
記住我




In this prospective single-center study in a tertiary care hospital, we analyzed the first 50 patients between July 2017 and November 2020 who underwent SNM therapy using the “H technique.” All included patients were diagnosed with constipation or FI and FI was defined as the involuntary loss of solid or liquid stool or gas and further assessed by the Vaizey incontinence score [4]. Causes of incontinence included posttraumatic, idiopathic and multifactorial origins. The posttraumatic group comprised patients with low anterior resection syndrome (n = 12, 63%), sphincter injuries (n = 5, 27%), and other anal surgeries (n = 2, 10%). Constipation was defined by the Rome III criteria [2, 5]. Patients were chosen for SNM treatment if conservative treatment strategies had failed. These included lifestyle and diet changes, pelvic floor exercise, unresponsive to laxatives and prokinetics. The application of SNM treatment in each patient population was according to the international guidelines published by Goldman et al. [6]. All operations were performed or supervised by a single colorectal surgeon. Demographic data and overall pelvic function were recorded for all patients using a standardized questionnaire at baseline and during the last follow-up.
Bowel function was evaluated in more detail by the obstructed defecation score, which ranged from 0 (no symptoms) to 31 (very severe symptoms) [7]. The severity of FI was assessed using the Vaizey incontinence score: 0 points indicates no incontinence and 24 points the worst incontinence [4]. Preoperative and postoperative evaluation of a patient’s quality of life was assessed using the SF-12 survey, which includes a mental component score (MCS-12) and a physical component score (PCS-12) [8]. Evaluation of QoL regarding urinary incontinence was assessed by the international consultation on incontinence urinary incontinence short form (ICIQ-SF), using a score scale of 0–21 [9]. Over 50% improvement of all scores between the baseline and the last follow-up visit was considered a successful outcome.
Patients subjected to SNM treatment underwent a two-step procedure. First, diagnostic stimulation was conducted over 14–21 days. Over 50% of self-reported improvement from the baseline condition was considered a positive criterion for permanent implantation of the neurostimulator. Complications and re-operations were assessed after up to 40 months of follow-up. All patients received an InterStim SNM device (Medtronic, Minneapolis, MN, USA).
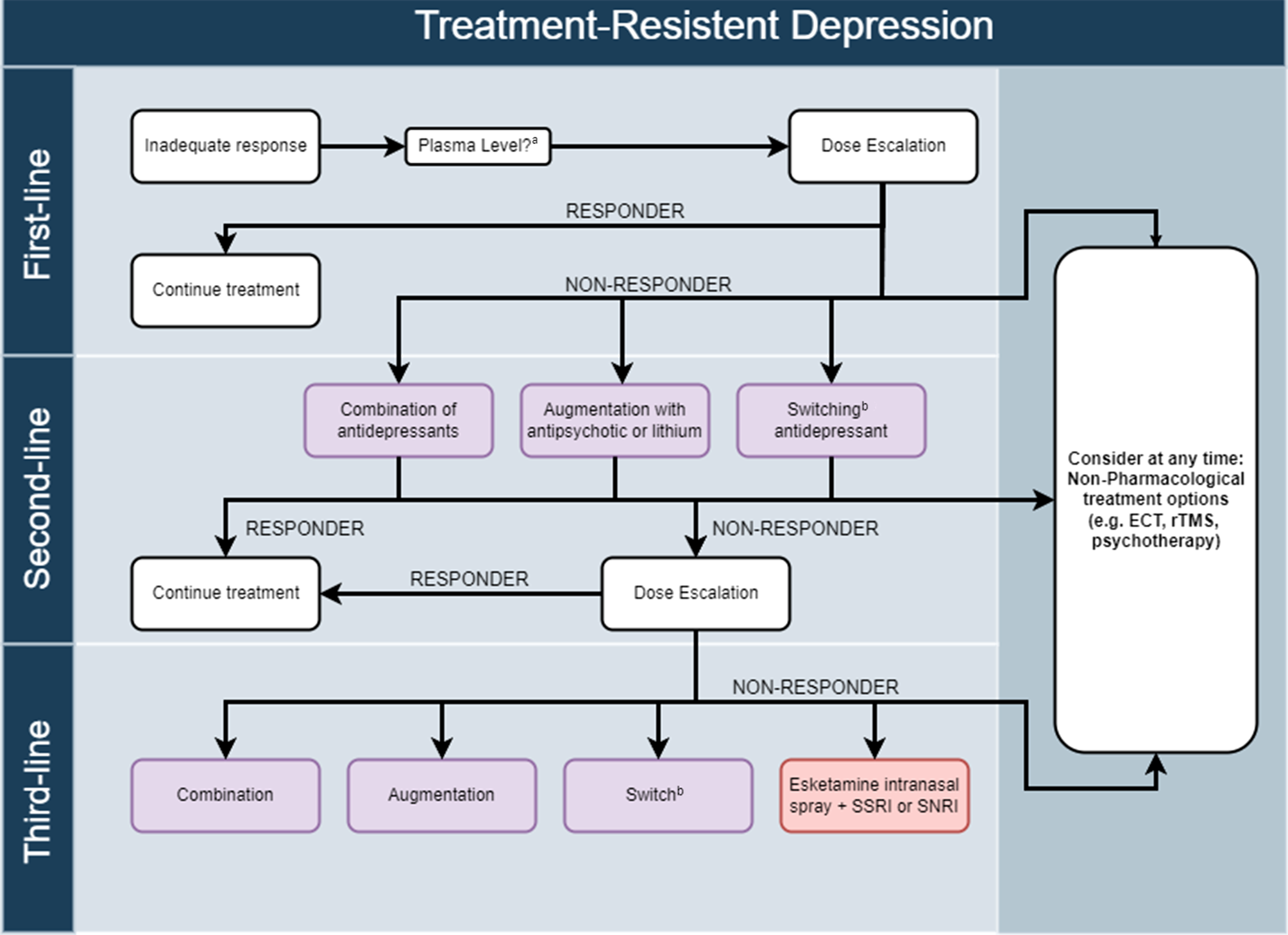
The “H” electrode placement techniqueThe “H” technique for percutaneous electrode placement has been standardized to minimize failed treatment attempts due to technical shortcomings [2]. For the procedure, the patient is placed in the prone position, with the pelvis supported to minimize lumbar lordosis. An X‑ray of the sacrum then helps locate the landmarks, the sacral foramina and the sacroiliac joint that guide needle placement. The vertical lines connecting the medial edges of the foramina and the horizontal line connecting the lower edges of the sacroiliac joint produce an “H.” These lines are marked on the skin, and the intersecting points represent the ideal entry point for needle placement in S3. The needle is then advanced, with lateral X‑rays used for guidance and minor positioning corrections. The needle placement is tested with stimulations to maximize the response. This stimulation can also elicit characteristic movements, depending on the sacral foramen. Under fluoroscopic control, the needle is then replaced by a guidewire and a dilatator, followed by the electrode (Fig. 1).
Fig. 1
The “H” technique for percutaneous electrode placement is presented. The patient is placed in prone position. a An X‑ray of the sacrum helps to locate the landmarks that guide needle placement. The landmarks are the sacral foramina a,b and the sacroiliac joint. b The vertical lines connecting the medial edges of the foramina and the horizontal line connecting the lower edges of the sacroiliac joint produce an “H”. The lines are marked on the skin and the intersecting points represent the ideal entry point for placement of the needle in S3. c The needle is then advanced, with lateral X‑rays used for guidance. As presented by X‑ray marked by red circle. d A guidewire is introduced over the needle followed by a dilatator after the needle is removed. e The electrode is placed through the dilatator
Statistical analysisAbsolute and relative frequencies describe categorical variables. The corresponding 95% confidence intervals (95% CI) were computed according to the method of Wilson [10]. The association between two categorical variables was tested by a χ2-testor Fisher’s exact test for small group sizes. Continuous variables are described by median, minimum, and maximum based on their skew distributions. Furthermore, the impact of various factors, including sex, BMI, diagnosis, age, and comorbidities on the success rate of SNM treatment were analyzed by logistics regression. The Wilcoxon signed-rank test assessed comparisons between preoperative and postoperative scores. All statistical calculations were performed without data imputation. For all tests, a two-sided p-value of ≤ 0.05 was considered significant. Data obtained were evaluated statistically using IBM SPSS Statistics (version 25, SPSS Inc., Chicago, IL, USA).
Ethics approvalThis study was approved by the ethics committee of the Medical University of Vienna (EK Nr. 1267/2020) and conducted according to the principles of the Helsinki Declaration and good clinical practice.
留言 (0)