
記住我
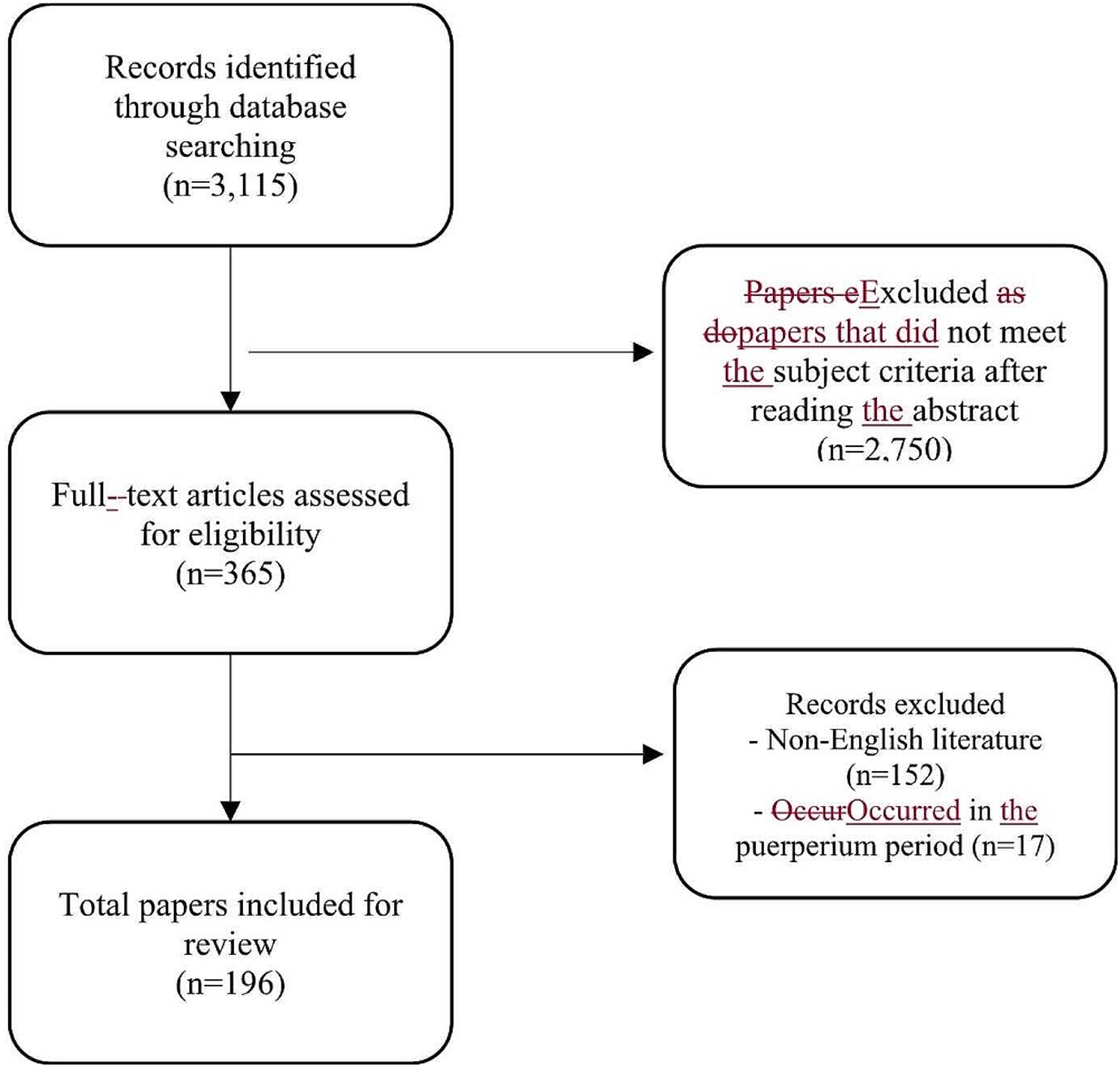
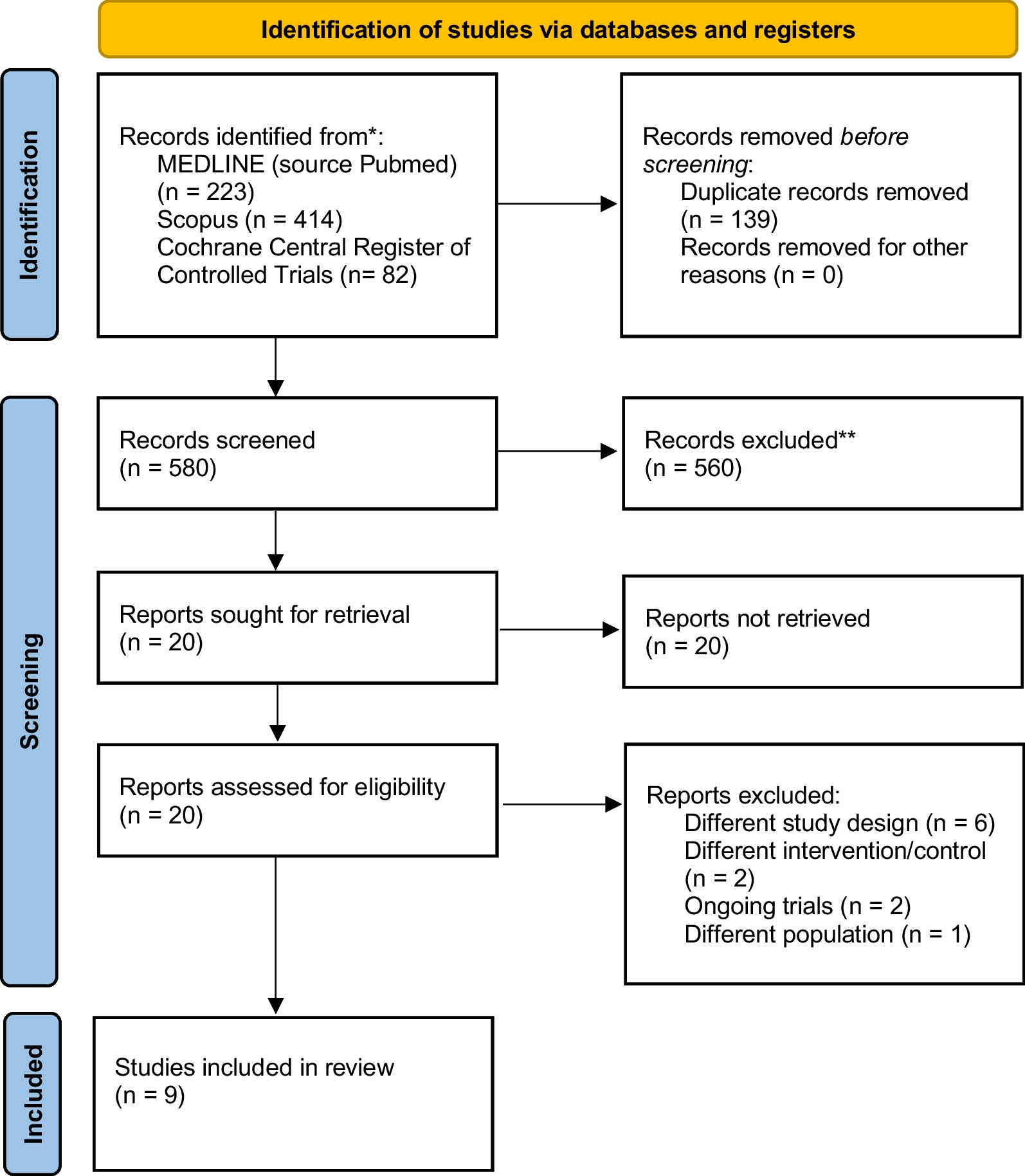


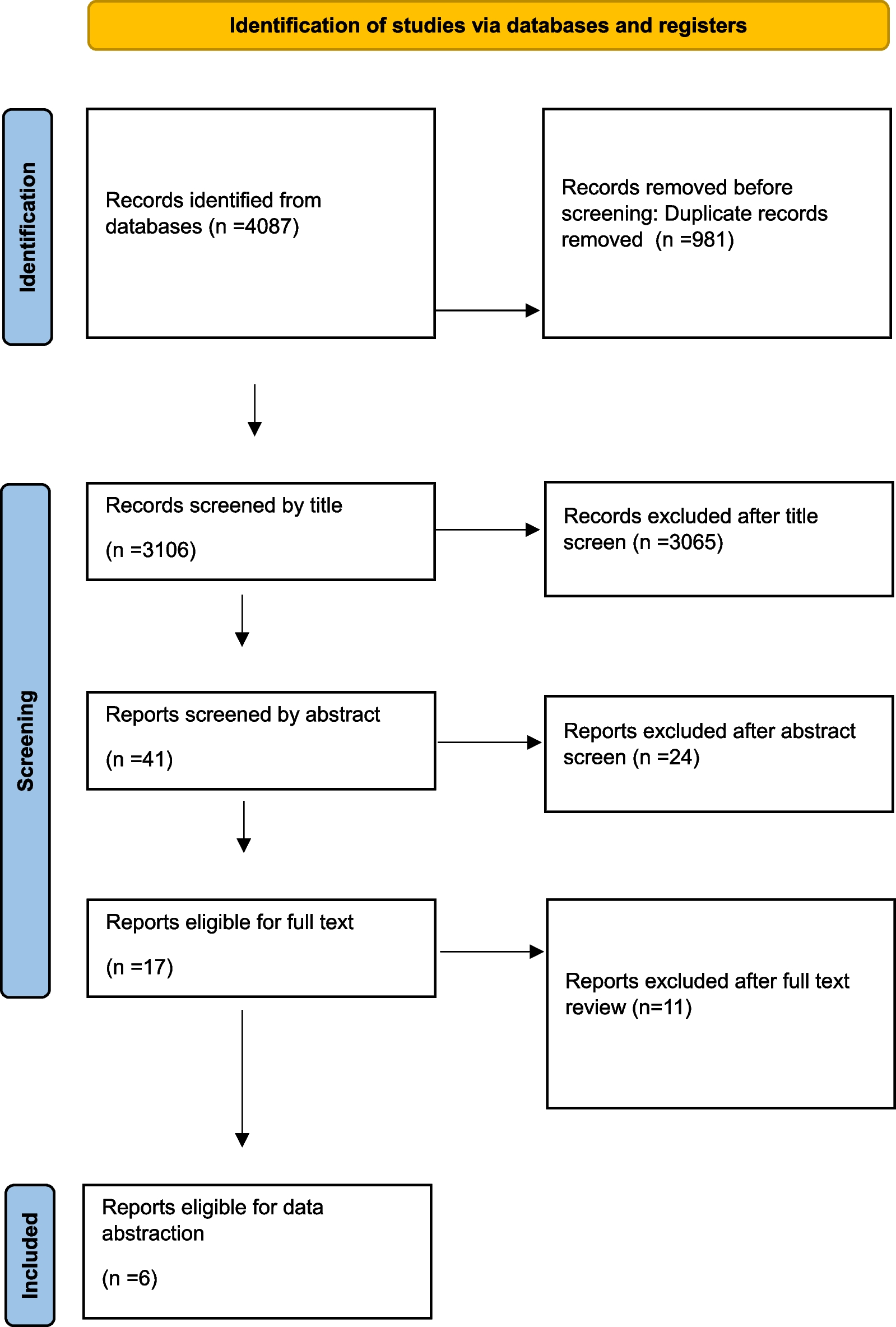
A total of 2025 articles were identified in accordance with the search strategy, and 131 duplicate citations were removed before screening. Of the remaining records, 1814 were excluded after title and abstract screening because of irrelevance. Seventy references were excluded after full-text screening. The reasons were as follows: abstract only (14 studies), uncontrolled studies (15 studies), traditional pairwise review and meta-analyses (11 studies), different topics did not meet the inclusion criteria because they were not clustered based on timing, approach and application of the step-up strategy (10 studies), protocol (8 studies), case reports (3 studies), studies reporting long-term follow-up outcomes of included studies (3 studies) and non-RCTs (2 studies). We did not identify any non-English articles that met our inclusion criteria. Finally, 10 RCTs were eligible for quality assessment and quantitative synthesis [39,40,41,42,43,44,45,46,47,48]. A PRISMA flowchart is presented in Fig. 1.
Fig. 1 Study characteristics
Study characteristicsThe 10 included studies were published from 1984 to 2021, with their respective studies starting from 1982 to 2019 across 6 countries [39,40,41,42,43,44,45,46,47,48] (Table 1). Ten studies [39,40,41,42,43,44,45,46,47,48] were designed as two-arm randomized controlled trials. A total of 570 participants with necrotizing pancreatitis were randomly assigned to one of the 8 interventions: 4 studies [39, 40, 47, 48] for early drainage (ED), 2 studies [47, 48] for delayed drainage (DD), 5 studies [39,40,41,42, 46] for early surgery (ES), 1 study [46] for early endoscopic step-up approach (EEU), 1 study [45] for delayed endoscopic step-up approach (DEU), 3 studies [42, 43, 45] for delayed surgical step-up approach (DSU), 1 study [44] for delayed endoscopic debridement (DE) and 3 studies [41, 43, 44] for delayed surgery (DS). The proportion of males in these studies ranged from 58 to 90.9%, and the mean age of patients ranged from 35.7 to 63 years. The etiology of necrotizing pancreatitis was reported in 7 studies [41, 43,44,45,46,47,48], and biliary pancreatitis was the most commonly identified etiology (53.2%, 235/442). The detailed baseline characteristics are shown in Additional file 1: Appendix S3.
Table 1 Characteristics of included trials within the network meta-analysisTen studies [39,40,41,42,43,44,45,46,47,48] reported morality. Eight studies [39,40,41,42,43,44, 46, 47] reported major complications. Nine studies [39, 40, 42,43,44,45,46,47,48] reported the length of hospital stay. Seven studies [42,43,44,45,46,47,48] compared bleeding, and six studies [43,44,45,46,47,48] reported organ failure, pancreatic fistula, visceral organ or enterocutaneous fistula, exocrine insufficiency, and endocrine insufficiency. (Additional file 1: Appendix S4).
Risk of bias in studiesThe quality assessment of individual studies is presented in Fig. 2. Using the Cochrane Collaboration tool, the overall risk of bias was low to moderate. Seven (70%) studies [41, 43,44,45,46,47,48] clearly described the generation of random sequences, and 6 (60%) studies [39, 40, 43, 45, 47, 48] had adequate allocation concealment procedures. The primary and secondary endpoints were rarely affected by the binding of participants and personnel. In addition, one study [48] had incomplete outcome data.
Fig. 2
Assessment of risk of bias in the trials used in analysis using the Cochrane Collaborations tool
Primary endpointThe mortality of necrotizing pancreatitis participants was reported in all 10 studies [39,40,41,42,43,44,45,46,47,48]. Figure 3a displays the network of all the interventions included in this network meta-analysis, the number of RCTs comparing different interventions and the sample size of each intervention. Table 2a presents the direct and indirect evidence using both traditional pairwise meta-analysis and Bayesian network meta-analysis. Accordingly, patients with ED and DD were more likely to obtain greater survival benefits than those who received ES from pairwise meta-analysis, (OR 2.56, 95% CI 2.06–25.03; OR 3.13, 95% CI 2.19–14.30, respectively) [49]. In addition, ES was discerned to offer a marked higher risk of mortality in comparison with DSU and DS (OR 2.56, 95% CI 1.05–6.69; OR 3.39, 95% CI 1.30–15.96, respectively). The remaining direct comparisons were statistically insignificant. However, based on the SUCRA scores, DE had the highest probability of mortality (73%), followed by DD (70%), EEU (65%), ED (63%), ES (54%), DEU (37%), DSU (24%) and DS (16%). In other words, the top three interventions ranked by safety were DS, DSU and DEU (Fig. 4a).
Fig. 3
Network of included trials comparing interventions for necrotizing pancreatitis. a Mortality. b Major complications. DD, delayed drainage; DE, delayed endoscopic debridement; DEU, delayed endoscopic step-up approach; DS, delayed surgery; DSU, delayed surgical step-up approach; ED, early drainage; EEU, early endoscopic step-up approach; ES, early surgery
Table 2 Direct and indirect evidence of primary endpoints in the network meta-analysisFig. 4
Ranking probability of mortality and major complications for different interventions for necrotizing pancreatitis. a Mortality. b Major complications. DD, delayed drainage; DE, delayed endoscopic debridement; DEU, delayed endoscopic step-up approach; DS, delayed surgery; DSU, delayed surgical step-up approach; ED, early drainage; EEU, early endoscopic step-up approach; ES, early surgery
A total of 9 studies [39, 40, 42,43,44,45,46,47,48] reported major complications (Fig. 3b). Multiple events in the same patient were considered one endpoint. All the data on the composite of major complications used in the analysis were mentioned in the original article. As given in Table 2b, major complications were more common in the ES group than in the EEU group (OR 5.13, 95% CI 1.46–18.08). For network meta-analysis, we found that DD was most likely to rank first for major complications rates (85%), followed by ED (77%), DE (66%), ES (56%), EEU (38%), DS (33%), DEU (24%) and DSU (21%), using SUCRA (Fig.
留言 (0)