
記住我
Appeals to the dignity of people with dementia are widespread in clinical practice guidelines and policy recommendations.1 2 In the current academic literature, scholars similarly invoke the concept of dignity in examining various ethical issues in dementia care.3–6 References to dignity in the context of dementia care are part of a broader trend in bioethical literature in which the concept of dignity has gained considerable traction.
One influential account of dignity in the wider philosophical and bioethical literature that has received relatively less attention and has remained underexplored in the context of dementia care is that of Martha Nussbaum. This paper critically examines Nussbaum’s account of dignity and aims to determine what moral guidance this account can offer for the provision of care to people with dementia.
The paper proceeds as follows. The first section identifies four possible objections to the normative relevance of appeals to dignity in dementia care. These objections are (1) redundancy of the dignity talk, (2) exclusionary implications, (3) reliance on (suspect forms of) speciesism and (4) unclear practical implications. The second section discusses and examines Nussbaum’s account of dignity vis-à-vis the four objections. I argue that Nussbaum’s account, in its original version, effectively evades the first and the third objections but struggles to overcome the objections of exclusionary and unclear practical implications. In the third section, I argue for a modified version of Nussbaum’s account of dignity. The modified version of Nussbaum’s account is predicated on a novel dementia-specific model of flourishing, which draws on Kitwood and Bredin’s7 empirically driven list of indicators of well-being for people with dementia. I conclude briefly afterwards.
Dignity and dementia care: four possible objectionsRedundancy of the dignity talkThe first possible objection concerns what Macklin and Pinker describe as the redundancy of appeals to human dignity. Pinker’s8 criticism focuses on the alleged politicisation of dignity by those opposed to particular advances in biomedical research. Pinker, p318 asserts that dignity has been used by some ‘to condemn anything that gives someone the creeps’ and claims that that talk of dignity is redundant as ‘ultimately it’s just another application of the principle of autonomy’.
Similarly, Macklin9 lambasts invoking the considerations of dignity in medical ethics. She argues that appeals to human dignity are either slogans or ambiguous reiterations of more precise ethical considerations of ‘respect for persons or for their autonomy’ (Macklin, p1419).9 Alternatively stated, if respect for dignity is simply a restatement of respect for persons and/or respect for autonomy, then the talk of dignity is redundant.
This objection is not strong.
First, consider respect for persons. Macklin seems to assume that we can subsume appeals to respect for human dignity under respect for persons. She also seems to assume that respect for persons is relatively unambiguous. One can challenge both of these assumptions.
As Foster10 notes, subsuming appeals to respect for human dignity under respect for persons would not get the justificatory story right. Respect for human dignity often is thought to function as a justification for respect for persons. The invocation of respect of persons ‘is an acknowledgment … of a deeper principle at work’ (Foster, p61).10 As long as the underlying principle behind invocations of respect for persons is thought to be respect for human dignity, Macklin’s strategy to subsume extant appeals to respect for human dignity under respect for persons would fail1.
There are also grounds for scepticism about Macklin’s suggestion that respect for persons is a relatively unambiguous moral principle. As Beauchamp and Childress (p68)11 point out, there are definitional issues around what entities count as persons. There are considerable disagreements in the current bioethical and philosophical literature on whether (and/or to what extent) entities such as fetuses, newborns or non-human animals can be considered persons.12 ,2 But even if we settle the definitional issues around what entities can be considered persons, there is a further philosophical question that needs to be answered. This further question is how we (dis)respect entities considered as persons qua persons. This question can be answered differently given that, as Darwall, p3713 notes, there are ‘different ways in which persons may be the object of respect’. As such, and given these definitional and conceptual issues, one could argue that it is debatable whether respect for persons functions as an unambiguous moral principle.
But what about respect for autonomy (which some might think is more unambiguous than respect for persons)? Can we, as Macklin and Pinker suggest, equate respect for dignity with respect for autonomy? In the following, I argue that there are reasons to suspect that respect for dignity cannot be equated with respect for autonomy.
On the one hand, consider people with very advanced dementia. While it seems counterintuitive to think that acts taken by people at the very late stages of dementia can be autonomous, the situation is different regarding dignity. It appears to be consistent with the intuition that many of us share that, for instance, abusive, degrading or insulting forms of caregiving compromise the dignity of people with very advanced dementia.
On the other hand, there might be cases in which one can reasonably consider a specific decision as autonomous yet be willing to over-ride it by dignity considerations. An illustrative example is the banning of a local dwarf-throwing competition by the Mayor of Morsang-sur-Orge (a commune in France) in 1991. The Mayor banned the contest claiming it violates ‘respect for the dignity of the human person’ (Rosen, p64).14 Manuel Wackenheim, a dwarf, who was willing to take part in the competition appealed the ban. In February 1992, the ban was revoked by the Administrative Court in Versailles, but later in October 1995 was reissued by the Conseil d’État. In this case, the fact that Wackenheim was willing (or consented) to take part in the dwarf-throwing competition was deemed inconsequential. The ban by the Mayor and its adjudication by the Conseil d’État were influenced by the idea that respecting human dignity sets ‘limits to autonomy’3 (Beyleveld, p27).15
My intention in discussing these cases is simply to strike a cautionary note. I am aware that they do not generate strong arguments to refute the claim that respect for dignity and respect for autonomy do the same moral work. But note that the case for equating autonomy with dignity made by Macklin and Pinker does not seem strong either.
I think, nonetheless, that the objection should be taken seriously (even if the version of the objection made by Macklin and Pinker is not strong). To be conceptually sound, any account of dignity for people with dementia needs to explain the relation, if any, between respect for autonomy and respect for dignity.
Exclusionary implicationsThe second objection concerns the ground of human dignity. Suppose we base human dignity on the cognitive competence to exercise rational agency. In that case, a concern might arise that this way of grounding dignity may exclude people with cognitive disabilities, including people with dementia. For instance, the Kantian account attributes dignity to beings who have a rational nature and are autonomous self-legislating moral agents.17 As Kittay18 notes, accounts of dignity of the Kantian sort can be exclusionary to people with dementia.
This objection seems to be based on the presumption that it is desirable (or even necessary) to attribute dignity to people with dementia and wrong to exclude them from the circle of human beings with dignity. I tend to agree with this, given the potential for dignity to capture morally relevant features about the care of people with dementia and the central place of dignity talk in the literature on dementia care. If we want to include people with dementia in the circle of human beings with dignity, the cognitive abilities-based accounts of dignity such as the Kantian-inspired accounts do not provide relevant grounds.
Reliance on (suspect forms of) speciesismThe third objection also concerns the ground of human dignity but targets different conceptions. Human dignity is often conceived as an inherent property of all human beings that justifies human rights entitlements and ultimately serves as the foundation for social and political equality everywhere in the world.19
At first blush, this seems very inclusionary to people with dementia. But one might ask: what gives all human beings dignity?
One answer is that the ground of human dignity is in the membership of the species Homo sapiens. This answer is unsatisfactory because of its appeal to what Singer20 calls speciesism. The key idea here is that the mere membership of a particular species (ie, Homo sapiens) cannot be solid grounds for attributing dignity exclusively to all human beings. That is to say, it seems to be somewhat arbitrary to attribute dignity to all members of a specific species and refuse to give it to other species (eg, Pan troglodytes or chimpanzees)4.20
This objection is serious. It should, nonetheless, be noted that this objection works as far as we solely (and presumably arbitrarily) attribute dignity to members of a specific species. To be able to include people with dementia in the circle of human beings with dignity in a way that is not arbitrary, we need an account of dignity that does not ground the attribution of dignity solely based on the membership in our species (ie, Homo sapiens).
Unclear practical implicationsLastly, the fourth objection is concerned with the usefulness of appeals to dignity in dementia care. Part of what motivates the criticism made by Macklin and Pinker is the concern that lack of clarity about the meaning of dignity renders its use in biomedical ethics impracticable. After reviewing different philosophical accounts of dignity, Schulman, p1322 also voices a similar concern about the lack of ‘clear and unambiguous guidance in bioethical controversies’.
This is a legitimate concern. This concern provides a further desideratum for a robust account of dignity for people with dementia: it must have reasonably unambiguous practical implications and provide sufficiently clear guidance on care for these individuals.
Nussbaum’s account of human dignityI now provide a concise overview of Nussbaum’s account of human dignity.
Nussbaum offers her notion of human dignity as part of her version of the capabilities approach, a political theory arguing for the fundamental political entitlements of all citizens to have a threshold amount of opportunity for exercising and developing essential human capabilities5.23 24
Nussbaum, p36226 charges accounts of dignity such as that held by Kant with ‘excessive rationalism’. Nussbaum instead sets out to develop a novel account of human dignity, which she characterises as a hybrid Aristotelian/Marxian account. Her starting points are two interrelated claims.
First, she holds that we should construe ‘the dignity of the human being as squarely a part of the world of nature’ and we should not ‘posit a sharp split between rationality and other human capacities’ (Nussbaum, p362).26 Nussbaum26 argues that the foundation of human dignity lies in ‘a varied set of capacities that are all elements in the life of a type of animal being’. Nussbaum, p36323 then adds that the capacities at issue here are certain evaluatively chosen and species-relative capacities in the sense that the opportunity to exercise those capacities is an indicator of the flourishing of human beings qua members of species Homo sapiens.
Nussbaum, however, does not hold that only human beings have dignity. On Nussbaum’s, p36526 account, the status of dignity extends to all animal beings, including human animals, that present a certain set of capacities to ‘grow up and lead flourishing lives’. Not all animals, Nussbaum notes, present such capacities. One key feature, according to Nussbaum, that grounds the dignity of animal beings is their sentience, that is to say, their capacity for feeling pleasure and pain.
Human dignity, on Nussbaum’s account, is different from the types of dignity in other species because of a certain set of normatively chosen capabilities, the exercise of which is an indicator of the flourishing of members of our species. Nussbaum lists 10 essential capabilities that are markers of a flourishing life for members of our species (table 1).
Table 1List of the 10 basic capabilities of human beings as suggested by Nussbaum26
Nussbaum’s account of dignity does not run into the problem of speciesism as her account transcends the boundaries of species membership. In Nussbaum’s view, there is not only one form of dignity that human beings share with many other non-human animals. Instead, Nussbaum, p36526 holds that there are ‘many distinct varieties of dignity, some human and some belonging to other species’.
Further, Nussbaum takes issue with the inviolability presumption about human dignity. According to Nussbaum, the capabilities in their untrained form are basic. Once trained, they become internal capabilities. To fully exercise these internal capabilities, in Nussbaum’s view, one requires sufficient material resources and needs to be in favourable material, social and political circumstances. Under such circumstances, the internal capabilities become what Nussbaum calls combined capabilities. Absent suitable circumstances, Nussbaum holds, someone with even fully developed internal capabilities cannot have combined capabilities. For example, an educated woman in a repressive environment might have a highly developed internal capability of practical reasoning, yet she may not have the associated combined capability due to a lack of opportunities to shape her life the way she aims to.26
Having made the above distinctions, Nussbaum argues that all human beings have inalienable dignity in virtue of having the basic capabilities (ie, the potential) to flourish. Nussbaum, however, does not think of human dignity as inviolable. She holds that violations of human dignity occur when there are setbacks in converting basic capabilities to combined capabilities. Alternatively stated, according to Nussbaum, setting back the fulfilment and flourishing of the said capabilities of human beings leads to violations (but not the abrogation) of human dignity6.26
The above was a concise summary of the main features of Nussbaum’s account of (human) dignity. I noted earlier that her account evades the objection of reliance on speciesism. In what follows, I investigate whether Nussbaum’s account of dignity overcomes the three other problems discussed in the first section.
Although Nussbaum does not explicitly address the issue of equating dignity with autonomy, she does not seem to consider dignity considerations to be the same as autonomy concerns. While in the list of 10 capabilities, as Jecker29 notes, we have elements such as control over one’s environment or bodily integrity that fall within the purview of autonomy considerations, Nussbaum’s conception of human dignity appears more expansive than that. For example, her list of 10 essential capabilities includes items such as bodily health or life. These capabilities can be labelled as welfare considerations. As such, Nussbaum’s notion of human dignity seems to be inclusive of but not limited to autonomy considerations. For this reason, Nussbaum’s account of dignity does not seem to run into the problem of equating dignity with autonomy (ie, redundancy of the dignity talk).
What about the problems of exclusionary and unclear practical implications for people with dementia?
Here, it seems to me that some of the essential capabilities proposed by Nussbaum might not be inclusive of people with dementia and may result in practical difficulties. By way of example, consider political participation or practical reasoning. Exercising these capabilities, along with other essential capabilities, in Nussbaum’s view, is an indicator of flourishing life. People with severe cognitive disabilities, including people with advanced dementia, however, might not be able to exercise (or even have access to) the capabilities of political participation or practical reasoning to any significant degree. It should be noted that Nussbaum, p3625 explicitly argues that respect for human dignity requires ensuring ‘an ample (specified) threshold of capability, in all ten of those areas’. It seems to me then that Nussbaum’s account struggles to overcome the problem of exclusionary implications and consequently lack clear practical applicability for people with (advanced) dementia.
These issues with Nussbaum’s account have been identified and discussed in detail by Kittay, p110.18 She holds that the issues arise from the way in which Nussbaum appeals to and utilises a particular ‘norm of human functioning’. According to Kittay,18 by relying on a single, strict model of human flourishing, Nussbaum’s account risks excluding some human beings.
To be fair, Nussbaum seems to be aware of these problems with her account of dignity (and her respective model of the flourishing of human beings). Nussbaum23 30 acknowledges the challenges that people with cognitive disabilities present to her account of human dignity. But she dismisses the criticism that her account of dignity excludes people with cognitive disabilities. She argues that guardianship can be a viable practical strategy to facilitate the ‘access to all the central capabilities’ in people with cognitive disabilities (Nussbaum, p199).23
Nussbaum’s reasoning, however, is vulnerable to a serious objection. Guardianship may facilitate access to the basic capabilities in people with milder forms of cognitive disability (eg, early-stage Alzheimer’s disease). But, as Formosa and Mackenzie, p88127 note, it is implausible to suggest that guardianship can be of practical use for people with severe cognitive disabilities for whom (many of the 10) capabilities are ‘constitutively’ beyond their reach.
Considering such difficulties, Nussbaum’s account of dignity for people with dementia, at least in its original version, seems to struggle to overcome the problems of exclusionary and unclear practical implications. In the next section, however, I argue that a modified version of Nussbaum’s account is more likely to get around these problems.
A modified version of Nussbaum’s account of human dignity for people with dementiaI will take two steps to modify Nussbaum’s account of dignity.
First, I suggest that Nussbaum’s original list of capabilities can be considered a broad list that needs some further specification and contextualisation in the context of dementia care. That is, instead of relying on Nussbaum’s original list of capabilities for people with dementia, we can have a more specified and tailored set of capabilities that are more accessible to these individuals.
Second, Nussbaum’s model of flourishing for people with dementia should be modified to account for the natural progression of the disease. As previous empirical research has shown, with the progression of the underlying neurodegenerative condition, the capabilities of people with dementia diminish over time.31 As such, we need to make a distinction between dementia-related progressive deprivation of capabilities and external setbacks to the exercise of extant capabilities in the context of dementia care.
In keeping with Nussbaum, the latter refers to those instances when there is a lack of sufficient material resources for people with dementia to convert their basic capabilities to combined capabilities. The former, however, refers to the negative impact of the progression of dementia on the access to and exercise of an individual’s capabilities. As such, any assessment of respecting or violating dignity in the context of dementia care needs to attend to the two following facts: (1) people with dementia have a varying degree of access to basic capabilities, and (2) the access that an individual with dementia has to their basic capabilities progressively declines in the course of dementia.
As such, we need a dementia-specific model of flourishing that has more practical relevance to people with dementia than Nussbaum’s original model, which is more suited to adult, neurotypical human beings with relatively more stable access to their basic capabilities.
I think what Kitwood and Bredin7 propose as a dementia-specific list of indicators of well-being can provide some ground for developing a more specific model of flourishing for people with dementia (box 1).
Box 1 Indicators of well-being of people with dementia as proposed by Kitwood and Bredin7Expression of desires or showing will.
The ability to have emotional experiences or expressions.
Initiating social interaction.
Affectional warmth.
Social sensitivity.
Self-respect.
Accepting other people with dementia.
Humour.
Creativity and self-expression.
Showing evident pleasure.
Helpfulness.
Relaxation.
Kitwood and Bredin’s list of indicators of well-being is empirically driven and, for the most part, the indicators do not require the exercise of complex cognitive abilities. They propose their list of indicators of well-being as part of a personhood-centred approach to dementia care. This approach deploys a conferral account of personhood, according to which personhood is a moral status conferred on a human being by others ‘in the context of relationship and social being’ (Kitwood, p6)32.
As I 33 elsewhere argued, however, Kitwood’s appeal to personhood as a normative notion to conceptually ground the above list of indicators of well-being is problematic7. For Kitwood, there is only one necessary and sufficient condition for the status of personhood: there need to be other human beings that are willing to confer the status of personhood on an individual. As such, the personhood of people with dementia, as construed by Kitwood, is socially contingent and precarious.33 Kitwood’s account implies that an individual will lose (or not acquire) personhood status, if others are reluctant to consider them as a person. This means that, according to Kitwood's account, 33 ‘there is nothing about individuals with dementia that grounds the attribution of personhood except for their relationship with others’.
Instead, my suggestion is to consider Kitwood and Bredin’s list of indicators of well-being as a specified and contextualised version of Nussbaum’s list of basic capabilities for people with dementia (figure 1).
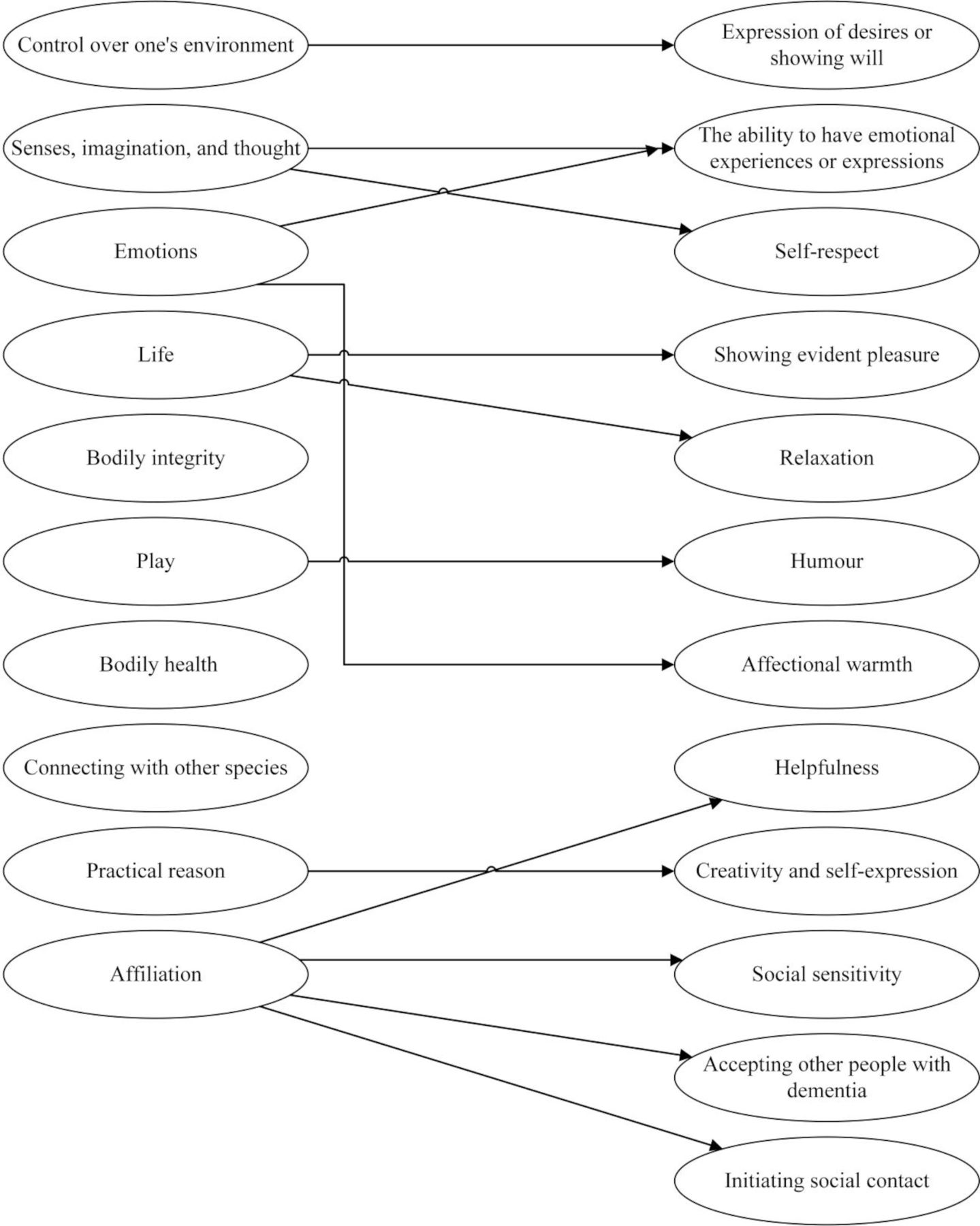 Figure 1
Figure 1 Nussbaum’s list of basic capabilities (on the left) vis-à-vis Kitwood and Bredin’s list of indicators of well-being (on the right).
There are two points that need further clarification here.
First, there are three capabilities on Nussbaum’s list that do not seem to map directly on items on Kitwood and Bredin’s list. These include bodily health, bodily integrity and connecting with other species. It seems plausible to me that Kitwood and Bredin considered protecting bodily health and bodily integrity as given or as a minimum of care in their account. As such, they did not include any item on their list that reflects the protection of bodily health and bodily integrity. Similarly, Kitwood and Bredin did not include any item on their list that parallels what Nussbaum frames as the capability to connect with other species. But this might be because at the time Kitwood and Bredin were compiling the list, there was scant evidence on the benefits of animal companionship for people with dementia. Currently, there is an extensive body of research documenting that people with dementia at various stages of the disease retain the capacity to connect with and benefit from animal companions.34 35
My suggestion is that we supplement Kitwood and Bredin’s list with the above three items (table 2). One advantage of this list is that it has fairly clear implications for what forms of care respect or violate the dignity of people with dementia. Table 2 lists some of the concrete external setbacks and facilitators to the flourishing of people with dementia in relation to the proposed dementia-specific list of basic capabilities.
Table 2Dementia-specific basic capabilities
I should also emphasise that the aim of respecting dignity in dementia care cannot be achievement of an equal level of exercising all the capabilities. Instead, a more practical and conceptually sound aim is to provide external opportunities and material resources for people with dementia to exercise to the greatest extent possible and as many as possible of their extant capabilities. Conversely, assessing the violations of the dignity of people with dementia should focus on external constraints that negatively impact people with dementia to access and exercise their extant capabilities given and despite dementia-related progressive deprivation of capabilities.
Before concluding my discussion in this paper, it is apposite to address two possible objections.
The first objection is that relying on a dementia-specific model of flourishing for people with dementia may imply that people with dementia have a different type of dignity than other human beings. But this objection would be based on a misinterpretation of what I argued above. My proposed dementia-specific model of flourishing (on which dignity claims are based and sustained) is not a substitute for Nussbaum’s standard model of flourishing. Instead, my proposed dementia-specific model of flourishing is a specified and contextualised version of Nussbaum’s original model. On my account, there is no conceptual division between the (status) dignity of people with dementia and the (status) dignity of other human beings.8
There may be, nonetheless, a further objection. The modified version of Nussbaum’s account that I defended above rests on the following core idea. The idea is that people with dementia have dignity in virtue of having some of the basic capabilities listed in table 2. One now may contend that this definition excludes some people with very advanced dementia who do not have any extant capabilities of the sort described above.
My response to the objection is that there is insufficient factual evidence to suggest that people at the very advanced stages of dementia lose all capabilities. But for the sake of argument, let’s suppose that this is true. This, however, still does not undermine the conceptual rigour of the modified version of Nussbaum’s account. This is because the list of the dementia-specific capabilities that I proposed above is open to include additional items that hold relevance to people in the late stages of dementia. The objection is viable only if we cannot find any sort of (human-like) capacity available to people in the late stages of dementia. I highly suspect that this is not the case.
ConclusionThe modified version of Nussbaum’s account of dignity can better overcome all four objections. It also provides relatively clearer moral guidance on how to care for people with dementia. It is predicated on an empirically informed dementia-specific model of flourishing and can be used as a guiding theoretical framework to conduct further empirical research on what forms of caregiving (do not) align with the moral requirements of respect for the dignity of people with dementia.
Data availability statementData sharing not applicable as no datasets generated and/or analysed for this study.
Ethics statementsPatient consent for publicationAcknowledgmentsI would like to express my sincere gratitude to Distinguished Professor Wendy Rogers and Dr Katrina Hutchison for their continuing support, guidance, and helpful feedback on initial drafts of this paper. This research was supported by a write-up grant from the Macquarie University Centre for Agency, Values and Ethics (CAVE). I acknowledge the support of Distinguished Professor Wendy Rogers in securing the write-up grant. I also extend my gratitude to two anonymous reviewers and the editor(s) of the Journal of Medical Ethics for their insightful and constructive comments on an earlier version of this paper.
留言 (0)