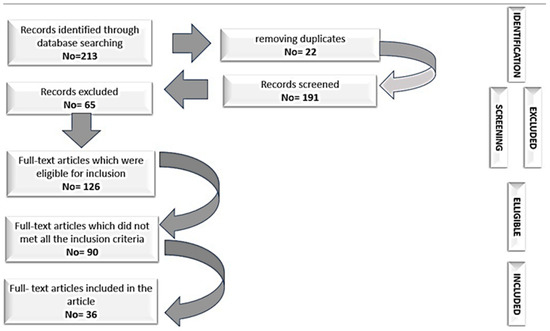
Figure 1.
The selection process.
![Clinpract 13 00002 g001]()
Table 1.
Neurological deficit assessment scales.
Table 1.
Neurological deficit assessment scales.
Nr.ScaleYearWhen to UseAdvantageLimitationReferences1.Scala Frankel1969- Neurological deficit: A–E
- A (complete neurological damage)
- E (clinically normal)- The first publicly available neurological scale
- Synthetic
- Clinically easy to use- Unclear differentiation between grade C and D
- Subjective nature in judging “usefulness” of any remaining motor movements
- The level of the injury is not incorporated in the classification
- Limited responsiveness to subtle neurological improvements during recovery.[
22,
23,
24,
25]2.Bracken Scale1978- 2 subscales: 7 sensitive items and 5 motor items
- Acute hospitalization
- Clinically rarely used [
26,
27]3.Lucas and Ducker’s Neuro-trauma Motor Index1979- Evaluates 23 muscles- Predictive value of patient’s functional independence- Heavy calculations in the evaluation of motor function[
28,
29]4.Yale Scale1981- Tests sensory and motor function- Numerical grading of selected functions below the level of the lesion- The multiple calculations make it difficult to use in current practice[
29,
30]5.Sunnybrook Scale1982- 10 degrees with motor and sensory deficit-Differentiation of sensory and motor deficits between the equivalent degrees C and D from Frankel scale- Multiple calculations[
31,
32,
33]6.American Spinal Injury Association (ASIA)1984- Derived from the Frankel scale
- Designated as an assessment tool to classify baseline neurological impairment.- Classifies neurological injuries based on a practical way to admission
- Provides information regarding the improvement of the patient’s condition during the follow-up- Does not reveal the objective anatomic origin of the causal injury
- Does not decide injury severity[
34,
35,
36,
37]7.Botsford
Scale1992- Assesses motor and sensory function, rectal tone and bladder control
- The motor score is obtained by testing 15 key muscles scored between 0–5 points (maximum 75 points)
- The maximum sensitive score is 10 points
- Anal tonus 10 points
- Bladder tonus 5 points- Introduces anal sphincter and bladder tonus control testing into the neurological assessment, as a measure of outstanding functionality
- Can be used at the patient’s bedside
- It does not require special tests other than those performed in a routine clinical neurological examination
- Motor function is assessed in a functional assessment system- Few clinical studies have used this scale.[
38,
39]
Table 2.
Functional evaluation scales of SCI.
Table 2.
Functional evaluation scales of SCI.
Nr.ScaleYearWhen to UseAdvantagesLimitationReferences1Barthel Index (BI)1965- Functional evaluation of patients with stroke and TVM
- Score between 0–100 points, evaluates the tone of the anal sphincter, bladder tonus
- Personal hygiene
- Using the toilet
- Food
- Transfer from bed to cart and vice-versa
- Mobility
- Dressing
- Climbing steps
- Bathing- Evaluates daily activities and some physiological functions
- Easy to useThe examination time is long[
40]2Modified Barthel Index (MBI)1989- Allows anyone to assess the activities of daily living- Measures independence in ADLEvaluates only stroke patients[
41,
42]3Functional Independence Measure
(FIM)1987- Consists of 13 motor and 5 cognitive items with a score between 18 and 126 points
- Divided into main categories and subcategories: self-care (feeding, brushing, bathing, dressing, toileting) sphincter control (bladder and anal), transfer mobility (transfer from bed to chair or wheelchair, from toilet to wheelchair, using the shower), locomotion (walking/wheelchair, stairs), communication (understanding, expression), social cognition (social interaction, problem solving, memory)- Measures global independence during specific functional tasks
- Records progress results
- Specifies the patient’s functional mobility and independence
- More sensitive, detailed and comprehensive compared to the Barthel index, socio-economically meaningful improvementsLong examination time[
43,
44,
45]4Quadriplegia Index of Function QIF1980- Quadriplegic patients- More sensitive and reliable than the Barthel IndexUse only in quadriplegic patients[
46,
47]5Spinal Cord Independence Measure
(SCIM)1997- Functional categories: selfcare (subscore 0–20), breathing and sphincter management (0–40) and mobility (0–40);
- Final score between 0 and 100- Disability scale developed specifically for patients with spinal cord injuries, to make functional assessments sensitive to changes occurring in the follow-up of patients with para- or tetraplegiaUse only in SCI[
48,
49,
50]6Walking Index for Spinal Cord Injury WISCI2000- Originally described with 19 levels, it was revised and expanded in 2001 to include 21 levels, thus resulting in the WISCI II for use in clinical trials- Measures improvement in walking after SCICannot be used in clinical trials[
51]7Walking Index for Spinal Cord Injury II
(WISCI II)2001- Improvements in walking following SCI- Incorporates physical assistance, the use of dental aids and appliances to be able to adapt to the needs of patients with varying degrees of post SCI impairment
- Self-explanatoryDoes not take psycho-metric properties into account[
52,
53]8Spinal Cord Injury Functional Ambulation Inventory (SCI-FAI)2001- 6 parameters: weight shift, step width, step rhythm, step height, foot contact and step length
- Each limb is scored individually, so the same score for each limb indicates symmetry between bilateral limbs, the patient is assessed from the frontal plane, then sagittal
- Divided into 3 areas: walking (6 parameters and symmetry between the lower limbs)—maximum score of 20 points, 14 points for the use of assistive devices and 5 points for the walking mobility score- Observational assessment of walking ability in people with SCI
- Can be performed directly or from video recordings- The three scores of the SCI-FAI instrument are intended to measure different domains of functioning
- Not relevant to combine them to obtain a global score[
54,
55]
Table 3.
Scale for the evaluation of the neurological deficit and functional assessment of patients with SCI.
Table 3.
Scale for the evaluation of the neurological deficit and functional assessment of patients with SCI.
Nr.ScaleYearWhen to UseAdvantagesLimitationReferences1.American Spinal Injury Association/International Medical Society of Paraplegia Standards (ASIA/IMSOP)1992- Assesses sensory level, motor function
- Incorporated in the Functional Independence Measure (FIM)- Functional status based on their ability to perform ADL plus social interaction
- Good discrimination in severity of SCI
- Predictability of outcome- Weak interobserver reliability for the grading of incomplete SCI[
56]









留言 (0)