
記住我






To the Editor:
Bullous pemphigoid (BP) is a rarely described side-effect of external beam radiation therapy.1–5 In reported cases, skin lesions typically arise after cessation of treatment and are localized to irradiation sites, on occasion spreading to nonirradiated skin or becoming more widespread.1–5 In a minority of affected patients, BP develops during treatment, potentially mimicking other more common acute radiation sequalae/effects, compounding diagnosis and, if not readily recognized, delaying appropriate patient care.1–5 Herein, we report an unusual case of localized, pauci-inflammatory BP that started during radiotherapy for breast cancer.
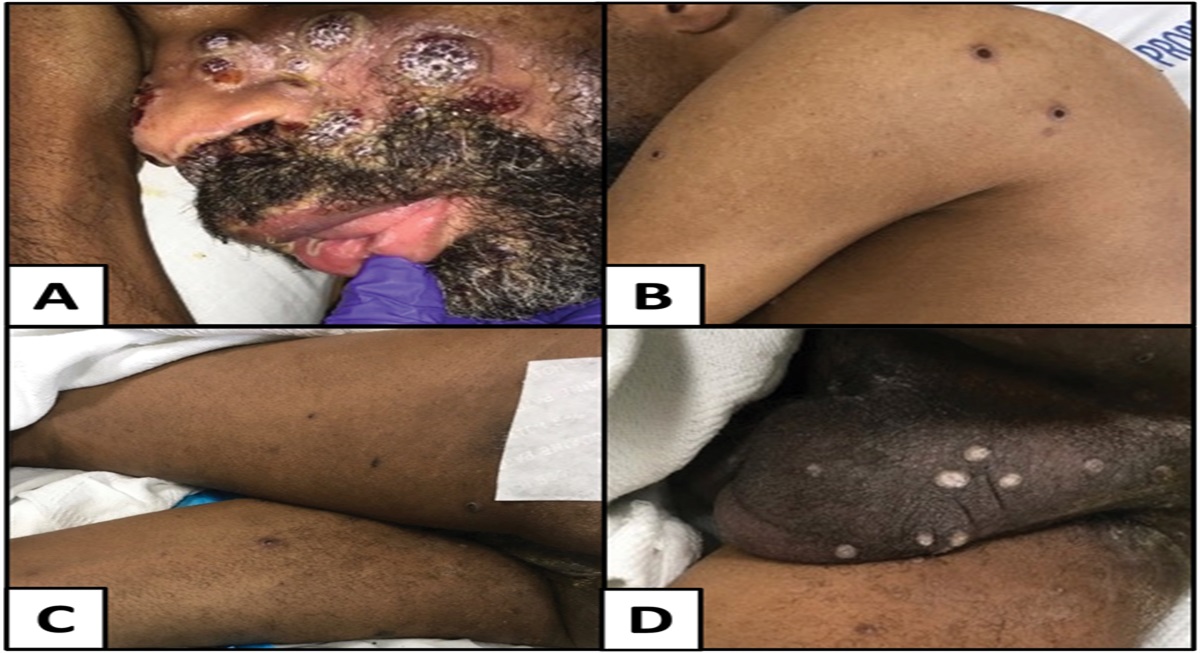
A 74-year-old female presented with painful and pruritic tense bullae and erosions on her left chest and left arm that developed 5 months before (Fig. 1). She had a recent history of invasive ductal carcinoma of the left breast, diagnosed in May 2021, AJCC stage IIA (pT1cN1a), estrogen receptor positive, progesterone receptor positive, HER-2 negative, status post partial mastectomy with axillary lymph node biopsy. The patient was started on anastrozole (aromatase enzyme inhibitor) with tamoxifen (selective estrogen receptor modulator), and discontinued hormone replacement therapy after her breast cancer diagnosis. Other medications included intermittent furosemide, lisinopril, and daily aspirin. The patient underwent 2 months of adjuvant external beam radiation therapy with a cumulative dose of 60 Gray (Gy) to left axillary lymph node region, 46 Gy to left axillary and supraclavicular fields, 26 Gy to left breast, and 26 Gy to left breast surgical bed. Cutaneous signs and symptoms developed early during the course of radiotherapy, leading to suboptimal management that included multiple treatment delays and subtherapeutic doses. New skin lesions continued to arise after cessation of radiotherapy. Cutaneous findings were restricted to the irradiation fields. No oral or mucosal lesions were noted. The patient had no previous history of a blistering skin disease.
 FIGURE 1.:
FIGURE 1.: Tense bullae and erosions on the left chest and left arm, restricted to previous irradiation fields for breast cancer.
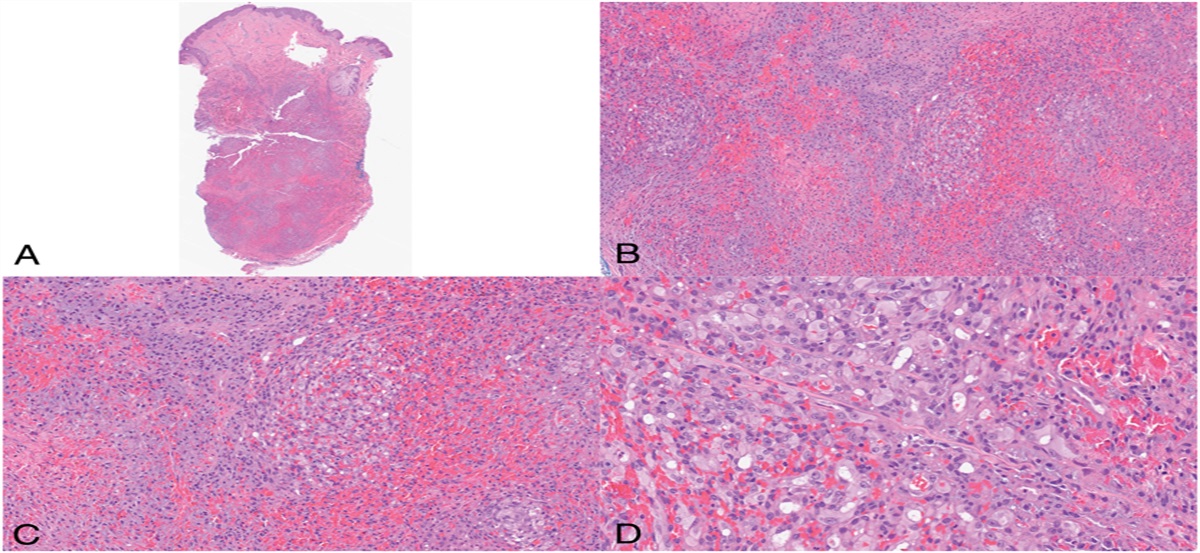
 FIGURE 2.:
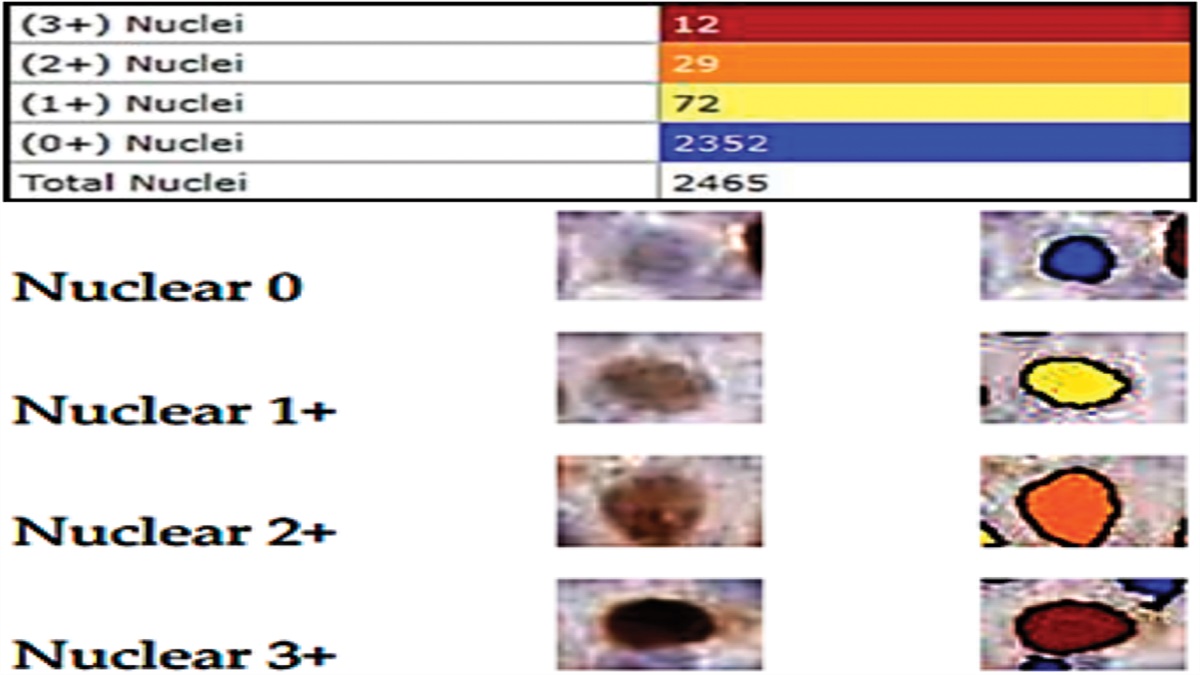
FIGURE 2.: A and B, Histopathologic sections show features of subepidermal split (with denuded epidermis) and sparse superficial dermal inflammation with rare eosinophils. C and D, Direct immunofluorescence studies demonstrate continuous, linear, homogenous IgG (3+) and C3 (3+) deposition along the dermoepidermal junction [hematoxylin-eosin (HE), original magnification ×20 and ×100].
Skin punch biopsies were performed. Hematoxylin & eosin–stained sections demonstrated features of a subepidermal split (with denuded epidermis) and sparse superficial dermal inflammation (Figs. 2A, B). Rare eosinophils were noted. Direct immunofluorescence studies confirmed the presence of continuous, linear, homogenous IgG (3+), and C3 (3+) deposition along the dermal–epidermal junction (Figs. 2C, D). IgA, IgM, and fibrinogen were negative. Serological studies revealed elevated BP230/BPAg1 (31 U/mL, positive reference range >9 U/mL) and BP180/BPAg2 (41 U/mL, positive reference range >9 U/mL) autoantibodies. Indirect immunofluorescence studies were not accomplished. Compete blood count was within normal limits. Complete metabolic profile showed elevated creatinine at 1.03; with other parameters within normal limits. A diagnosis of radiation-induced localized BP was made. The patient was treated with 4-week oral prednisone taper starting at 1 mg/kg/d, topical betamethasone dipropionate 0.05% ointment BID, doxycycline 100 mg BID, and niacinamide 500 mg BID. Over 90% of the cutaneous bullae and erosions healed in 6 weeks.
Cutaneous adverse effects during and after external beam radiation therapy for breast cancer are common, with “radiation dermatitis” occurring in 74%–100% of patients.1–5 Other known cutaneous side-effects include radiation-induced morphea, radiation-induced fibrosis, radiation recall dermatitis, secondary malignancies, erosions, and ulcerations.1 Blistering skin diseases, including immunobullous disorders, are rarely triggered by radiotherapy.1–5
BP is an uncommon side-effect of radiation therapy.1–5 Recent systematic reviews and case–control studies have found that most reported cases of radiation-associated BP occur in women (86%).1–5 Most patients have received radiotherapy for breast cancer (78%–84%), with blistering confined (at least initially; in 89%–93% of individuals) to the site of radiotherapy.1–5 A relatively low dose of 20 Gy can induce skin lesions in some patients.1–5 Up to two-fifths (41%) of patients progress to generalized disease.1–5 Skin lesions typically develop months-to-years after treatment (range, 2 weeks to 16 years; mean, 15 months; median, 5 months).1–5 In contrast, our patient developed bullous skin lesions during radiotherapy, a finding reported in only 15%–28% of previous cases.1–5
The widely accepted pathophysiology of (idiopathic) BP involves circulating and tissue-bound autoantibodies to cutaneous self-antigens (ie, BP230 and BP180 proteins, both components of the hemidesmosome, and responsible for adhesion between epidermis and dermis), leading to complement activation, proteolytic basement membrane cleavage, and subsequent subepidermal clefting.1–5 In most patients, (idiopathic) BP is a generalized disease with tense blisters, erosions, and erythema, with or without urticarial plaques, on the lower abdomen, skin folds, and extremities.1–5 Oral lesions are present in 10%–30% of patients, with rare mucosal involvement at other sites.1–5 Only ∼15% of patients with BP present with an identifiable inciting factor, such as viral infections, various drugs (ie, captopril, furosemide, penicillamine, nonsteroidal anti-inflammatory agents, immune checkpoint inhibitors), mechanical trauma, ultraviolet and infrared irradiation, and rarely, radiotherapy.1–5
The exact etiology (triggering mechanisms/molecular cascades involved) of the localized, radiation-induced variant of BP remains unclear.1–5 Several theories have been proposed to explain the role of ionizing radiation in disease pathogenesis, including: (1) changes in antigenicity of keratinocyte surface/basement membrane antigens at the dermal–epidermal junction, with induction of autoantibody formation; (2) deposition of previously circulating (“sub-clinical”) antibodies onto exposed basement membrane sites, secondary to treatment-induced tissue damage; (3) localized immune system disruption, with alteration of T-cell suppressor activity and consequent autoantibody overproduction; and (4) changes in matrix metalloproteinase-9 (MMP-9) and vascular growth factor levels, with downstream effects1–5 It is also speculated that breast epithelial cells, while undergoing radiotherapy-induced cellular apoptosis, may release hemidesmosomes that become immunogenic and induce production of anti-BP230 and anti-BP180 autoantibodies.1–5 Of note, radiotherapy has been shown to cause an increase in basement membrane antibody binding, likely secondary to endothelial cell injury and increased vascular permeability.1–5 Concurrent medications (ie, chemotherapy, hormonal therapy) and other comorbidities (ie, chronic kidney disease) may also modulate the onset of radiotherapy-associated BP in some patients.1–5
The prognosis for radiation-induced BP is not uniformly reported in the literature, but outcomes generally range from disease control to complete remission with therapy.1–5 The disease generally responds to high-potency topical corticosteroids, and only occasionally requires the use of systemic medications, as in our patient.1–5 Importantly, BP occurring during radiation therapy is distinct from more common “radiation dermatitis,” and its rapid response to treatment suggests that disease development should not interfere with/disrupt on-going radiation oncology management decisions.1–5
Radiation-induced BP should be considered in the differential diagnosis for vesiculobullous eruptions occurring during or after ionizing radiotherapy, particularly in patients with breast carcinoma. Because a clear relationship has been established in all reported cases to date, BP is now recognized as both an early and late side-effect of ionizing radiation.1–5 Dermatologists and radiation oncologists should be aware of the correlation between radiotherapy and BP, allowing for rapid and accurate diagnosis with appropriate patient management.
1. Piras A, Fionda B, Sanfratello A, et al. Bullous pemphigoid and radiotherapy: case report and literature review update. Dermatol Rep. 2022;14:9170. 2. Nguyen T, Kwan JM, Ahmed AR. Relationship between radiation therapy and bullous pemphigoid. Dermatology. 2014;229:88–96. 3. Mul VE, van Geest AJ, Pijls-Johannesma MC, et al. Radiation-induced bullous pemphigoid: a systematic review of an unusual radiation side effect. Radiother Oncol. 2007;82:5–9. 4. Choi R, Cowper S, Young M, et al. Bullous pemphigoid exacerbated by radiation therapy: an atypical presentation. Adv Radiat Oncol. 2022;7:100794. 5. Hung TL, Chen YL, Lin KT, et al. Risk of radiotherapy-associated autoimmune bullous disease among Taiwanese patients with breast cancer: a case-control study. Arch Dermatol Res. 2020;312:69–75.
留言 (0)