
記住我
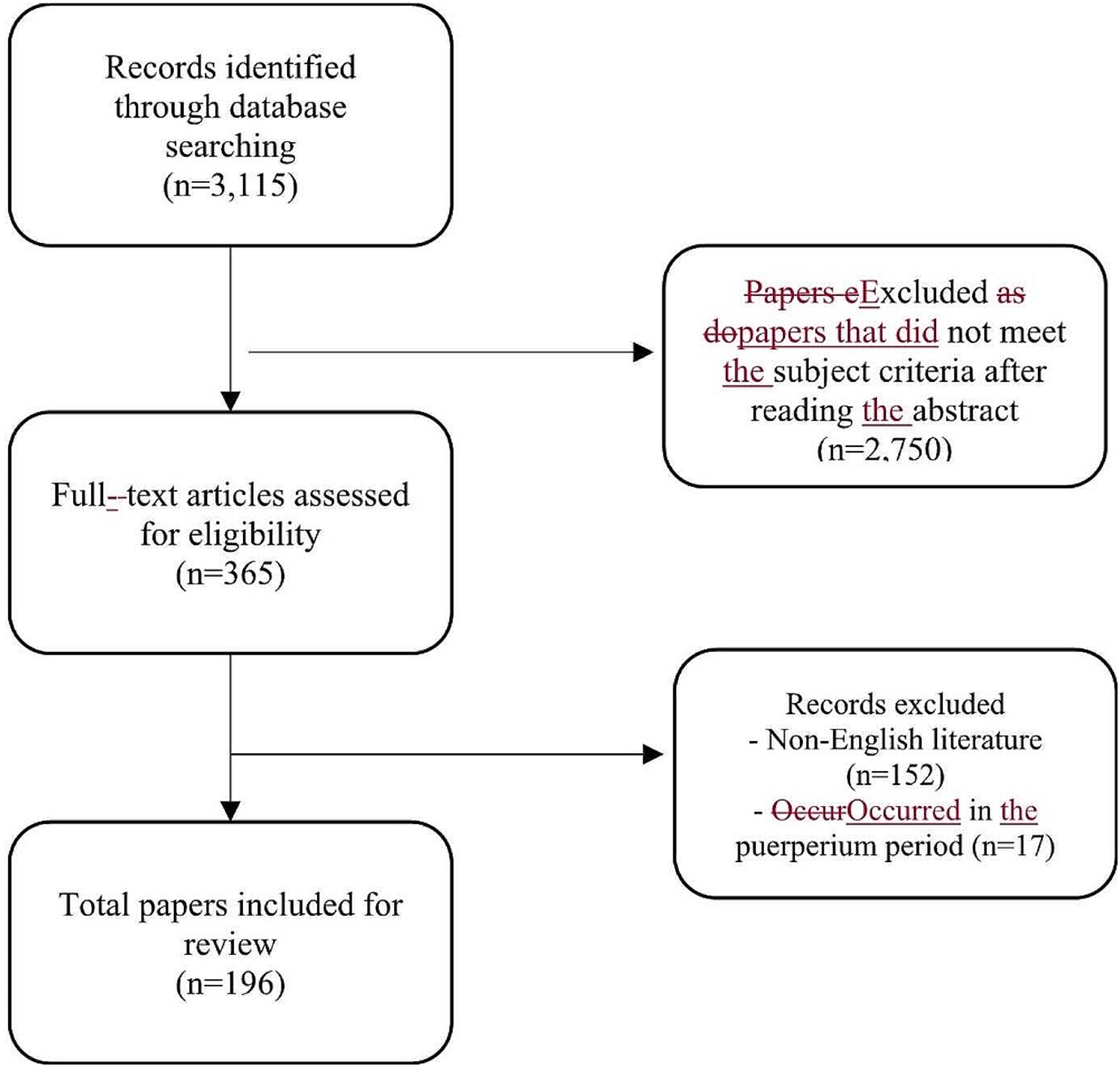
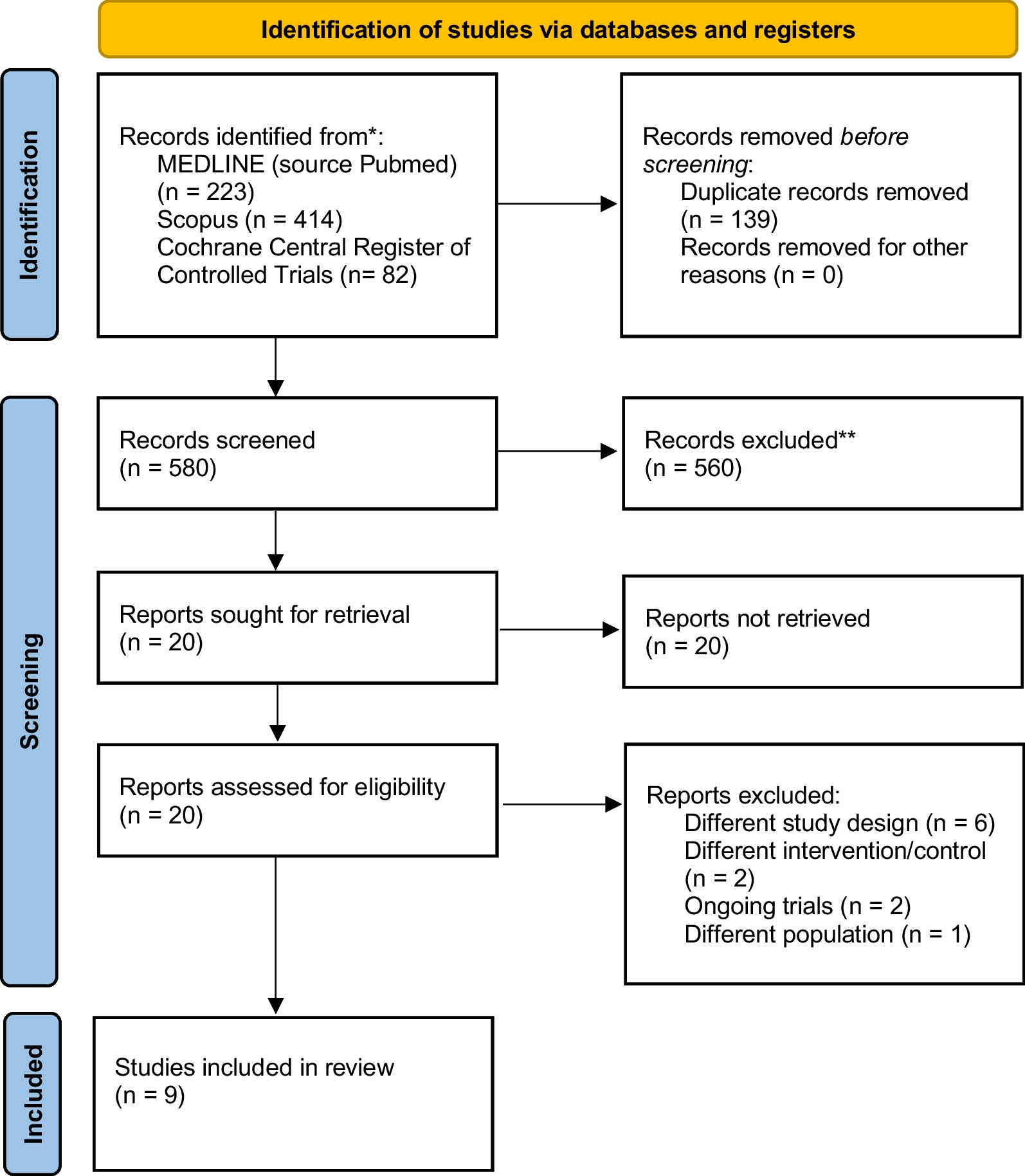


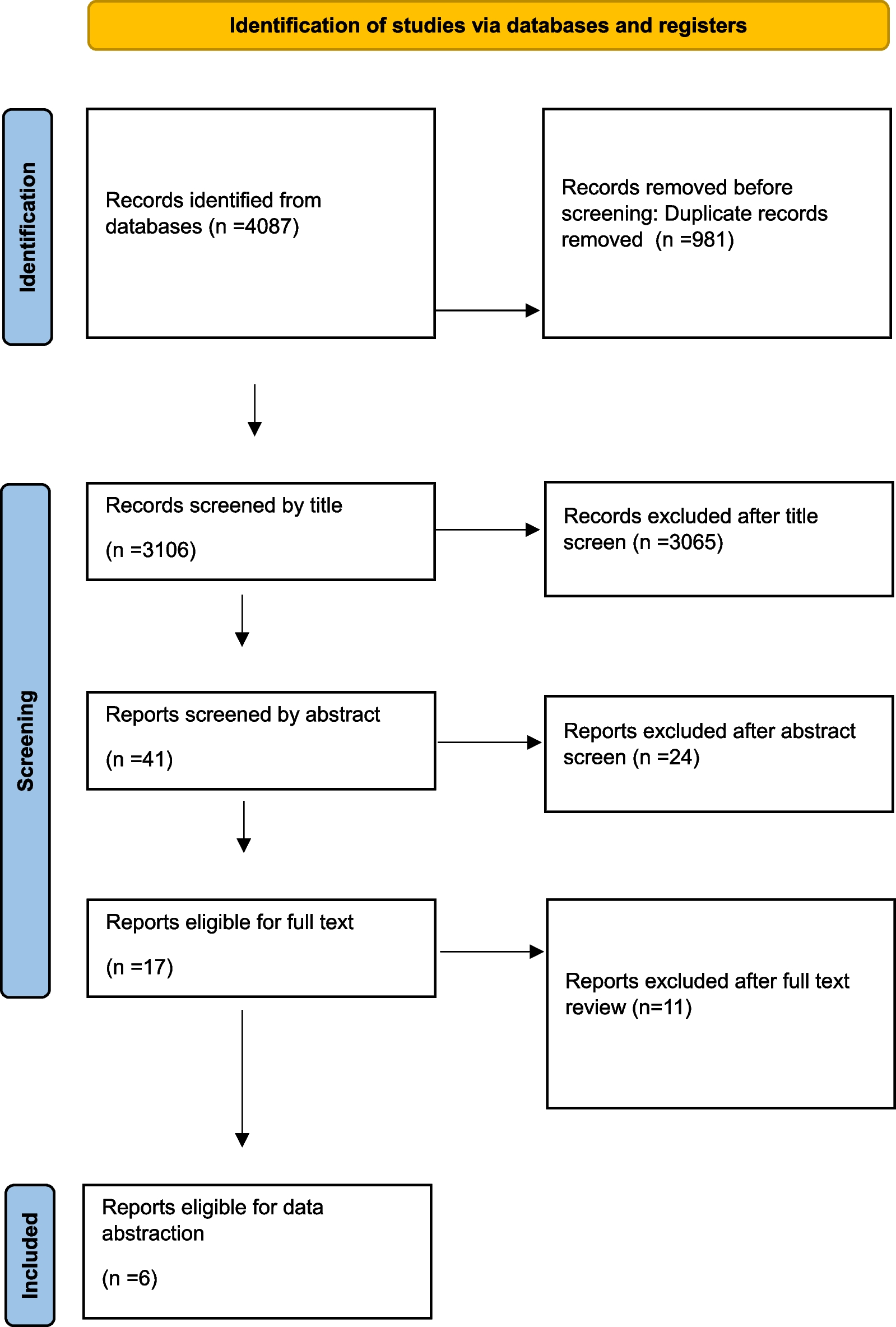
Initially, 14,284 records were identified. After duplicate removal, 13,567 articles were screened upon title and abstract. The majority were excluded because non-pertinent to the review question or did not meet all selection criteria. Forty-five articles underwent a full-text evaluation, and 13 studies were finally included in this review (Fig. 1). The list of the excluded articles after full text evaluation is reported in Additional file 1: Table S1.
Fig. 1
Flowchart of the literature search and selection
Study characteristicsThe included studies were published between 2008 and 2022. All were case series carried out in Asia (n = 6), Europe (n = 5), North America (n = 1), or South America (n = 1). The characteristics of the included studies are summarized in Table 1. Overall, 4557 minimally invasive emergency procedures were described, of which the great majority (85%) was represented by emergency laparoscopic appendectomy. Only one study reported the learning curve in emergency robotic single-site cholecystectomy [20].
Table 1 Studies reporting on learning curve during urgent/emergent minimally invasive surgeryGreat heterogeneity in the learning curve assessment was noted; six studies described the chronological distribution in groups and their evaluation [21,22,23,24,25,26]; one study used the moving average method [27]; two studies used the cumulative sum (CUSUM) analysis [20, 28]; two studies adopted both the moving average method and the CUSUM analysis [29, 30]; and two studies applied the procedural-based assessment [31, 32]. Moreover, six studies evaluated the learning process of resident surgeons [21, 27, 29,30,31,32], four of graduated surgeons [20, 22, 23, 28], and three involved both residents and consultants [24,25,26]. Varying levels of surgical experience were reported in the single studies.
Qualitative synthesis of the literatureLearning curve in emergency laparoscopic appendectomy performed by residentsIn 2008, Jaffer et al. [29] published a study reporting the learning curve of a single surgical resident performing 40 cases of laparoscopic appendectomy. By using the moving average method and the CUSUM analysis, the authors demonstrated that the operative time significantly decreased after 20 procedures, indicating the achievement of the learning curve plateau. However, it is noteworthy that the study included a 6% of negative appendicitis, which may lower the difficulty of the emergency procedure.
Similarly, Kim et al. [27] reported in 2010 the experience of a single 2nd year resident dealing with open and laparoscopic appendectomies. The surgeon’s previous experience consisted of 30 open appendectomies supervised by a senior surgeon. According to the moving average method, the subgroup analysis performed on the laparoscopic group demonstrated a significant reduction in the operative time after 30 cases. Length of stay and complication rate were comparable across the consecutive intervention groups.
Lin et al. [21] in 2010 reported the learning process of six residents who performed laparoscopic appendectomy. Based on previous reports, the authors compared the surgical outcomes of the resident’s initial 20 laparoscopic appendectomies (cases performed during the learning curve) with the subsequent 20 cases. A significant reduction in the operative time and rate of postoperative complications was observed with the increasing experience of the residents. The length of hospital stay and conversion to open surgery did not change over time.
In 2016, Abdelrahman et al. [31] published an analysis of the higher surgical trainee’s curriculum from the 3rd to the 8th year. Different from the other studies, the authors adopted the procedural-based assessment (PBA) method, which allows rating the operating surgeon with an increasing level of competence. Levels were defined as follows: level 0 (L0C), insufficient evidence observed to support a judgment; level 1 (L1C), inability to perform the procedure under supervision; level 2 (L2C), ability to perform the procedure under supervision; level 3 (L3C), ability to perform the procedure with minimum supervision; level 4 (L4C), competency to perform the procedure unsupervised and to deal with eventual complications. The authors investigated the achievement of three L4C ratings in 69 residents’ curricula on six index interventions, among which laparoscopic appendectomy. The L4C was achieved in a median of 107 (20–206) appendectomies. The authors compared this number with the national threshold to obtain the surgical certification (80 procedures), highlighting the need for a 35% higher caseload. In 2017, the same research group published an update of the study adopting the same methodology and performing an analysis of the gradient of competence evolution [32]. Concerning appendectomy, the third level 4 PBA proficiency was reached after 95 cases. The study investigated the trajectory of the learning curve and found a significant gradient related to caseload when comparing the first level 3 PBA and the first level 4 PBA and between the first and the third level 4 PBA.
In 2020, Kim et al. [30] published an analysis of 150 laparoscopic appendectomies performed by residents with a growing level of seniority and experience. Three residents, at the first, second or third year of training, performed 50 consecutive laparoscopic appendectomies; no significant differences were shown in operating time (OT) between the three operating residents. Using the moving average method and the CUSUM analysis, the authors reported a decreasing tendency in OT for all residents, with the achievement of peaks between the 18th and 31st cases. When analyzing the need for takeover by the supervisor during the procedure (defined as surgical failure), the steady state on the CUSUM curve was reached between the 11th and 35th cases.
Learning curve in emergency laparoscopic appendectomy performed by graduated surgeonsIn 2013, Liao et al. [22] reported on the learning curve of single-port laparoscopic appendectomy (SPLA) for noncomplicated appendicitis. The operations were performed by a single surgeon trained in laparoscopic surgery. Thirty SPLA were considered; 3 groups of 10 consecutive SPLA were compared. A significant decrease in OT was observed after 10 cases. Moreover, the study showed that an OT equivalent to a conventional three-port laparoscopic appendectomy was achieved after 30 SPLA cases. No differences were found in the conversion rate, time to resumption of oral intake, length of hospital stay, and postoperative complication rate between the 3 groups of consecutive SPLA.
In 2016, Kim et al. [23] investigated the SPLA learning curve in 120 patients admitted to the emergency department with acute appendicitis. The operations were performed by a single surgeon whose experience was estimated in more than 500 laparoscopic appendectomies and more than 500 conventional open cases. According to the chronological order, 4 groups of 30 consecutive procedures each were compared. A decrease in the OT was observed after 30 cases; no further improvement was reported until 90 operations were completed. No differences were shown between the four groups concerning the rate of postoperative complications, the time to resumption of oral intake, and the length of hospital stay.
Learning curve in emergency laparoscopic appendectomy performed by residents and senior surgeonsIn 2016, Mán et al. reported a series of 600 laparoscopic appendectomies performed by 5 residents having two or three years of surgical experience and by 5 consultants having eight or nine years of surgical experience [24]. The analyses were performed considering different groups of consecutive interventions: those performed during the learning curve period (the first 100 laparoscopic appendectomies for both residents and consultants) and those performed thereafter (219 cases for residents and 181 for consultants). A significant difference in the OT was reported between residents and consultants both during the learning curve period and after the learning curve completion in favor of consultants. However, a reduction in OT was also observed within each group after the completion of the learning curve.
Lee et al. [25] reported the results of a series of 1948 SPLA performed by 8 attending surgeons and 33 residents. By setting the learning curve achievement threshold at 40 procedures, the authors compared the early cases vs. the subsequent ones. They demonstrated a significant reduction in OT after the completion of the learning curve, whereas the rate of intraoperative and postoperative complications was not different over time.
In 2021, Ussia et al. [26] retrospectively investigated the laparoscopic appendectomies performed in a single surgical unit for six years by nine attending surgeons and 64 residents. The 1173 patients operated on were compared after a propensity score matching, which derived two groups of 409 patients each. The results showed that only the hospitalization was significantly longer in the attendings group compared to residents. When the results were stratified by the inflammatory stage of appendicitis, a significant reduction in OT was present in edematous and suppurative cases. This reduction was progressive according to the year of training, but was not confirmed when including gangrenous appendicitis in the analysis.
Learning curve in emergency laparoscopic revisional colorectal surgery performed by graduated surgeonsAngeramo et al. [28] published in 2022 a study describing the learning curve in emergency laparoscopy applied to treat complications of elective laparoscopic colorectal surgery. Between 2000 and 2019, 132 patients underwent a re-operation for postoperative complications by three US board-certified colorectal surgeons. The CUSUM method was used to determine the threshold number of procedures to be performed to reach a stable operative time. Three groups of consecutive procedures (50, 52, and 30 cases respectively) were compared. A higher conversion rate and a longer operative time were observed during the first 50 cases compared to the subsequent cases. Also, the overall morbidity decreased over time, with the lowest rate for the last 30 cases. No differences were reported concerning major morbidity, mortality, and mean length of stay. The authors concluded that 50 laparoscopic interventions should be performed to complete the learning curve.
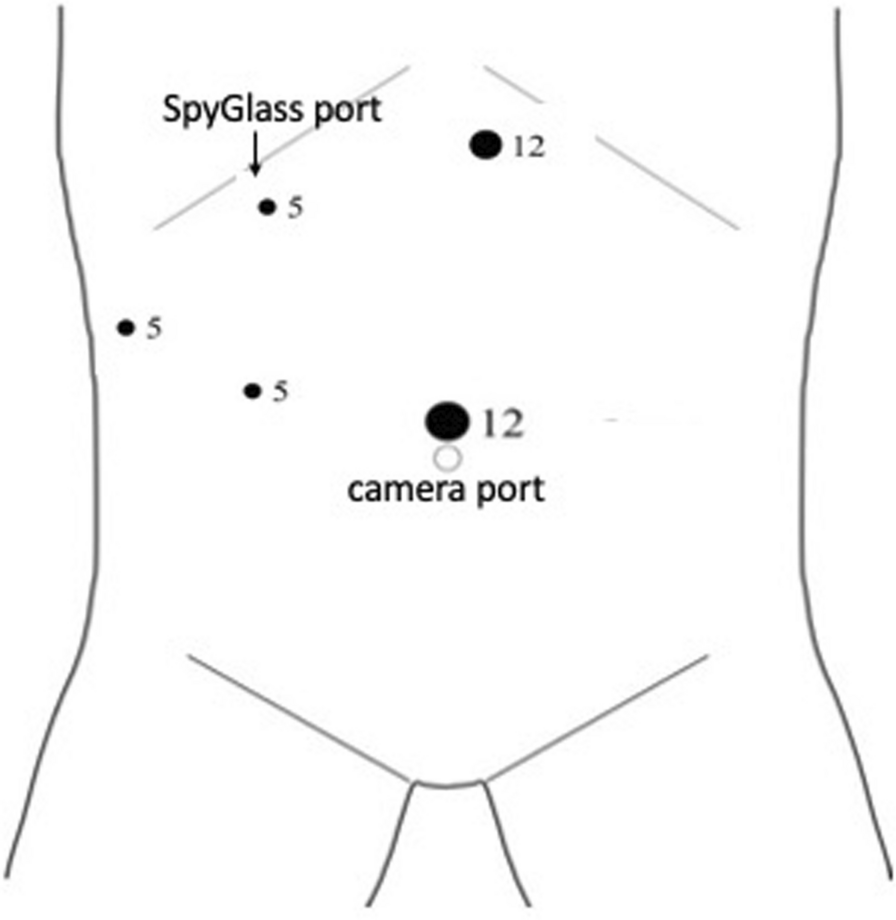
Learning curve in emergency laparoscopic and robotic cholecystectomy performed by graduated surgeonsIn 2016, Kubat et al. [20] described the learning curve of robotic single-site cholecystectomy in a case series of the first 150 patients operated on by a single surgeon. The operator was experienced in both multiport robotic cholecystectomy and single-incision laparoscopic cholecystectomy. Only 74 (49.3%) patients underwent an urgent intervention. The surgeon’s learning curve for OT, including both urgent and elective cases, was reached after 48 operations. A subgroup analysis revealed that the initial learning curve for urgent cases was 25% longer than for elective cases. The authors suggested that developing proficiency in elective cases first may aid the adoption of robotic technology in the urgent setting.
Study quality assessmentThe selected studies were judged of poor to moderate quality, with MINORS scores ranging from 8 to 18 [19] (Table 2). There was great heterogeneity in the methods and outcomes used to assess the learning curve. This is one of the main limitations, which hampers any pooled data analyses and claims for caution in the interpretation and generalizability of the results. The type of training received by the residents and consultant surgeons was rarely described (Table 3), with no standardized pre-clinical training curriculum, including simulation in surgery and hands-on on animal models. Only two studies [21, 24] reported the preclinical training process consisting of surgical simulation and training on animal model but the authors do not specify the time dedicated to training.
Table 2 MINORS scores assessing the risk of bias in non-randomized studiesTable 3 Characteristics of the training process in urgent/emergent minimally-invasive digestive surgery described in the selected studiesThese data highlight the need for further studies to identify and test the effectiveness of specific training programs to be implemented during the residency (and thereafter) until the surgeons reach proficiency in emergency MIS.
Position statementsBased on the review of the literature presented above, the following position statements (PS) were proposed and voted by the Expert Panel. For each statement, the supporting literature, the evidence level, and consensus’s strength are reported. Most of the experts involved works in a university hospital/academic center (72.2%) or tertiary care center (27.8%). Most of them has been performing MIS for surgical emergencies for 10–20 years (44.4%) or more than > 20 years (22.2%). Only half of them have access to a robotic platform for surgical emergencies, but with difficult accessibility (27.8%) or only during daytime (11.1%). The experts were trained and reached proficiency in MIS in different ways. They all believe that an emergency surgeon should continue to perform a caseload of elective MIS procedures to remain proficient in emergency MIS.
PS-1. There is a need for further studies assessing with reliable methods the learning curve process of surgeons in the management of the most common emergencies currently approached with minimally invasive surgical techniques, such as appendicitis, cholecystitis, gastro-intestinal perforations, bowel obstruction, and incarcerated herniae.
The concept of a learning curve has very old origins, described in 1885 by Ebbinghaus as the retention of memorized information [33]. Today, we refer to the process of granting adequate expertise in a given domain [34]. Particularly in surgery, it requires the repetition of a minimum number of procedures to achieve proficiency [13, 35,36,37]. Despite the fact that this represents the basis of surgical education, there need to be more studies elucidating the process of the surgical learning curve, particularly in the emergency setting [38, 39]. This potentially translates into disparities in medical education between residency programs, countries, and regions [39, 40]. Most of the time, the surgeon who starts to work autonomously at the end of residency has not yet reach full proficiency in all possible domains of emergency surgery. Mackrill et al. [41] demonstrated that a standardized intervention, such as the laparoscopic appendectomy, has different outcomes if performed by registrars or consultants in Australia. As known, the growing experience is accompanied by a progressive amelioration of the surgical outcomes even after the formal learning curve is completed, meaning after approximately 20–30 cases.
Each minimally invasive procedure may be associated with a different learning process, so data about laparoscopic appendectomy cannot be generalized to laparoscopic cholecystectomy or robotic procedures. Furthermore, laparoscopic appendectomy is a procedure with repeated anatomy which does not include some of the skills required in laparoscopy such the suturing task. Differently, laparoscopic cholecystectomy introduces an anatomical variability without offering the suturing task to the trainer. The literature lacks studies investigating even the most common surgical emergencies that are nowadays approached by MIS, such as appendicitis, cholecystitis, gastrointestinal perforations, bowel occlusion, and incarcerated hernias. Only 13 articles were found in the present systematic review, and 85% of the treated cases consisted of a laparoscopic appendectomy.
It should also be considered that the learning process of an elective procedure may be extended to an emergency one, at least concerning the main technical aspects. Goksoy et al. [42] accurately investigated the learning curve in the elective setting of laparoscopic inguinal hernia repair, concluding that the spectrum of difficulty should be extended gradually and after the completion of the learning curve. This is confirmed by two recent series of robotic abdominal hernia repair where a small number of patients were treated for strangulated hernias. The number of emergency cases increased over the time, showing an extension of the surgeon’s indications and confidence [43, 44]. Kubat et al. [20] described the same progression in robotic single-site cholecystectomies, who suggested that the learning curve could be accelerated by first acquiring the skills necessary to complete elective cases. This concept is not new when considering the studies by Stam et al. [45] and Naguib et al. [46] who highlighted that laparoscopic colorectal resections for diverticular disease are technically challenging and more difficult than the resections performed for oncological indications in an elective setting. The study by Miskovic et al., based on an international multicenter analysis of 4852 cases, confirmed that the learning curve in colorectal surgery should include difficult cases like emergency surgery only in the later stages [47].
Type of recommendation: Expert opinion.
Strength of consensus: 77.8%
PS-2. To achieve proficiency, surgical proctoring and dedicated surgical fellowships may have a role that deserves further evaluation. Credentialing systems should be developed to ensure quality standards among different training programs.
While in the elective setting surgical proctorship is adopted, no literature is available concerning surgical proctoring in the emergency setting. This is not surprising considering the impossibility, by definition, of scheduling an emergency procedure. However, adopting new procedures or technologies should always be accompanied by proctoring to assist surgeons at the beginning of their new activity and support them in difficult situations even when the learning curve is completed [48,49,50,51,52]. In the emergency setting, telesurgery and telementoring including telestration, may have a valuable role that should be further evaluated and applied while using MIS techniques [10, 53,54,55,56].
There is an increasing trend toward post-residency surgical sub-specialization, which may become necessary to deliver expert care and master advanced surgical technologies that cannot be completely acquired during residency [57]. In the United States, subspecialization, which is pursued on a voluntary basis, is chosen by the majority of general surgeons before starting an independent activity [58]. The importance of fellowship certification has been recognized in several countries with a documented improvement in surgical outcomes [59, 60]. A good training program can reduce the learning time while maximizing the teaching process; even the simple observation of a standardized procedural step can shorten the learning curve [61] and promote proficiency [62,63,64,65].
In the field of emergency surgery, fellowships may represent valuable formal training that allows surgeons to achieve the additional experience needed to operate independently in emergency settings, particularly if the surgeon wishes to practice MIS. Another valid option, which
留言 (0)