
記住我
The patient is a 59-year-old woman with Goodpasture’s disease on immunosuppressants presenting with hemodynamically significant gastrointestinal bleeding (GIB) requiring blood product transfusion and intensive care unit admission. Initial colonoscopy was notable only for a few non-bleeding, superficial rectal ulcers and a large fecolith. One week thereafter, the patient developed haemorrhagic shock from another GIB, haemoglobin of 5.2 g/L and substantial bright red blood per rectum necessitating emergent blood product resuscitation.
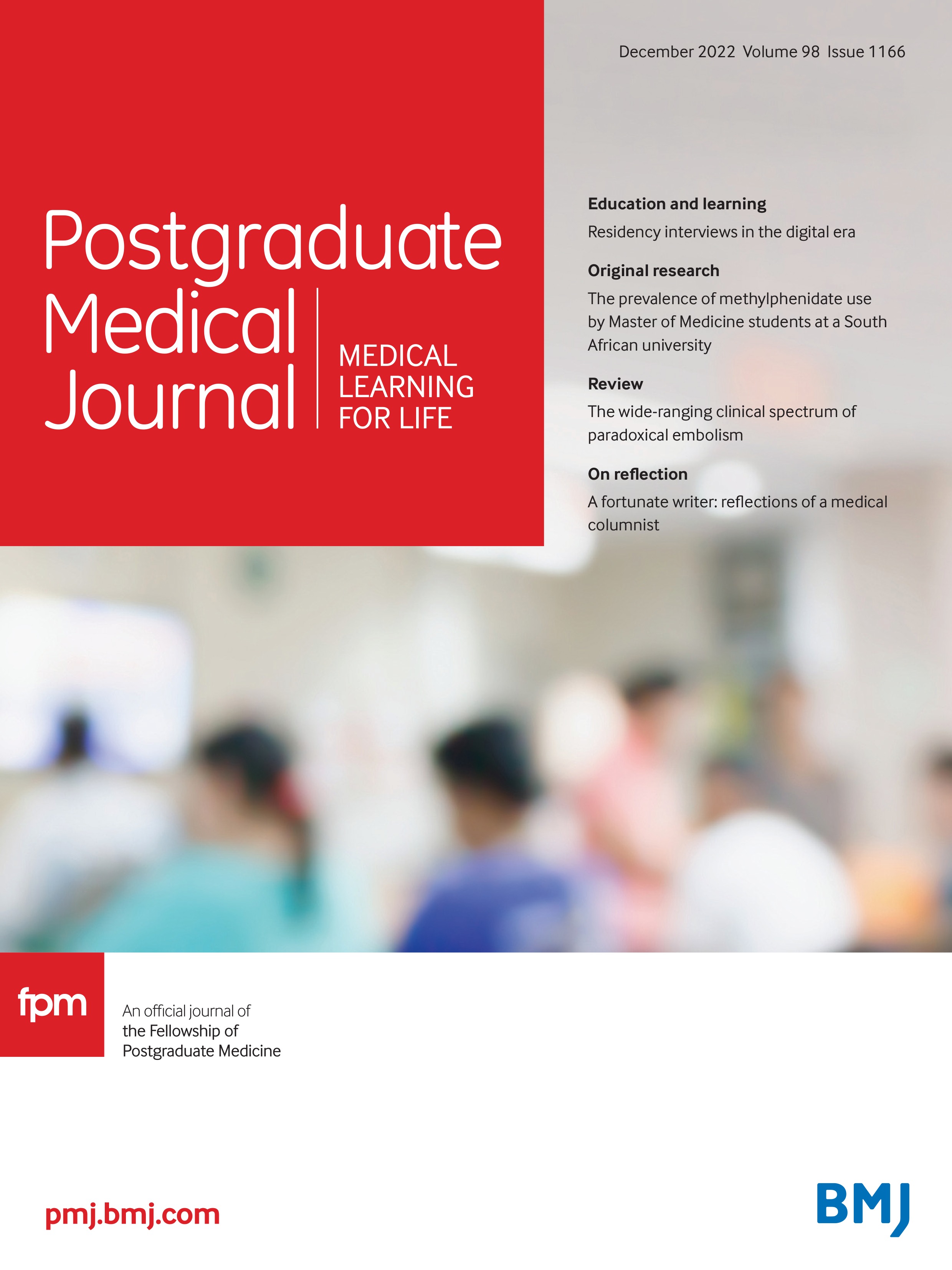
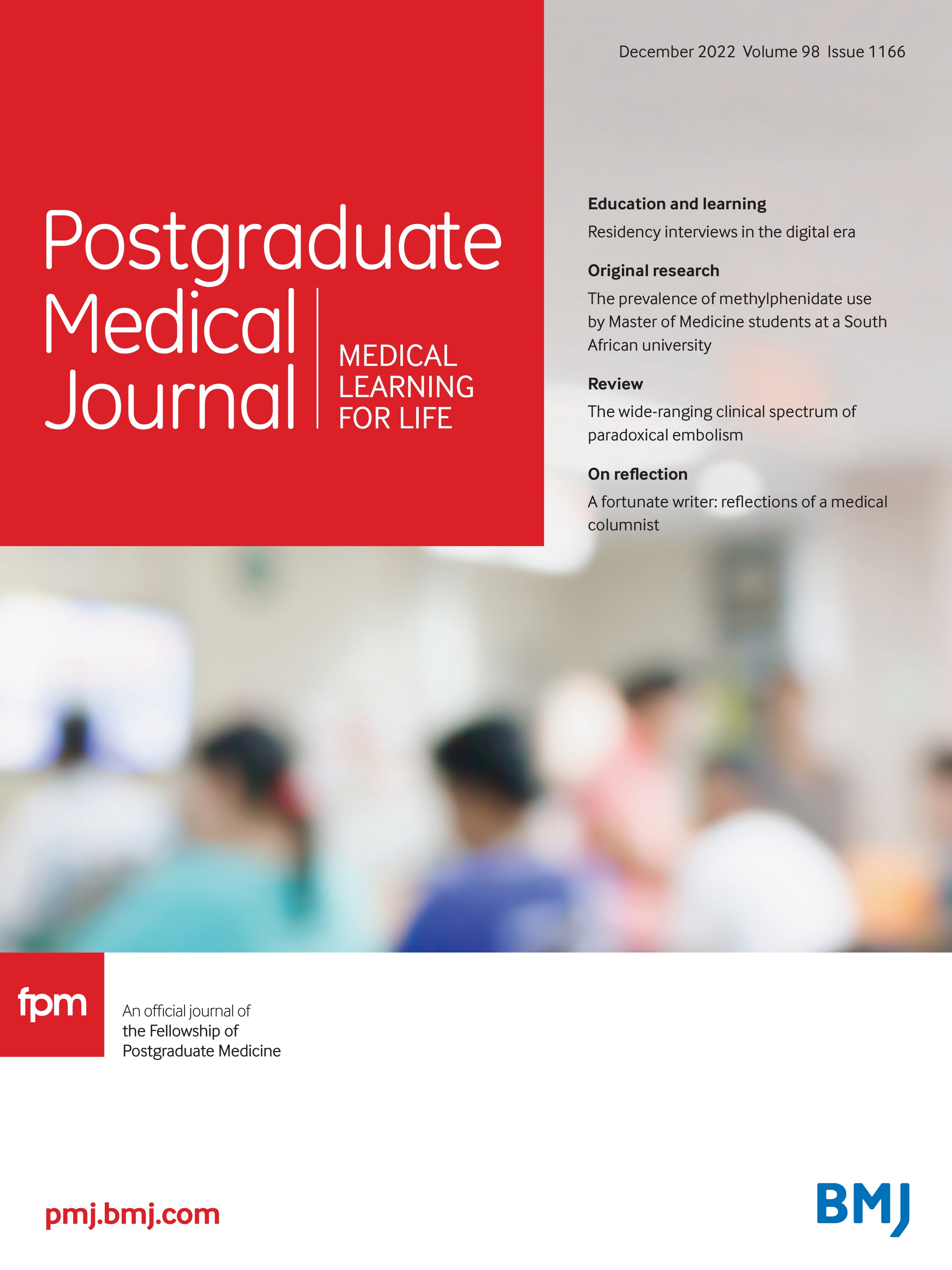
Mesenteric arteriography revealed active extravasation in the rectum (figure 1). Angiographic embolisation with gelform was successful, but she still required addition treatment due to collaterals. Follow-up colonoscopy revealed a single pulsatile visible artery protruding from the 9 O’clock position within the rectal mucosa, 3 cm from the rectum. It was consistent with a Dieulafoy’s lesion (DL) (figure 2) and was definitively treated with a single epinephrine injection and application of two mechanical clips.
 Figure 1
Figure 1 Mesenteric arteriography with contrast extravasation.
 Figure 2
Figure 2 Endoscopic visualisation of a rectal Dieulafoy’s lesion.
DL is a dilated aberrant submucosal arterial vessel of unknown aetiology, typically located in the proximal stomach and duodenum. They are rarely found in other parts of GI tract such as the rectum in this case. DL may lead to massive GI bleeding. According to Baxter and Aly, DL is theorised to occur due to localised mucosal ischaemic damage and acquired vascular ectasia, which erodes through atrophic mucosa.1 The patient most likely had a predisposition secondary to her prednisone use.
留言 (0)