terpinen-4-ol and γ-terpinene as a major component of THO.38
Plantago majorPlantago major contains several effective chemical constituents, including flavonoids, alkaloids, terpenoids, phenolic acid derivatives, iridoid glycosides, fatty acids, polysaccharides, and vitamins.42,56 Ghiansian et al16 used quercetin as a chemical marker for P major extract. The authors chose quercetin and its derivatives because these compounds have very high antioxidant and anti-inflammatory activity among the plant’s chemical compounds.
All the natural products evaluated by the clinical trials included in this scoping review share the presence of phenolic compounds in their phytochemistry. Studies show that phenolic compounds have excellent wound-healing activity.9,57 When analyzing Güneş and Eşer14 and Ghiansian et al,16 the two studies included in this review that showed a significant difference between the control and treatment groups in PI healing, a common compound stands out in the chemical composition of these treatments, namely, quercetin (Figure 3).
 Figure 3:
Figure 3: QUERCETIN AND SOME OF ITS DERIVATIVES PRESENT IN NATURAL PRODUCTS
Quercetin and its derivatives are flavonoids that alone or in synergy with other phytocompounds can help restore physiologic conditions in the wound-healing process.57 Quercetin has important biological activities related to improving wound healing, such as antibacterial, anti-inflammatory, and antioxidant properties.58,59 Research indicates that quercetin treatment improves wound healing in vitro and in vivo.60,61
Natural products and their structural analogs have historically made a major contribution to pharmacotherapy. Natural products offer special features compared with conventional synthetic molecules, which confer advantages and challenges for the drug-discovery process.5 Phenolic acids are prominent phytocompounds responsible for PI wound-healing activity among natural products.57 As noted in this review, few studies have developed dressings containing these phytocompounds for patients with PIs. Therefore, a rigorously designed large-scale RCT is required to provide robust evidence regarding using natural products to treat PIs.
LimitationsFirst, this systematic review included only six studies; there are few controlled trials of natural products for PIs. The included studies evaluated PIs at different stages, in addition to evaluating different natural products. Each trial also had limitations. The study by LeVasseur and Helme17 was limited by the difference in treatment frequency in the experimental and control groups. The major limitation of the Thomas et al13 trial was the number of patients and the observational time. Güneş and Eşer’s14 study was not blinded to the treatment group, and variability exists in the potency of the antimicrobial effects associated with unprocessed honey. The observational time is a limitation of the study by Chotchoungchatchai et al.15 Pinheiro et al18 did not present qualitative data, and Ghiasian et al16 did not provide details on how healing was assessed. Finally, the standardization of extracts and derivatives of natural products is not always carried out. The lack of standardization impairs the evaluation of results because several factors alter the chemical constitution of these products.
CONCLUSIONSSeveral studies indicate that compounds of natural origin show wound-healing activity in PIs. However, most clinical trials are not controlled. The studies included in this scoping review show that natural products have a healing effect on PIs. Honey and P major dressings were the most effective interventions. The literature suggests that the effect on wound healing demonstrated by these natural products may be related to the presence of phenolic compounds, mainly the flavonoid quercetin. An effective and safe dressing containing natural products could be a useful option for treating PIs, especially in low- and middle-income countries. However, more rigorous RCTs with adequate sample sizes are required to identify the best natural product and its derivative and increase understanding of the compound mechanisms of action in PI wound healing.
REFERENCES 1. Mervis JS, Phillips TJ. Pressure ulcers: prevention and management. J Am Acad Dermatol 2019;81(4):893–902. 2. Edsberg LE, Black JM, Goldberg M, McNichol L, Moore L, Sieggreen M. Revised National Pressure Ulcer Advisory Panel pressure injury staging system. J Wound Ostomy Cont Nurs 2016;43(6):585–97. 3. Silva DRA, Bezerra SMG, Costa JP, Luz MHBA, Lopes VCA, Nogueira LT. Pressure ulcer dressings in critical patients: a cost analysis. Rev Esc Enferm USP 2017;51:03231. 4. Kathawala MH, Ng WL, Liu D, et al. Healing of chronic wounds: an update of recent developments and future possibilities. Tissue Eng B Ver 2019;25(5):429–44. 5. Atanasov AG, Zotchev SB, Dirsch VM, et al. Natural products in drug discovery: advances and opportunities. Nat Rev Drug Discov 2021;20(3):200–16. 6. Santos MJ, Vianna LAC, Gamba MA. The effect of propolis cream in healing chronic ulcers. ACTA Paul Enferm 2007;20(2):199–204. 7. Dat AD, Poon F, Pham KBT, Doust J. Aloe vera for treating acute and chronic wounds. Sao Paulo Med J 2012;132(6):382. 8. Buzzi M, Freitas F, Winter MB. Pressure ulcer healing with Plenusdermax Calendula officinalis L. Rev Bras Enferm 2016;69(2):230–6. 9. Givol O, Kornhaber R, Visentin D, Cleary M, Haik J, Harats M. A systematic review of Calendula officinalis extract for wound healing. Wound Repair Regen 2019;27(5):548–61. 10. Arksey H, O’Malley L. Scoping studies: towards a methodological framework. Int J Soc Res Methodol Theory Pract 2005;8(1):19–32. 11. Armstrong R, Hall BJ, Doyle J, Waters E. “Scoping the scope” of a Cochrane review. J Public Health 2011;33(1):147–50. 12. Aromataris EMZE, Munn Z. JBI Manual for Evidence Synthesis. Adelaide, Australia: JBI; 2020. 13. Thomas DR, Goode OS, LaMaster K, Tennyson T. Acemannan hydrogel dressing versus saline dressing for pressure ulcers. Adv Wound Care 1998;11:273–6. 14. Güneş ÜY, Eşer I. Effectiveness of a honey dressing for healing pressure ulcers. J Wound Ostomy Cont Nurs 2007;34(2):184–90. 15. Chotchoungchatchai S, Krairit O, Tragulpiankit P, Prathanturarug S. The efficacy of honey and a Thai herbal oil preparation in the treatment of pressure ulcers based on Thai traditional medicine wound diagnosis versus standard practice: an open-label randomized controlled trial. Contemp Clin Trials Commun 2020;17:100538. 16. Ghiasian M, Niroomandi Z, Dastan D, Poorolajal J, Zare F, Ataei S. Clinical and phytochemical studies of Plantago major in pressure ulcer treatment: a randomized controlled trial. Complement Ther Clin Pract 2021;43:101325. 17. LeVasseur SA, Helme RD. A double-blind clinical trial to compare the efficacy of an active based cream F14001 against a placebo non-active based cream for the treatment of pressure ulcers in a population of elderly subjects. J Adv Nurs 1991;16:952–6. 18. Pinheiro D, Ribeiro JA, Oliveira Kde, Rocha S, Nobre G, Nascimento L. Simple blind clinical study of scaring action in Aloe vera as coverage in pressure injuries in hospitalized patients. Int J Dev Res 2020;10:34766–70. 19. Madhujith T, Izydorczyk M, Shahidi F. Antioxidant properties of pearled barley fractions. J Agric Food Chem 2006;54(9):3283–9. 20. Choi KC, Hwang JM, Bang SJ, et al. Methanol extract of the aerial parts of barley (Hordeum vulgare) suppresses lipopolysaccharide-induced inflammatory responses in vitro and in vivo. Pharm Biol 2013;51(8):1066–76. 21. Lee YM, Han SI, Song BC, Yeum KJ. Bioactives in commonly consumed cereal grains: implications for oxidative stress and inflammation. J Med Food 2015;18(11):1179–1186. 22. Fusté NP, Guasch M, Guillen P, et al. Barley β-glucan accelerates wound healing by favoring migration versus proliferation of human dermal fibroblasts. Carbohydr Polym 2019;210:389–98. 23. Maan AA, Nazir A, Khan MKI, et al. The therapeutic properties and applications of Aloe vera: a review. J Herb Med 2018;12:1–10. 24. Tarameshloo M, Norouzian M, Zarein-Dolab S, Dadpay M, Mohsenifar J, Gazor R. Aloe vera gel and thyroid hormone cream may improve wound healing in Wistar rats. Anat Cell Biol 2012;45(3):170. 25. Hekmatpou D, Mehrabi F, Rahzani K, Aminiyan A. The effect of Aloe vera gel on prevention of pressure ulcers in patients hospitalized in the orthopedic wards: a randomized triple-blind clinical trial. BMC Complement Altern Med 2018;18(1):1–11. 26. Baghdadi M, Rafiei H, Rashvand F, Oveisi S. Effect of Aloe vera gel, Calendula officinalis ointment and simple prophylactic sacral dressings for pressure injury development. Chronic Wound Care Manag Res 2020;7:19–26. 27. Molan PC. The role of honey in the management of wounds. J Wound Care 1999;8(8):415–8. 28. Cooper R. Honey for wound care in the 21st century. J Wound Care 2016;25(9):544–52. 29. Blomfield R. Honey for decubitus ulcers. JAMA 1973;224(6):905. 30. Van der Weyden EA. The use of honey for the treatment of two patients with pressure ulcers. Br J Community Nurs 2003;8(12):S14–20. 31. Maruhashi E. Honey in wound healing the history of honey. Ther Dressings Wound Heal Appl 2020:235–54. 32. Disayavanish C, Disayavanish P. Introduction of the treatment method of Thai traditional medicine: its validity and future perspectives. Psychiatry Clin Neurosci 1998;52:S334–7. 33. Jacobsen N, Salguero CP. Thai Herbal Medicine: Traditional Recipes for Health and Harmony. United Kingdom: Inner Traditions/Bear & Co; 2014. 34. Chusri S, Settharaksa S, Chokpaisarn J, Limsuwan S, Voravuthikunchai SP. Thai herbal formulas used for wound treatment: a study of their antibacterial potency, anti-inflammatory, antioxidant, and cytotoxicity effects. J Altern Complement Med 2013;19(7):671–6. 35. Arullappan S, Rajamanickam P, Thevar N, Kodimani CC. In vitro screening of cytotoxic, antimicrobial and antioxidant activities of Clinacanthus nutans (Acanthaceae) leaf extracts. Trop J Pharm Res 2014;13(9):1455–61. 36. Wanikiat P, Panthong A, Sujayanon P, Yoosook C, Rossi AG, Reutrakul V. The anti-inflammatory effects and the inhibition of neutrophil responsiveness by Barleria lupulina and Clinacanthus nutans extracts. J Ethnopharmacol 2008;116(2):234–44.
留言 (0)