


記住我









Aside from the NBSCC and satellite clinics, clinical genetics centers also have been created in each of the three main island groups in the Philippines (Luzon, Visayas, and Mindanao) to respond to the acute and long-term needs of patients diagnosed through the PNSP. Currently, the services of the NBSCCs and satellite clinics are conducted on an outpatient basis and are limited to non-critical care services.
1.2. The COVID-19 PandemicThe novel Coronavirus Disease 2019 (COVID-19) resulting from the SARS-CoV-2 virus has significantly affected all aspects of life worldwide since its discovery. Working to limit COVID-19 infections, quarantines and lockdowns have been common globally, and travel restrictions have existed both within and between countries. Recognizing the alarming spread and severity of infection, the World Health Organization (WHO) officially characterized COVID-19 as a pandemic on 11 March 2020 [8].In the Philippines, the national government declared an “enhanced community quarantine” for Metro Manila beginning 15 March 2020 until 14 April 2020. Public transportation, non-essential businesses, and classes at all levels were suspended to restrict mobility and exposure. The entire population, except for essential workers, was placed under “stay at home” orders [9], later made more stringent by extending the quarantine to the entire island of Luzon [10]. In late June, Cebu City was identified as the epicenter of COVID-19 in the Philippines and a “hard lockdown” was initiated there [11]. In response to these limitations, the economy suffered markedly resulting in significant unemployment and extensive business closures.Healthcare also was impacted. In response to the extreme increase in patients suffering from COVID-19, medical priorities were immediately shifted to respond to the health emergency. Outpatient services were reduced or discontinued, and elective procedures and surgeries were often forced to be deferred [12]. Public health services such as vaccination campaigns were postponed, increasing the risk of outbreaks of vaccine-preventable diseases in the Philippines. Unlike some countries where healthcare access for regular needs, including antenatal care and newborn screening, were reportedly unavailable, NBS continued [13].Reported here are the results of a survey of NBSCCs that investigates the impact of COVID-19 on the services and, potentially, the health of newborns diagnosed and referred to NBSCCs during the pandemic.
2. Materials and MethodsFollowing the initiation of the community quarantine, a situation assessment survey to be completed online was distributed to the 14 NBSCCs in July 2020. An informed consent form was included in the distributed material and its completion was required prior to completing the survey. Survey questions concerned the impact of the pandemic on the NBSCC activities including challenges encountered and strategies implemented to address them. Survey findings were thematically analyzed using Braun and Clarke’s thematic analysis framework [14]. Data analyses were performed independently by four investigators from the National Institutes of Health’s Newborn Screening Reference Center. Following the analyses, NBSCC respondents and the Newborn Screening Reference Center analysts discussed the survey responses and reached a consensus as to appropriate and harmonized descriptions of the challenges encountered and the actions required to overcome them.To compare NBSCC operations activities in pre-pandemic years (2018, 2019) and pandemic years (2020, 2021), patient interaction data from each NBSCC were obtained and analyzed. Data included annual and cumulative data for endorsed patients and were adjusted by excluding patients who died or were discharged after having been determined not to have the disorder (based on findings of an accredited specialist). It is the goal of the NBSCC to make contact with all endorsed patients at least once in a six-month period. Patients with whom contact is not made after numerous attempted contacts by the NBSCC and additional follow-up attempts by the relevant CHD are classified as “unresponsive”.
3. ResultsThere were 14 responses to the July 2020 survey, one from each NBSCC. The responses were analyzed and thematically categorized as follows: (1) Challenges to the NBSCC’s operational capacity; (2) challenges with patient communication; and (3) challenges with staff and patient safety.
3.1. Challenges to the NBSCC’s Operational CapacityAs a result of COVID-19, face-to-face clinic consultations were temporarily halted in 85.7% of the continuity clinics during the pandemic. The primary reason reported was the loss of manpower at the NBSCC due to the hosting institution’s decision to close its clinics. As a result of travel restrictions, 57.1% of NBSCCs also reported difficulties in distributing medical foods and medications. A reduction in the activities conducted by the continuity clinics such as subspecialty clinics and lay fora (patient education seminars) was reported by 28.6% of the NBSCCs.
3.2. Challenges with Patient CommunicationsPatient communications were a common challenge faced by the NBSCCs during the pandemic. Difficulty in patient recall was reported by 50.0% of the NBSCCs. In order to minimize patient contact, telemedicine consultations were initiated across all NBSCCs and quickly became an effective means of patient contact. Telemedicine and telegenetics visits were readily accepted as an alternative to face-to-face clinic visits, but these were not without difficulties [15]. Three continuity clinics (21.4%) reported difficulty conducting telemedicine consultations due to poor internet connections or lack of proper equipment to conduct consultations. 3.3. Challenges to Health Staff and Patient SafetyOnly one continuity clinic (7.1%) reported difficulties with staff and patient safety during the pandemic. The remaining NBSCCs reported that any potential difficulties were overcome using telemedicine. Over a period of three months, the 14 continuity clinics saw a total of 379 patients via telemedicine consultations.
3.4. NBSCC StatisticsAnnual and cumulative NBSCC data for 2018–2021 are presented in Table 1. A total of 6519 endorsed patients were under the supervision of the NBSCCs by the end of 2021. An increase in endorsements of 146% occurred between 2019 and 2020 corresponding to the 2019 expansion of NBS from 6 to 29 conditions [16,17]. The preponderance of the additional endorsements was from hemoglobinopathy and thalassemia cases. The decrease in the number of endorsed patients in 2021 corresponds to the decrease in national newborn coverage from 80.4% in 2020 to 70.7% in 2021 [18]. Throughout the four years, the number of patient contacts rose, keeping pace with the added endorsements. In 2018 and 2019, the contact percentages contacted were 70.6% and 70.2%, respectively, and for 2020 and 2021, these percentages increased to 74.9% and 76.8%. While management reorganization during this period likely contributed to the increased contact efficiency, it is clear that during the pandemic, patient contact services were not negatively affected and contact percentages improved slightly. The decrease in the percentages of unresponsive patients across the four years likely reflects both system improvements resulting from the management changes alluded to previously and decreased mobility of families because of the pandemic’s travel restrictions. 4. DiscussionSince the beginning of the pandemic, the NBSCCs have encountered new and unique issues and concerns affecting their operations. These in turn have affected the delivery of quality services to patients and their families. As a result of the imposed quarantine, modes of transport were limited, and transportation for both staff and patients was almost nonexistent. Strict border controls were enacted between provinces, challenging the way in which medical foods, supplies, and medicines could be transported. In some cases, medical items such as NBS specimens, which were transported to a provincial border, could be picked up by an ambulance on the other side of the border for transport to a medical facility. Patient movements were also possible in this way. Metabolic patients who required blood draws for monitoring also experienced difficulties in getting to NBSCCs or Newborn Screening Facilities (NSFs). For certain patients, such as those with endocrine disorders, CH, and CAH, monitoring laboratory services were only available at a limited number of facilities.
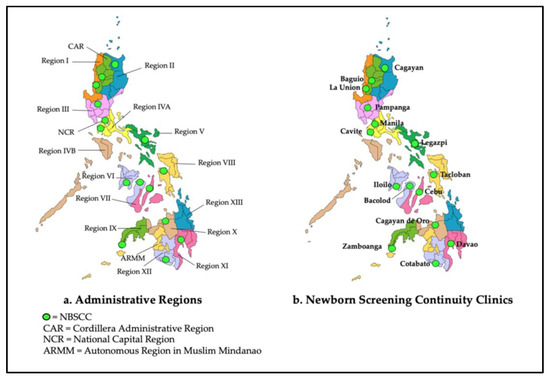
As government hospitals, 13 of the 14 host facilities of the NBSCCs were designated as COVID-19 Referral Centers by the DOH. Only one facility was not: West Visayas State University Medical Center (Iloilo) (see Figure 1). As referral centers, the organization of the host facilities was modified, and operations were streamlined to adequately respond to the pandemic. Of necessity, this included the temporary closure of outpatient services, including the NBSCCs.In addition to the general categories of NBSCC challenges noted above, Table 2 summarizes some of the specifics of these challenges and the strategies employed to address them. Contingency plans were executed and there was coordination with the different stakeholders (i.e., Newborn Screening Centers (NSCs), Local Government Units, DOH-CHDs, Clinical Genetics Unit, and satellite clinics) to assure continued delivery of services to patients despite the limitations caused by the pandemic. NBSCCs utilized telemedicine consultations whenever possible as a substitute for face-to-face visits. The limitations of telemedicine visits were explained to the parents and caregivers prior to the visit. During the pandemic, five NBSCCs relied solely on telemedicine consultations while five others used both face-to-face and telemedicine consultations. In the latter case, telemedicine consultations were reserved for patients who did not need urgent or emergent medical care. All telemedicine encounters were well documented.Despite having well-thought-out contingency plans for continuing operations in case of emergencies, some NBSCCs encountered difficulties in their implementation. For example, cellular phone calls, text messages, and telemedicine visits all rely on good Internet connections. Unfortunately, some areas of the country have poor Internet connectivity, which interfered with some transmissions. Additionally, some parents were not sufficiently familiar with the use of cell phones and the Internet, which slowed telemedicine services. For facilities that used face-to-face consultations, adequate clinic space was often an issue because of increased COVID-19 cases, the need for increased numbers of hospital beds, and related space requirements. Caregivers’ apprehensiveness about contracting the virus also resulted in a decrease in the number of patients attending clinics.
Coordination with other stakeholders to assure the delivery of services to NBSCC patients was a continuing consideration. Some NBSCCs requested assistance from the Local Government Units and DOH-CHDs to help in mobilizing healthcare workers (i.e., Barangay Health Workers, Rural Health Units, and health centers) to assist in caring for NBSCC patients. Care concerns included (1) the distribution of medications, medical formulas, and related supplies; (2) documentation of anthropometrics; (3) monitoring medical indicators for metabolic patients; and (4) assuring compliance with treatment.
5. ConclusionsThe COVID-19 pandemic has provided the NBSCCs with opportunities to strengthen their ties with other NBS stakeholders and to think of creative ways to achieve their goals and objectives. The modified NBSCC contingency plans resulting from the challenges encountered during the COVID-19 pandemic can be used as references to better prepare for future disasters and/or pandemics. Given that the COVID-19 viral threat continues, along with the possibility of other unexpected events, regular and continuous evaluation and contingency planning are essential to continuing quality services for optimum patient care.
In conclusion, continuing care for patients under NBSCC oversight is essential for achieving optimum health outcomes. The COVID-19 pandemic resulted in new and innovative strategies for addressing challenges to NBSCCs’ operational capacity, mechanisms for patient communication, and adequate safety of staff and patients. Based on NBSCC data, patient services were continued at the same level during the pandemic as before and fewer patients were lost-to-follow-up. The work ethic and dedication of NBSCC staff members resulted in these continued high levels of service.
Author ContributionsConceptualization, E.B.G.M., C.D.P., B.L.T.J., M.E.A., K.A.R.P. and F.D.E.B.; methodology, E.B.G.M., M.E.A., K.A.R.P., F.D.E.B., I.R.C.V.-A., G.D.T., S.B.G., M.V.L.M., L.M.S.M.A.-A., M.A.F.-D., K.J.V.V., M.R.A.S.R.B., N.G.H., M.S.E., R.D.O.-O., G.J.B. and M.C.N.B.-E.; validation, E.B.G.M., C.D.P. and B.L.T.J.; formal analysis, E.B.G.M., C.D.P., and B.L.T.J.; data curation, E.B.G.M., M.E.A. and K.A.R.P.; writing—original draft preparation, E.B.G.M., M.E.A., K.A.R.P., F.D.E.B. and B.L.T.J.; writing—review and editing, E.B.G.M., M.E.A., B.L.T.J., I.R.C.V.-A., G.D.T., S.B.G., M.V.L.M., L.M.S.M.A.-A., M.A.F.-D., K.J.V.V., M.R.A.S.R.B., N.G.H., M.S.E., R.D.O.-O., G.J.B. and M.C.N.B.-E. All authors have read and agreed to the published version of the manuscript.
FundingThis research received no external funding.
Informed Consent StatementInformed consent was obtained from all subjects involved in the study.
Data Availability StatementAll data generated or analysed during this study are included in this published article.
AcknowledgmentsThe authors thank the following NBSCC nurses for their dedicated long-term care of patients, particularly during the COVID-19 pandemic: Vanessa Mabalo, Ma. Cristina Calimag, Florenz Ronielo Nastor, Ma. Cesca Retomarta, Jhonalyn Bantigue, Gellie Ann Golfo, Mary Joy Rebueno, Diana Pondevida, Lucille Jra Largo, Eldeliza Campomanes, Iris Tomas, Udall Armand Cabading, Margaret Sibug, and Juledene Mendoza. The authors also thank Christine Mae Avila for their assistance in manuscript preparation.
Conflicts of InterestThe authors declare no conflict of interest.
AbbreviationsCAHCongenital adrenal hyperplasiaCHCongenital hypothyroidismCHDCenter for Health DevelopmentCOVID-19Coronavirus Disease 2019DOHDepartment of HealthNBSNewborn bloodspot screeningNBSCCNewborn screening continuity clinic (long-term follow-up)NSCNewborn Screening Center (screening laboratory)NSFNewborn Screening Facility (screening specimen collection site)PNSPPhilippine Newborn Screening ProgramReferencesPadilla, C.D.; Domingo, C.F. Implementation of newborn screening in the Philippines. Philipp. J. Pediatr. 2002, 51, 2–10. [Google Scholar]Padilla, C. Newborn screening in the Philippines. Southeast Asia J. Trop. Med. Public Health 2003, 34 (Suppl. 3), 87–88. [Google Scholar]Therrell, B.L. US newborn screening policy dilemmas for the twenty-first century. Mol. Genet. Metab. 2001, 74, 64–74. [Google Scholar] [CrossRef] [PubMed]Department of Health. Administrative Order 2014-0035—Implementing Guidelines on the Setting-Up of Newborn Screening Continuity Clinics. Available online: https://newbornscreening.ph/images/stories/ResourcesDOHPolicies/AO%20No.%202014-0035.pdf (accessed on 2 September 2020).Padilla, C.D.; Therrell, B.L.; Panol, K.A.R.; Suarez, R.C.N.; Reyes, M.E.L.; Jomento, C.M.; Maceda, E.B.G.; Lising, J.A.C.; Beltran, F.D.E.; Orbillo, L.L. Philippine Performance Evaluation and Assessment Scheme (PPEAS): Experiences in newborn screening system quality. Int. J. Neonatal Screen. 2020, 6, 95. [Google Scholar] [CrossRef] [PubMed]Newborn Screening Reference Center. Manual of Operations for Newborn Screening Continuity Clinics. Available online: https://www.newbornscreening.ph/images/stories/ResourcesTechnicalDocuments/nbsccmanops.pdf (accessed on 17 October 2022).Department of Health—National Center for Disease Prevention and Control. Memorandum on Newborn Screening Grant for Pediatric Endocrinologists and Clinical Geneticists. Available online: https://newbornscreening.ph/images/stories/ResourcesDOHPolicies/doh.newborn%20screening%20grant%20for%20pediatric%20endocrinologists%20and%20clinical%20geneticists.pdf (accessed on 17 October 2022).World Health Organization. WHO Characterizes COVID-19 as a Pandemic. 31 July 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed on 2 September 2020).Legaspi, G.D.; Omar, A.T., 2nd; Baticulon, R.E.; Salonga, A.E.M.; Gaddi, M.J.S.; Hong, M.A.C.; Seng, K.S.; Khu, K.J.O. Letter to the Editor “Service and Training during the COVID-19 Pandemic: Perspectives from a Neurosurgical Center in the Philippines”. World Neurosurg. 2020, 139, 741–743. [Google Scholar] [CrossRef] [PubMed]Amit, A.M.L.; Pepito, V.C.F.; Dayrit, M.M. Early response to COVID-19 in the Philippines. West. Pac. Surveill. Response J. 2021, 12, 56–60. [Google Scholar] [CrossRef] [PubMed]Dancel, R. The Straits Times. Cebu City Looms as Philippines’ New COVID-19 Epicentre. Available online: https://www.straitstimes.com/asia/se-asia/cebu-city-looms-as-philippines-new-covid-19-epicentre (accessed on 22 November 2022).Cole, B. National Academy of Social Insurance. The Impact of the Covid-19 Pandemic on access to health care. Health Policy Brief. 2020, 17, 1–31. [Google Scholar]Hirabayashi, K.; UNICEF East Asia and Pacific. The Impact of COVID-19 on Routine Vaccinations. Available online: https://www.unicef.org/eap/stories/impact-covid-19-routine-vaccinations (accessed on 22 November 2022).Braun, V.; Clarke, V. Using thematic analysis in psychology. Qual. Res. Psychol. 2006, 3, 77–101. [Google Scholar] [CrossRef]Tumulak, M.J.R.; Pascua, A.V.; Jover, E.J.M.; Guerbo, R.J.; Canoy, G.M.R.; Laurino, M.Y. Genetic counseling in the time of COVID-19: The Philippine experience with telegenetics. J. Genet. Couns. 2021, 30, 1285–1291. [Google Scholar] [CrossRef] [PubMed]Padilla, C.D.; Therrell, B.L., Jr.; Alcausin, M.M.L.B.; de Castro, R.C., Jr.; Gepte, M.B.P.; Reyes, M.E.L.; Jomento, C.M.; Suarez, R.C.N.; Maceda, E.B.G.; Abarquez, C.G.; et al. Successful implementation of newborn screening for hemoglobin disorders in the Philippines. Int. J. Neonatal Screen. 2021, 7, 30. [Google Scholar] [CrossRef] [PubMed]Padilla, C.D.; Therrell, B.L., Jr.; Alcausin, M.M.L.B.; Chiong, M.A.D.; Abacan, M.A.R.; Reyes, M.E.L.; Jomento, C.M.; Dizon-Escoreal, M.T.T.; Canlas, M.A.E.; Abadingo, M.E.; et al. Successful implementation of expanded newborn screening in the Philippines using tandem mass spectrometry. Int. J. Neonatal Screen. 2022, 8, 8. [Google Scholar] [CrossRef] [PubMed]Newborn Screening Reference Center. Newborn Screening Statistics: National Coverage 2021. Available online: https://newbornscreening.ph/index.php?option=com_content&view=article&id=83:nbs-statistics&catid=32:statistics&Itemid=57 (accessed on 21 December 2022).Figure 1. Administrative Regions of the Philippines and Newborn Screening Continuity Clinic Locations.
Figure 1. Administrative Regions of the Philippines and Newborn Screening Continuity Clinic Locations.
Figure 2. Short- and long-term follow-up flow for patients identified through newborn screening.
Figure 2. Short- and long-term follow-up flow for patients identified through newborn screening.
Table 1. Annual and Cumulative Data from Newborn Screening Continuity Clinics 2018–2021.
Table 1. Annual and Cumulative Data from Newborn Screening Continuity Clinics 2018–2021.
CategoryYear2018201920202021Annual number of endorsed newborns (referred from NSCs)4594761171643Cumulative endorsed newborns (long-term care monitoring) 4229470558766519Annual number of expired cases (died while in long-term care)10224617Annual number discharged (diagnosed clinically normal)1718298Actual newborn census [endorsed − (expired + discharged)]3991442755236141Number contacted (contact with patient made within 6 months)2819310741384717Percentage contacted [(number contacted/actual census) × 100%]70.6%70.2%74.9%76.8%Annual unresponsive patients (patient contact lost for over 6 months)3041486539Table 2. Strategies initiated to address some of the challenges posed by the pandemic.
Table 2. Strategies initiated to address some of the challenges posed by the pandemic.
ChallengesStrategiesLimited or complete disruption of clinic hoursGuidelines from the Philippine Pediatric Society and University of the Philippines Manila were distributed defining the conduct of telemedicine consultations
Collaboration with subspecialists was continued remotely through available telemedicine platforms
The utilization of telemedicine consultations were maximized through use of online platforms, phone calls and SMS for continued patient follow-up.
Distribution of medical food, supplies, and medicineSafety of both NBSCC staff and patients during face-to-face consultationsDisclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content.
留言 (0)