
記住我
What is known about the topic?
From patients’ perspectives, noise is the most significant contributing factor for poor sleep quality in ICUs. Sleep deprivation in ICUs is associated with difficulties in rehabilitation, impaired immune function, delayed weaning from ventilation, a higher incidence of delirium, and longer lasting neurocognitive changes. Noise and light reduction strategies in ICUs are recommended, with repercussions on reducing the incidence of delirium and environmental noise.What does this article add?
Controlling noise in the ICU, as recommended by the WHO, is challenging for professionals working in these places. Implementing best practices for noise control in ICUs should include strategies to engage people in behavioural change. Staff training concerning best practice compliance for sleep hygiene should be continuous. IntroductionTranslating knowledge into practice often occurs over years or decades, promoting a gap that results in the high or incorrect use, or underuse, of evidence, which negatively impacts health safety, quality, and costs.1 The nursing field is essential in reducing the gap between research and practice, especially in building knowledge about successful processes for adopting evidence and sustainably implementing evidence in routine clinical practice1 – a process known as implementation science. Implementation science can be defined as ‘the scientific study of methods to promote the systematic uptake of research findings and other evidence-based practices into routine practice, and, hence, to improve the quality and effectiveness of health services’.2 Implementing best practices in healthcare settings is vital for healthcare institutions to provide care based on the best available evidence, given their importance. Further, an implementation model increases the probability of successfully translating knowledge and its sustainability over time.1
In the ICU, clinical conditions and environmental factors are associated with sleep deprivation in patients,3 with a lack of restorative sleep3,4 and a high prevalence.5 Moreover, approximately 50% of ICU patients’ sleep time commonly occurs during the daytime, with more sleep time in the light stages of sleep; this is related to the environment and ICU care routines.6 Patients discharged from the ICU exhibited poor sleep quality, with slight improvement after 6 months.7 Sleep deprivation in these environments is associated with difficulties in rehabilitation, impaired immune function, delayed weaning from ventilation, higher incidence of delirium, and longer lasting neurocognitive changes.8
Sleep deprivation is related to physiological factors, such as underlying disease, physical and psychological stress, age-related changes, pain, and worry, and environmental factors, such as discomfort from care interventions, noise related to the tone of voice of the healthcare providers, excessive lighting, and monitoring alarms.8,9 Among these, noise, according to patients, is the most critical disruptive factor in sleep.10,11 According to the recommendation of the WHO, the average noise level in hospitals should not exceed 40 dB during both day and night time.12 However, generally, noise levels in ICUs are beyond what is recommended.13,14
Sleep deprivation is a relevant problem among patients hospitalized in ICUs with a high prevalence and significant repercussions. One way to manage this is by introducing evidence-based interventions to minimize noise. Implementing protocols for promoting sleep hygiene, which contitutes a set of behaviours recommended that people should do to promote good quality sleep,15 is necessary. This includes offering earplugs and eyeshades to patients, using relaxing music and noise, and reducing light in night shift as strategies recommended in the ICUs,8 with repercussions in reducing the incidence of delirium. However, there is low adherence to these measures, and they need to be adequately incorporated into routine team practices.14,16
Nonpharmacological interventions are often utilized to reduce environmental noise in ICUs and improve sleep quality. These include modifying environmental factors, training teams, raising awareness of the problem among professionals, and providing protective devices to patients.17 Among the proposed care practices, those involving changes in behaviour, such as educational programs for noise reduction among ICU professionals and using standardized alert indicators for staff and family members if their original indicators are beyond the acceptable rates for the location, and those related to the environment, such as the reduction of noise from doors and other sound-producing agents, are essential.18 These interventions should be considered in promoting sleep to favour a change in the team's behaviour to reduce noise and enable a shorter patient recovery time in the ICUs.13
ObjectivesThis evidence implementation project aimed to improve compliance with best practices recommended for noise control in the ICU of a private hospital.
Specific objectives (1) To provide the ICU nursing team with tools regarding sleep disorders, their repercussions, and sleep hygiene interventions for critically ill patients. (2) To identify barriers and facilitators in implementing practices recommended following the guidelines for reducing noise and promoting sleep hygiene in critically ill patients. (3) To assess the current practice of healthcare workers concerning best practice recommendations. MethodsThe current evidence-based implementation project was developed according to the evidence implementation model proposed by JBI. It constitutes applying the Practical Application of Clinical Evidence System (also known as JBI PACES) and Getting Research into Practice (GRiP) audit and feedback tools.19 The model advocates three steps: the baseline audit and identification of barriers to non-compliance, implementation of best recommended practices, and a follow-up audit after implementation.
LocationThe project was presented to a general ICU of a high-complexity private hospital in the city of Sao Paulo. It constitutes 11 beds distributed in individual rooms, each with access to a television, telephone, bedside computer, separate sink and toilet, and an extended visit model in which companions could stay for a continuous 24 h. The number of professionals in the nursing team during the study period was 51, 12 of whom were registered nurses, and the other were nursing technicians. Unfortunately, the unit did not have any guidelines or protocols for noise control.
Data collection procedure Phase 1: baseline audit and identification of barriers to noncomplianceBaseline audit and identification of barriers to noncompliance involved identifying the compliance of the ICU staff with the best practices of noise control implementation as per the JBI recommendations.20
The study team was established as follows:
(1) Team leader: drafting the protocol, conducting the baseline and postimplementation audits, implementing evidence, analysing data, and writing reports. (2) Team member 1: helping the team leader carry out all activities throughout the study. (3) Team member 2: helping the team leader carry out all the activities throughout the study. (4) Team member 3: unit coordinator responsible for helping to address the administrative and existing barriers of the study and ensuring all technical aspects of the study.The team leader presented the baseline audit results to the unit's leaders and the implementation project team. During this meeting were discussed the potential barriers to implementing best practices with their respective coping strategies.
The seven criteria audited during the entire month of April 2019 were inspired by the criteria proposed by the evidence summary Sleep Disturbances (ICUs): Noise Reduction and Behaviour Modification (Table 1),20 which includes noise level control in the ICU; documentation of the ICU patient's sleep pattern in medical records; training of the ICU nursing staff on sleep disorders and their implications for patients; training regarding intervention implementations to reduce noise in the ICUs; and training concerning staff behaviour change programs related to the sleep hygiene of ICU patients and training of strategies to moderate the tone of voice in the ICU.16,18,21-25
Table 1 - Audit criteria and measures of best practices in noise reduction. São Paulo, 2020 Audit criteria Sample Method of measuring compliance with best practices Criterion 1 - noise levels are based on the levels less than 40 dB recommended by the WHO or decreased by approximately 30% from the last measurement before the implementation of best practices 120 consecutive days before and 180 consecutive days after implementation of best practices Continuous measurement of the noise level, considering whether the noise level was as per the levels recommended by the WHO (40 dB) or decreased by 30% concerning the levels measured before the implementation of best practices Criterion 2 - the patient's sleep pattern in the ICU is adequately documented in their medical record 172 medical records after the implementation of best practices Evaluation of the record on the patient's self-evaluation of their sleep, considering whether this information was recorded in the medical record Criterion 3 - the nursing staff of the ICU receives training on sleep disorders and their implications for patients, interventions that reduce noise in ICUs, multifaceted interventions that reduce noise in ICUs, behavioural changes regarding the sleep hygiene of patients hospitalized in ICUs, and how to moderate the tone of voice in ICUs 45 nursing staff professionals Number of professionals from the unit's nursing team who underwent training on the topic in the last 6 months; professionals who answered that they attended the training were included Criterion 4 - the nursing staff of the ICU receives training on interventions that reduce noise in ICUs 45 nursing staff professionals Number of professionals from the unit's nursing team who underwent training on the topic in the last 6 months; professionals who attended the training were included Criterion 5 - the nursing staff of the ICU receives training on multifaceted interventions that reduce noise in ICUs 45 nursing staff professionals Number of professionals from the unit's nursing team who underwent training on the topic in the last 6 months; professionals who attended the training were included Criterion 6 - the nursing staff of the ICU receives training on behavioural changes regarding the sleep hygiene of patients admitted to ICUs 45 nursing staff professionals Number of professionals from the unit's nursing team who underwent training on the topic in the last 6 months; professionals who attended the training were included Criterion 7 - the nursing staff of the ICU receives training on how to moderate their tone of voice in ICUs 45 nursing staff professionals Number of professionals from the unit's nursing team who underwent training on the topic in the last 6 months; professionals who attended the training were includedCriterion 1 was measured between April and June, and the others were audited in May (before implementation) and August (after implementation) 2019. Data collection was carried out by the clinical leader of the project and two members of the research team. It was measured using the SoundEar noise sensor (SoundEar A/S, Søborg, Denmark) positioned at the unit's centre, close to the beds and the nursing station. The sensor continuously measured the noise level in dB, with values visible on the equipment screen and electronic recordings every hour in the software on the equipment. Criterion 2 was audited in the medical records (documentation of patients’ sleep patterns). Further, there was a field in the daily control of vital signs where the patient's self-assessment of their sleep pattern referring to the previous night, classified as good or bad, was recorded. Criteria 3, 4, 5, 6, and 7 were audited by asking professionals about their training regarding the topic.
On the basis of the analysis of data from the baseline audit, a discussion between the project team and key stakeholders was initiated on the strategies to be used in implementing the best practices and promoting adherence to the audited criteria, including the strategy to address barriers with the support of the GRiP tool (Table 2). The barriers identified were: the nursing team's insufficient knowledge about the main aspects of sleep deprivation and its impact on patients’ rehabilitation, the nursing team's resistance to adhering to recommended practices, financial difficulties in acquiring communication materials to raise the team's awareness about the importance of noise control, and difficulties in including a sleep diary in the electronic medical record.
Table 2 - Barriers and strategies according to the Getting Research into Practice tool, São Paulo, 2020 Expected barriers Strategies Resources Outcomes Lack of knowledge of nursing professionals on sleep disorders and their impact on patient rehabilitation and prevention strategies and noise reduction in the environment Training on evidence-based best practices in promoting sleep hygiene for ICU patients Team-based learning Multimedia resources Improvement of the nursing team's knowledge training of approximately 90% of the nursing team Resistance of the nursing team in adopting recommended practices Raising awareness of the team through an institutional communication campaign on the topic and trainingSupervision and feedback Information leafletsSupport from the institutional communication area and the ICU leadershipTeam-based learning strategy Nursing team development, and engagement sense and responsibility in noise control Financial difficulties in acquiring communication materials to raise the team's awareness about the importance of noise control Meetings with the ICU leadership and with the communication area to make the budget feasible Budget for the acquisition of materials and the dissemination and communication campaign Availability of content on the subject that is easily accessible to the nursing team Difficulties in including the sleep diary in the electronic medical record Meetings with the leadership of the ICU and with the technology area to update the electronic medical record Electronic medical record Availability of functionality for recording the patient's sleep diary in the electronic medical recordThe clinical leader selected teaching strategy as a resource to resolve the barriers identified by the team. The hospital where the project was developed offers support for developing improvements related to the care process, such as infrastructure related to communication, electronic medical records, and financial support.
Phase 2: implementation of best practices and strategies to improve practice (implementing research into practice)Professional training on best practices related to the topic was conducted using the team-based learning (TBL) strategy and included nursing staff from all shifts. TBL uses principles that maximize student preparation and participation and includes pre-classroom activities, classroom activities to promote active learning, teamwork skills, professional skill development, and elements to generate student interaction and engagement.26
Therefore, TBL consists of three sequential phases: phase 1, in which students perform pre-learning (before class) activities; phase 2, wherein students are subjected to a multiple-choice test of central concepts of the topic, answered individually, and later in teams of five to seven members; and phase 3, where the team applies the knowledge in their practice. Additionally, there is a discussion of the answers by the groups facilitated by the teacher.27
The training was conducted at different times. It included content related to sleep deprivation and non-pharmacological interventions for sleep hygiene to reduce noise in the ICU. Each training session lasted 120 min. Further, they were conducted by the clinical leader of the study, a specialist in the subject and the teaching methodology. The clinical leader also guided the activities and discussions during the group sessions to clarify doubts.
After the training, the professionals had access to an information leaflet on the importance of noise control, made available in the ICU and internal communication channels. Regarding the practice of documenting the sleep pattern of ICU patients, the strategy implemented was the inclusion of a sleep diary in the electronic medical record, with questions aimed at enabling patients to report the quality of their sleep once a day.
Noise monitoring was performed by placing a noise sensor in the area close to the nursing station, where the movement of people was intense. The noise sensor had softwares and noise data were extracted and analyzed.
Phase 3: follow-up auditNotably, preimplementation and postimplementation audits were identical. During the follow-up audit, the team responsible for the study monitored the staff's adherence to recommended practices, applying the same criteria as in the baseline audit, and 1 month after implementing the best practices. For example, the audited criterion 2 was related to sleep documentation in patients’ electronic medical records. Moreover, criteria 3, 4, 5, 6, and 7 were related to the attendance of the nursing staff in the training offered on the subject. Additionally, criterion 1 was evaluated 6 months after implementing the best practices.
Data analysisThe study data for the first and second stages were entered into Microsoft Excel 2010. Data regarding criteria 2, 3, 4, 5, 6, and 7, which corresponded to staff training and sleep quality documentation, were analysed using descriptive statistics and expressed in absolute and relative frequencies. Regarding the noise level (criterion 1), in addition to descriptive analysis, data were compared before and after implementation using the Mann-Whitney U test after verifying the type of distribution of this variable using the Shapiro-Wilk test. A significance level of 5% was used to compare noise-level data.
Ethical procedureThe project was approved by the Ethics and Research Committee of the hospital where it was conducted, under approval number 3325367.
ResultsThe values for noise generation in the analysed ICU remained stable, and the median after implementing the best practices was lower than before implementation (Fig. 1). That is, from April to July 2019 (the baseline audit period) and from August 2019 to January 2020 (the period after the implementation of the best practices), the noise levels reached a median of 64.15 dB (59.2–66.4) and 63.9 dB (59.5–66.4), respectively. Although there was a decrease in the noise level, it was not above 30% of the values measured in the first step, as recommended. Furthermore, the noise levels during the daytime were higher than those at night (Fig. 1), indicating significant professional activities during the day.
 Figure 1:
Figure 1: Median values regarding noise level in dB before and after implementing best practices. São Paulo, 2019.
Although no statistically significant differences were detected in general noise levels between the periods before and after the implementation of the best practices (P = 0.853), the noise level at the five evaluated times showed a significant difference (less than 0.05) in the median values when comparing the steps before and after the implementation of the best practices. Among these, 5:30 a.m. had a higher median noise value in the period after implementation.
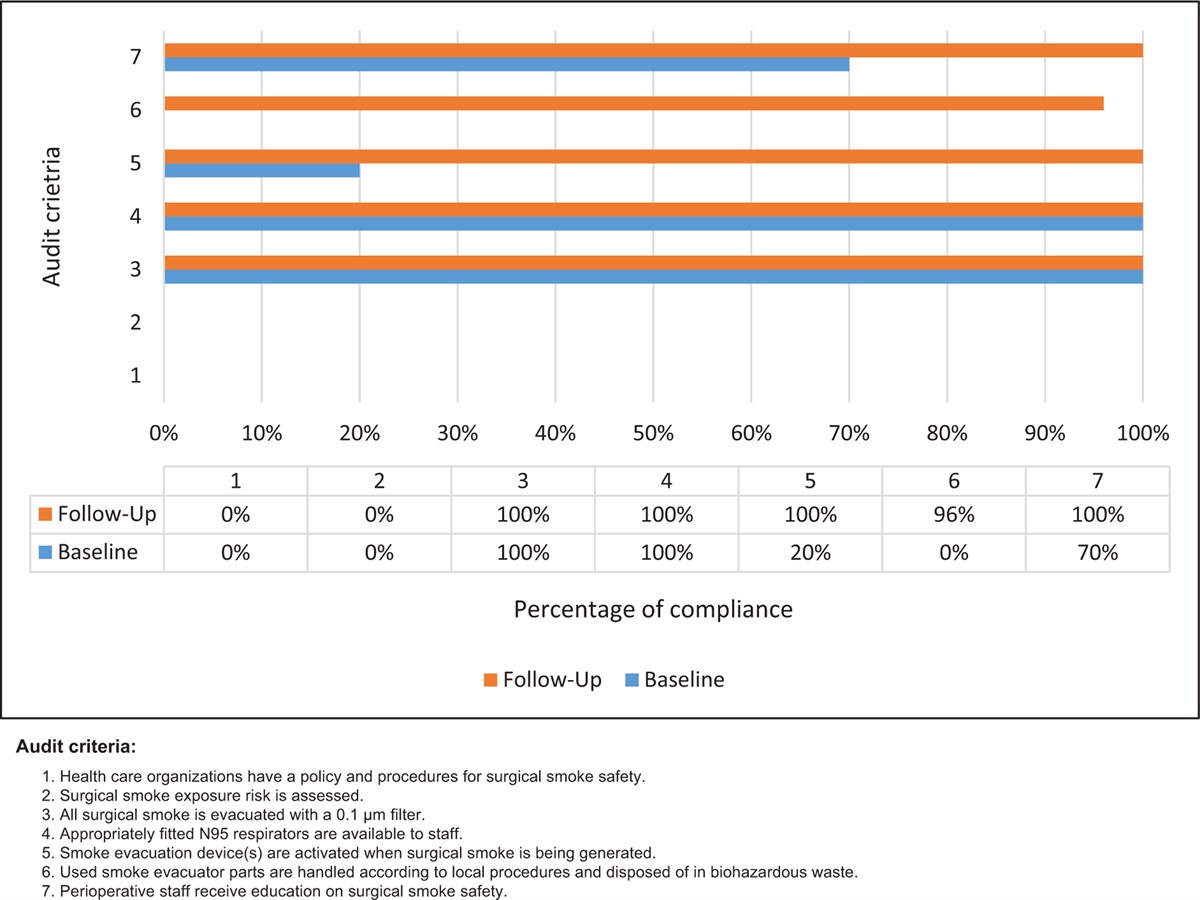
In Fig. 2, the baseline audit results indicate that none of the seven criteria evaluated, such as the best practices for promoting sleep, were implemented in the analysed ICU. However, six of the criteria considered had an adherence rate of 78–88% post-implementation.
 Figure 2:
Figure 2: Compliance rate of audit criteria before and after implementing good practices. São Paulo, 2019. β1 = noise levels in the intensive care unit are as per the recommendations of the WHO or have decreased by about 30% from the last measurement before implementing the best practices; ∗2 = patients’ sleep pattern is documented;+3 = the nursing staff of the ICU receives training on the importance of sleep for patients, including the consequences of sleep deprivation; ″4 = the nursing staff of the ICU receives guidance on noise reduction strategies; ?5 = the nursing staff of the ICU receives guidance on implementing a multifaceted approach for noise reduction; ∼6 = the nursing staff of the ICU receives guidance on behaviour modification to reduce noise; °7 = the team of professionals from the ICU receives guidance on how the team's tone of voice affects patients’ sleep patterns.
Regarding criterion 2, which aimed to analyze the adequate documentation of patients’ sleep in the medical records of hospitalized patients, the baseline audit compliance was 0% and increased to 78% after implementing the interventions.
Criteria 3, 4, 5, 6, and 7 referred to the training of the 45 professionals of the nursing team (88%), which included nurses and nursing technicians working in the evaluated ICU who participated in the activity conducted to equip the professionals.
DiscussionThe evidence-based implementation project showed satisfactory results regarding health professionals’ adherence in the ICU to the best practices recommended for promoting sleep hygiene and reducing noise. Most of the pre-established audit criteria, except noise level, obtained satisfactory compliance rates. The training was adequate, but the actual outcome of reducing the dB level was not. Therefore, increasing staff awareness of the factors contributing to noise did not have the intended effect.
Unfortunately, meeting the 40 dB parameter recommended by the WHO was difficult, reflecting the results of other related studies.28,29 Thus, controlling noise as a sleep deprivation factor is the most challenging, hindering the realization of comfortable environments for patients and professionals. In a previous study, wherein the median noise level in the ICU was similar to that in the present study, noise was the only factor that significantly influenced patients’ sleep quality.30
Studies that showed significant noise reduction implemented some innovative strategies such as ‘Quiet Time’,31 referring to when changes in staff behaviour aimed to produce less noise. The literature shows that noise reduction can be achieved, as much of the noise source is avoidable30 and comes from infusion equipment, monitors with maladjusted vital parameter alarms, and conversations among health professionals.32,33 Thus, training and awareness of nursing staff on the importance of the topic could have significantly influenced the decrease in the noise level.
In the present study, after training the nursing staff, there was a reduction in noise levels at four time points: 8: 30 a.m., 2: 30 p.m., 5: 30 p.m., and 6: 30 p.m.; these are traditional moments of intense movements and activities within hospitals. However, at other times, such as 5: 30 a.m., there was an increase in noise levels, which could be attributed to professional activities related to preparation for night shift changes and increased demand for care regarding drug administration time and control of vital signs. This fact corroborates the importance of improving professionals’ behaviours and reviewing the unit's care routines during this time. The increase in noise levels after 4:30 a.m. was documented in several ICUs, possibly because of the influence of activities, such as shift changes, visits, and patient feeding.34
The training of professionals from the nursing team in the analysed ICU emphasized the causes of noise and the interventions to control the problem. Notably, health professionals often underestimate the impact of these aspects on patients’ sleep quality. This is relevant, especially considering the importance of sleep as a vital element for critically ill patients’ recovery.29 Further, it is pertinent as sleep deprivation remains undervalued in ICU environments. Thus, a joint effort must be made among professionals working in this area to promote noise reduction as a practice to be included in care protocols.
Moreover, patients consider the tone of voice a determining factor in noise production, which contributes to sleep deprivation.10 Staff guidance on their tone of voice was emphasized during training and is among the best practices implemented and included in sleep hygiene protocols.31,35 This practice is significantly related to behavioural change and requires the reflection and incorporation of new attitudes by professionals.
These measures have contributed to greater adherence to best practices, except noise level, which is the biggest challenge. Owing to the ICU's complexity and work dynamics in these environments, noise is the most challenging factor to control. Therefore, healthcare professionals’ understanding of these environments regarding the need for changes in practices and behaviours is essential for modifying approaches concerning sleep hygiene and incorporating guidelines and protocols.
It is essential to highlight the aspects of documenting sleep patterns among patients in this study, which went from non-existent to 78% compliance after implementing the best practices. The documentation made by nurses was standardized and based on questions directed towards the patient sleep self-assessment regarding their previous night during the daily physical examination. Subjective assessment is considered the gold standard for measuring sleep quality. Furthermore, documentation of sleep in ICU patients should be a part of routine care and include the evaluation of patients’ needs to deal with sleep disorders, interventions, and their effects, along with patients’ perspectives, which contribute to the premise of person-centred care.36,37
A cluster of measures for noise control that involved staff training and control of environmental barriers effectively reduced the noise level,38 highlighting the continuous guidance of professional teams and family members on the relevance of noise in sleep deprivation and positively influencing the decrease in noise levels. However, the control of environmental aspects, such as monitors, alarms, doors, and garbage repositories, is an important aspect that requires joint action between professionals. Moreover, it may explain why merely training and guiding the team on the problem did not reduce the noise level in some situations.39
Best practice implementation projects are essential when adopting evidence to improve healthcare. They can also contribute to the significant reflection on and awareness of the problems encountered in our professional experience. These programs are supported by evidence-based, robust recommendation studies indicating that sleep hygiene among patients admitted to ICUs is significantly beneficial for patient management. However, it is necessary to implement and maintain the sustainability of these practices, which pose challenges for health institutions.
ConclusionAdherence to best practices concerning staff training and documentation of patients’ sleep diaries in the analysed ICU was satisfactory, with more than 70% compliance rate in six of the seven audited criteria. However, only the ‘noise level’ criterion did not reach the threshold recommended by the WHO, a difficulty also reflected in other related studies. Therefore, it is necessary to increase the motivation to engage professionals in elaborating guidelines on the subject and conducting studies on effective strategies to reduce noise in ICUs, consequently reducing sleep deprivation in patients hospitalized in ICUs. Additionally, actions related to the sustainability of practices are a significant challenge. Nonetheless, they should be planned using clinical auditing and the analysis of indicators.
AcknowledgementsThe authors thank the Instituto de Ensino e Pesquisa Sirio Libanes and The Brazilian Centre for Evidence-informed Healthcare: a JBI Centre of Excellence (JBI Brazil).
Conflicts of interestThere are no conflicts of interest.
References 1. Tucker S, McNett M, Mazurek Melnyk B, et al. Implementation science: application of evidence-based practice models to improve healthcare quality. Worldviews Evid Based Nurs 2021; 18:76–84. 2. Eccles MP, Mittman BS. Welcome to implementation science. Implement Sci 2006; 1:1. 3. Delaney L, Litton E, Van Haren F. The effectiveness of noise interventions in the ICU. Curr Opin Anaesthesiol 2019; 32:144–149. 4. Macfarlane M, Rajapakse S, Loughran S. What prevents patients sleeping on an acute medical ward? An actigraphy and qualitative sleep study. Sleep Health 2019; 5:666–669. 5. Carey MG, Qualls BW, Burgoyne C. Patients’ perception of stressful events in the intensive care unit after cardiac surgery. Am J Crit Care 2019; 28:149–151. 6. Bani Younis M, Hayajneh FA. Quality of sleep among intensive care unit patients: a literature review. Crit Care Nurs Q 2018; 41:170–177. 7. Alexopoulou C, Bolaki M, Akoumianaki E, et al. Sleep quality in survivors of critical illness. Sleep Breath 2019; 23:463–471. 8. Devlin JW, Skrobik Y, Gelinas C, et al. Clinical practice guidelines for the prevention and management of pain, agitation/sedation, delirium, immobility, and sleep disruption in adult patients in the ICU. Crit Care Med 2018; 46:e825–e873. 9. Shah P, Krishnan V. Hospitalization and sleep. Am J Respir Crit Care Med 2019; 199:p19–20. 10. Simons KS, Verweij E, Lemmens PMC, et al. Noise in the intensive care unit and its influence on sleep quality: a multicenter observational study in Dutch intensive care units. Crit Care 2018; 22:250. 11. Carrera-Hernández L, Aizpitarte-Pejenaute E, Zugazagoitia-Ciarrusta N, Goni-Viguria R. Patients’ perceptions of sleep in a critical care unit. Enferm Intensiva (Engl Ed) 2018; 29:53–63. 12. Dorsch JJ, Martin JL, Malhotra A, Owens RL, Kamdar BB. Sleep in the intensive care unit: strategies for improvement. Semin Respir Crit Care Med 2019; 40:614–628. 13. Jobanputra AM, Scharf MT, Androulakis IP, Sunderram J. Circadian disruption in critical illness. Front Neurol 2020; 11:820. 14. Grimm J. Sleep deprivation in the intensive care patient. Crit Care Nurse 2020; 40:e16–24. 15. Ellis JG, Allen SF. Grandner MA. Sleep hygiene and the prevention of chronic insomnia. Sleep and Health.. Cambridge: Academic Press; 2019. 137–145. 16. Plummer NR, Herbert A, Blundell JE, Howarth R, Baldwin J, Laha S. SoundEar noise warning devices cause a sustained reduction in ambient noise in adult critical care. J Intensive Care Soc 2019; 20:106–110. 17. Zamani K, Asgharnia HA, Yazdani J, Taraghi Z. The effect of staff training on the amount of sound pollution in the intensive care unit. J Nurs Midwifery Sci 2018; 5:130–133. 18. Konkani A, Oakley B. Noise in hospital intensive care units -a critical review of a critical topic. J Crit Care 2012; 27:522.e1-9. 19. Pearson A, Wiechula R, Court A, Lockwood C. The JBI model of evidence-based healthcare. Int J Evid Based Healthc 2005; 3:207–215. 20. Whitehorn, A. What is the best available evidence regarding noise reduction and behaviour modification programs or interventions in intensive care units (ICUs)? Evidence summary. Joanna Briggs Institute. 2019. Available at: https://connect.jbiconnectplus.org/ViewDocument.aspx?0=20856 [Accessed 23 January 2019]. 21. Tembo AC, Parker V. Factors that impact on sleep in intensive care patients. Intensive Crit Care Nurs 2009; 25:314–322. 22. Boyko Y, Jennum P, Nikolic M, Holst R, Oerding H, Toft P. Sleep in intensive care unit: the role of environment. J Crit Care 2017; 37:99–105. 23. Dube JA, Barth MM, Cmiel CA, et al. Environmental noise sources and interventions to minimize them: a tale of 2 hospitals. J Nurs Care Qual 2008; 23:216–224. 24. Monsen MG, Edell-Gustafsson UM. Noise and sleep disturbance factors before and after implementation of a behavioural modification programme. Intensive Crit Care Nurs 2005; 21:208–219. 25. Taylor-Ford R, Catlin A, LaPlante M, Weinke C. Effect of a noise reduction program on a medical-surgical unit. Clin Nurs Res 2008; 17:74–88. 26. Sookhoo D, Thurston C. Effectiveness and experiences of team-based learning in nurse education programs: a mixed methods systematic review protocol. JBI Database System Rev Implement Rep 2018; 16:1912–1921. 27. Parmelee D, Michaelsen LK, Cook S, Hudes PD. Team-based learning: a practical guide: AMEE guide no. 65. Med Teach 2012; 34:e275–e287. 28. Guisasola-Rabes M, Sola-Enriquez B, Velez-Pereira AM, de Nadal M. Effectiveness of a visual noise warning system on noise levels in a surgical ICU: a quality improvement programme. Eur J Anaesthesiol 2019; 36:857–862. 29. Bani Younis M, Hayajneh F, Batiha AM. Measurement and nonpharmacologic management of sleep disturbance in the intensive care units: a literature review. Crit Care Nurs Q 2019; 42:75–80. 30. Suparti S, Suroso J. The correlation between humidity, temperature, and noise with sleep quality at Intensive Care Unit (ICU). Journal INJEC 2020; 5:60–68. 31. Goeren D, John S, Meskill K, Iacono L, Wahl S, Scanlon K. Quiet time: a noise reduction initiative in a neurosurgical intensive care unit. Crit Care Nurse 2018; 38:38–44. 32. Kamdar BB, Simons KS, Spronk PE. Can ICUs create more sleep by creating less noise? Intensive Care Med 2020; 46:498–500. 33. Delaney LJ, Currie MJ, Huang HC, Lopez V, Van Haren F. They can rest at home: an observational study of patients’ quality of sleep in an Australian hospital. BMC Health Serv Res 2018; 18:524. 34. Garside J, Stephenson J, Curtis H, Morrell M, Dearnley C, Astin F. Are noise reduction interventions effective in adult ward settings? A systematic review and meta analysis. Appl Nurs Res 2018; 44:6–17. 35. Dennis CM, Lee R, Woodard EK, Szalaj JJ, Walker CA. Benefits of quiet time for neuro-intensive care patients. J Neurosci Nurs 2010; 42:217–224. 36. Alsulami G, Rice AM, Kidd L. Prospective repeated assessment of self-reported sleep quality and sleep disruptive factors in the intensive care unit: acceptability of daily assessment of sleep quality. BMJ Open 2019; 9:e029957. 37. Zengin N, Ören B, Üstündag H. The relationship between stressors and intensive care unit experiences. Nurs Crit Care 2020; 25:109–116. 38. Ahamed MF, Campbell D, Horan S, Rosen O. Noise reduction in the neonatal intensive care unit: a quality improvement initiative. Am J Med Qual 2018; 33:177–184. 39. Crawford KJ, Barnes LA, Peters TM, Falk J, Gehlbach BK. Identifying determinants of noise in a medical intensive care unit. J Occup Environ Hyg 2018; 15:810–817.
留言 (0)