
記住我




During the COVID-19 pandemic (coronavirus disease 2019), frontline employees working in various societal institutions rapidly implemented new routines and everyday practices to hinder spread of infection among pupils, clients, and patients.1,2 Although the consequences for the mental health and working environment among frontline employees have received attention,3–7 the majority of occupational health research during the pandemic has focused on hospital staff.
The death toll in nursing homes for elderly people in Denmark has been low compared with other countries, yet 39% of all COVID-19–related deaths in Denmark have been in nursing homes.8 As they were implementing new initiatives and practices to hinder spread of SARS-CoV-2 infection, the eldercare sector has concurrently experienced shortage of staff, lack of personal protective equipment (PPE), and increased time pressure.9 Worldwide, eldercare workers have been confronted by new ethical dilemmas of balancing safety procedures versus ensuring the quality of life of the elderly.10 At the same time, the public discourse and press coverage might have contributed to stigmatization of eldercare workers as potential carriers of infection.11–13 Thus, eldercare workers have been exposed to several occupational stressors and risk factors for adverse mental health outcomes during the pandemic.14
Lack of risk management in terms of unclear communication, information, and instruction; poor organization of work and ad hoc solutions; insufficient monitoring; training and infection control procedures; and lack of resources, such as PPE, are occupational stressors, which seem to increase adverse mental health outcomes among health care workers during a virus outbreak.14–18 Studies performed in other occupational settings indicate that workplace rumors concerning organizational changes and lack of two-way communication between managers and employees about expected work roles are associated with higher role ambiguity, emotional exhaustion, and job insecurity during the COVID-19 pandemic.19,20 Oppositely, transformational leadership seems to be associated with lower role ambiguity, particularly among employee with low involvement in changes and decisions.21
Also, supportive relations at work buffer the effects on mental health during crises,22,23 which in this sense enhance the individual and organizational resilience. Because of the need of such buffering social relations, it is important to gain knowledge about factors that determine these during crises. Such knowledge contributes to the literature by providing an understanding of the ways organizations can preserve the social environment at work during crises, for example, by their risk management practices. Furthermore, because of the buffering effect of social relations at work, the findings of this study have implications for the prevention of negative mental health outcomes among employees in the eldercare sector.
Against this background, the aim of this study was to investigate if the level of risk management during the initial phase of the COVID-19 pandemic affected the social environment at work. More specifically, we assessed the association of eight indicators of COVID-19 risk management with the perceived changes in conflicts and sense of community among eldercare workers. Furthermore, we hypothesized that workplaces' COVID-19 risk management was particularly important in situations where the external health threat, operationalized as the local SARS-CoV-2 infection rate, was high. Therefore, we also investigated if the association between COVID-19 risk management and perceived changes in the social environment at work depended on the local infection rates in the municipalities, where the workplaces were located.
METHODS Context, Study Design, Data Collection, and Study PopulationCross-sectional data were collected by the labor union, FOA. FOA is the third largest labor union in Denmark, organizing approximately 175,000 members primarily in the public sector. Data were collected from June 16 to July 6, 2020, approximately 3 months after the first SARS-CoV-2–infected case was identified in Denmark. In total, 10,289 currently occupationally active individuals from FOA's voluntary member panel were invited to participate in an electronic questionnaire survey distributed through e-mail. Responses were treated confidentially.
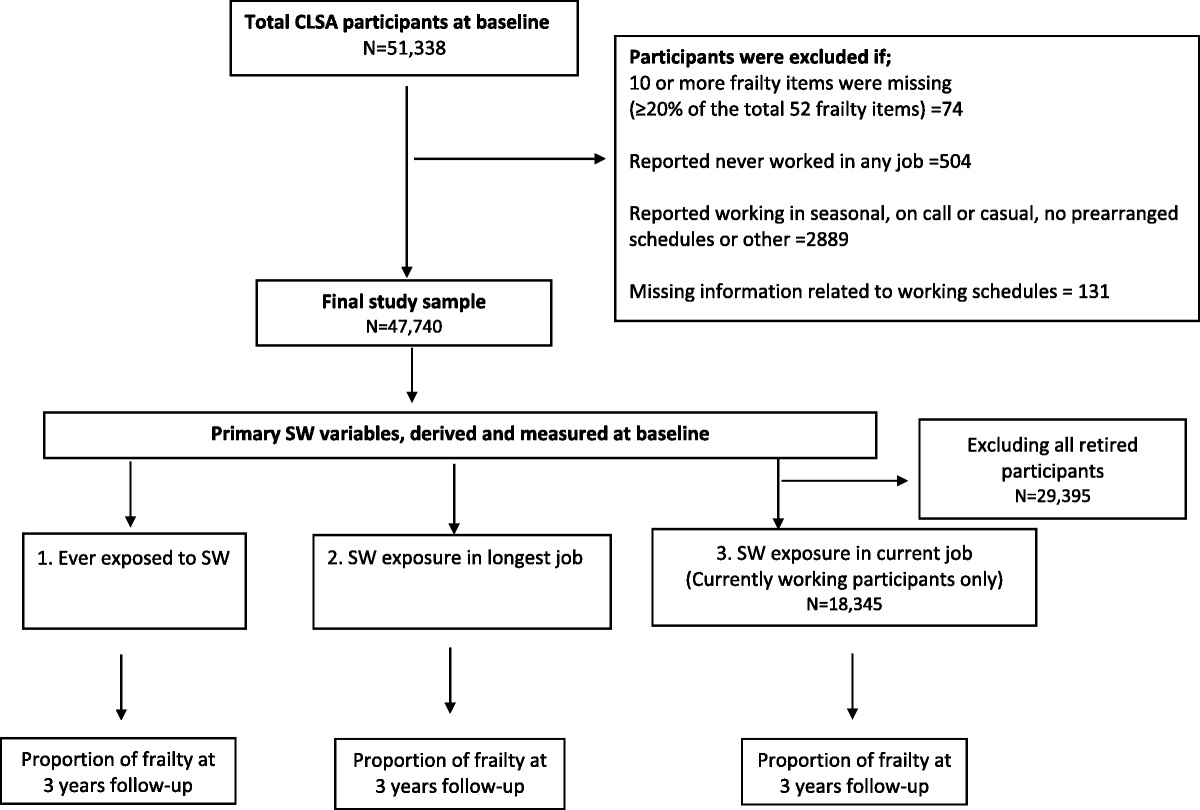
In total, 3624 individuals (response rate, 35%) responded to the questionnaire (Fig. 1). To be eligible for inclusion in the present study, participants had to work in the eldercare as social and health care helper (SHH) or assistant (SHA) (SHHs and SHAs differ in duration of education, and often SHAs have more responsibility for the medication of patients than SHHs24). Furthermore, to be eligible for inclusion, participants should be physically present at their workplace during work, be employed in a municipality, and work in homecare, in a nursing home, or in an activity center. We excluded participants who worked as leaders. We also excluded participants who responded “Not relevant” or “I have not been at work in the past week” to questions about COVID-19 risk management or “Do not know” to questions about the social environment at work.
 FIGURE 1:
FIGURE 1: Flowchart of the selection of study participants.
Social Environment at WorkTo assess the perceived changes in conflicts at work, the participants were asked, “Do you experience more or less conflicts at work compared with before the COVID-19 pandemic?” with the response options: “more,” “around the same amount,” and “less.”
Perceived changes in sense of community among colleagues were assessed by asking the participants: “Has the sense of community among colleagues become stronger or weaker during the COVID-19 pandemic?” with the response options: “It has become stronger,” “It is approximately the same,” and “It has become weaker.”
COVID-19 Risk Management at the WorkplaceTo assess the COVID-19 risk management at the workplace, the participants were asked to indicate if they agreed or disagreed with the following statements: (1) “Management has communicated clear guidelines regarding how employees should act at the workplace during the COVID-19 pandemic”; (2) “I feel secure regarding how my workplace organizes and plans the work during the COVID-19 pandemic”; (3) “My workplace is well-prepared to perform work tasks during the COVID-19 pandemic”; and (4) “The management monitors if the guidelines for the use of PPE are being followed.” The response options were “totally agree,” “partly agree,” “disagree,” “totally disagree” and “do not know.” Response categories were dichotomized, so that “totally agree” and “partly agree” were referred to as “agree.” “Disagree,” “totally disagree,” and “do not know” were referred to as “disagree” as we assumed that COVID-19 risk management was inadequate if the respondents did not know if it was the case or had taken place.
Participants were asked if their workplace paid attention to employees who were particularly vulnerable toward COVID-19. Participants were asked to indicate if their workplace paid attention to six different risk groups listed in the guidelines issued by the Danish Health Authorities: people 80 years or older, people with chronic diseases (eg, cardiovascular disease, lung disease, or diabetes), pregnant women, people with a body mass index of 35 kg/m2 or greater, people with a body mass index of 30 kg/m2 or greater who also have a chronic disease, and other risk groups.25 The variable was dichotomized into those who reported “lack of attention to 0–1 group” and those who reported “lack of attention to 2–6 groups.”
Participants were asked if they had received instruction in the use of PPE. Participants were also asked to indicate if they in the past week had experienced lack of access to PPE. Furthermore, participants were asked to indicate if their workplace had received the resources needed to live up to the Danish Health Authorities guidelines. The response options for these questions were “yes,” “no,” and “do not know.” We dichotomized the response categories into “yes” and “no.” Respondents reporting “do not know” were included in the response option “no.”
COVID-19 Risk Management IndexWe hypothesized that the eight indicators of COVID-19 risk management in our study could be used to construct an index to assess the scope of the workplaces' risk management. Each of the eight indicators included in our risk management index have previously been shown to be associated with mental health outcomes among health care workers during the COVID-19 pandemic.14–18 As such, the indicators have more generally been related to these workers' well-being and functioning.
An overall index for poor COVID-19 risk management was created by calculating a sum score of the eight dichotomized risk management variables (range, 0 to 8), with higher scores indicating poorer risk management. Thus, the index assessed the numbers of actions not taken by the workplaces to handle the COVID-19 pandemic and did not, as such, reflect an underlying “risk management construct” as would have been the underlying assumption when creating a scale.26
Local Incidence Rates of SARS-CoV-2 InfectionsFor each participant, we obtained information about the local cumulative incidence rates of SARS-CoV-2 infections in the municipality of his/her workplace. These data stem from the Danish authorities of Infectious Disease Control (Danish: Statens Serum Institut). Data included information about each of the 98 municipalities in Denmark, and we used data from the offset of the pandemic in Denmark from January 27 to June 16, 2020, where the data collection was initiated.
Sociodemographic Factors and Fear of InfectionInformation about area of work (homecare, nursing home, or activity center) was self-reported. Information about sex, age, municipality of workplace, and job title (SHH, SHA) was obtained from the member's register. Table 1 presents the distribution of the study variables.
TABLE 1 - Description of the Study Population and Local Incidence Rates Across Levels of COVID-19 Risk Management Level of Perceived COVID-19 Risk Management* Total (n = 952) High (Scores 0–1) (n = 383) Moderate (Scores 2–3) (n = 400) Low (Scores 4–8) (n = 169) n % n % n % n % Sex Women 908 95.4 364 95.0 385 96.2 159 94.1 Men 44 4.6 19 5.0 15 3.8 10 5.9 Age ≤39 y 112 11.8 32 8.4 56 14.0 24 14.2 40–49 y 176 18.5 73 19.1 79 19.8 24 14.2 50–59 y 440 46.2 180 47.0 176 44.0 84 49.7 ≥60 y 224 23.5 98 25.6 89 22.3 37 21.9 Job title SHA 520 54.6 217 56.7 211 52.7 92 54.4 SHH 432 45.4 166 43.3 189 47.3 77 45.6 Type of workplace Homecare 380 39.9 130 33.9 167 41.7 83 49.1 Nursing home/activity center 572 69.1 253 66.1 233 58.3 86 50.9 Conflicts among colleagues Less 94 9.9 49 12.8 37 9.3 8 4.7 Same amount 709 74.5 287 74.9 298 74.5 124 73.4 More 149 15.7 47 12.3 65 16.3 37 21.9 Sense of community Weakened 105 11.0 30 7.8 47 11.8 28 16.6 The same 647 68.0 265 69.2 269 67.3 113 66.9 Strengthened 200 21.0 88 23.0 84 21.0 28 16.6 Mean SD Mean SD Mean SD Mean SD Cumulative incidence rate of SARS-CoV-2 infection 168.4 141.8 160.0 135.4 177.2 149.6 166.7 136.7*A higher score indicates poorer risk management.
COVID-19, coronavirus disease 2019; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; SHA, social and health care assistant; SHH, social and health care helper.
In sensitivity analyses, we included fear of infection, which was assessed with the question: “To what degree do you fear to be infected with COVID-19 during work?” with the response options: “not at all,” “to a small degree,” “to some degree,” and “do not know” (reference) versus “to a high degree” and “to a very high degree.”
Statistical AnalysesFirst, we analyzed the distribution of all covariates and the social environment at work across the COVID-19 risk management index. For descriptive purpose, we trichotomized the risk management index into high (scores 0 to 1), moderate (scores 2 to 3), and low risk management (scores 4 to 8) and presented the distribution of covariates across these groups (Table 1). Furthermore, we analyzed the mean score of the local cumulative incidence rates (Table 1).
Second, we analyzed the association between COVID-19 risk management indicators and the perceived change in the social environment at work using multinomial logistic regression, thereby allowing for a nonbinary dependent variable (Table 2). In these analyses, all the measures of COVID-19 risk management were included as binary independent variables. For each COVID-19 risk management variable, the category of “agree”/“yes”/“lack of attention to 0–1 group” was used as the reference group. Analyses were adjusted for sociodemographic factors. All associations are expressed as odds ratios with their 95% confidence intervals. In all analyses, perceived changes in conflicts at work and sense of community among colleagues were included as dependent variables. We calculated the odds of reporting “more” or “less” conflicts as opposed to reporting “the same amount,” and “weakened” or “strengthened” sense of community as opposed to reporting “it is approximately the same.”
TABLE 2 - Associations Between Each of the Eight Indicators of COVID-19 Risk Management and Participants' Perception of Changes in Conflicts and Sense of Community Among Colleagues During the COVID-19 Pandemic Conflicts Sense of community Fewer More Stronger Weaker OR 95% CI OR 95% CI OR 95% CI OR 95% CI Unclear guidelines 0.31 0.94–1.01 2.40 1.45–3.95 0.63 0.34–1.15 1.99 1.13–3.50 Insecurity regarding organization of work 0.47 0.22–1.00 2.37 1.57–3.60 0.61 0.38–1.64 2.28 1.43–3.62 Not well-prepared to perform work tasks 0.90 0.52–1.56 0.94 0.60–1.48 0.90 0.60–1.35 0.92 0.56–1.55 Lack of monitoring of adherence to guidelines 0.97 0.62–1.49 1.11 0.78–1.59 0.93 0.67–1.28 0.85 0.56–1.30 Lack of attention to risk groups 0.65 0.34–1.23 2.31 1.53–3.48 1.16 0.78–1.74 1.93 1.20–3.08 Lack of PPE instruction 0.59 0.33–1.06 1.89 1.28–2.78 0.64 0.43–0.96 2.08 1.35–3.21 Lack of access to PPE 0.48 0.17–1.36 0.63 0.30–1.33 1.23 0.67–2.25 1.48 0.71–3.08 Lack of resources 1.00 0.64–1.56 0.78 0.54–1.12 1.27 0.91–1.78 0.88 0.58–1.34All associations are expressed as ORs with their 95% CIs. All associations are adjusted for sex, age, job title, and type of workplace.
COVID-19, coronavirus disease 2019; CI, confidence interval; OR, odds ratio; PPE, personal protective equipment.
Third, we analyzed the association of the local cumulative incidence rates of SARS-CoV-2 infections and the risk management index with perceived changes in the social environment at work (Table 3, model 1). Results are expressed as the increase/decrease in odds for more/less conflicts and strengthened/weakened sense of community per 100 additional cases per 100,000 individuals. Furthermore, we controlled for the risk management index in the model and estimated the increase/decrease in odds per one-unit increase in the risk management index (Table 3, model 2). Finally, we included the interaction between incidence rates and risk management to investigate the moderating effect of the local incidence rates on the association between COVID-19 risk management and the perceived changes in the social environment at work (Table 3, model 3).
TABLE 3 - Associations of Incidence Rates of SARS-CoV-2 Infections per 100,000 Individuals and the Risk Management Score With the Perception of Changes in Conflicts and Sense of Community Among Colleagues During the COVID-19 Pandemic Conflicts Sense of Community Fewer More Stronger Weaker OR 95% CI OR 95% CI OR 95% CI OR 95% CI Model 1* Incidence rate 0.99 0.85–1.16 0.96 0.85–1.10 0.99 0.85–1.16 0.96 0.85–1.10 Risk management 0.85 0.72–0.99 1.21 1.07–1.35 0.95 0.85–1.06 1.21 1.06–1.37 Model 2† Incidence rate 0.99 0.85–1.16 0.96 0.85–1.10 1.10 0.98–1.23 1.18 1.04–1.36 Risk management 0.85 0.72–0.99 1.21 1.08–1.35 0.95 0.85–1.06 1.20 1.05–1.37 Model 3‡ Incidence rate 1.13 0.88–1.43 0.90 0.70–1.16 1.10 0.91–1.33 1.07 0.82–1.40 Risk management 0.95 0.75–1.21 1.16 0.97–1.39 0.95 0.80–1.13 1.12 0.91–1.14 Interaction term 0.93 0.83–1.05 1.03 0.94–1.12 1.00 0.92–1.75 1.04 0.95–1.14All associations are expressed as ORs with their 95% CIs. A higher score indicates poorer risk management. The OR for “incidence” expresses the increase/decrease in odds associated with 100 additional cases per 100,000 individuals.
*Adjusted for sex, age, job title, and type of workplace. Incidence rate and risk management are not mutually adjusted.
†Adjusted for sex, age, job title, and type of workplace and risk management score. Incidence rate and risk management are mutually adjusted.
‡Model 2 plus interaction term (risk management × incidence rate).
CI, confidence interval; COVID-19, coronavirus disease 2019; OR, odds ratio; PPE, personal protective equipment; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
In sensitivity analyses of the association between the incidence rates and risk management index and the perceived change in the social environment at work, we repeated model 2 with the addition of fear of infection. Furthermore, we stratified analyses of this association across age groups.
RESULTSParticipants did not differ systematically across the three levels of COVID-19 risk management in terms of sex, age, and job title (Table 1). The percentage of employees in homecare was higher among participants reporting poorer COVID-19 risk management (Table 1). We did not find a systematic difference in mean incidence rates across levels of COVID-19 risk management.
Reporting poorer COVID-19 risk management was associated with higher odds of perceived negative changes in conflicts and sense of community for four of eight indicators of risk management (Table 2). More specifically, unclear guidelines, insecurity regarding organization of work, lack of attention to vulnerable employees, and lack of instruction in the use of PPE were significantly associated with more conflicts at work and a weaker sense of community (Table 2).
We observed no association between the local incidence rates of SARS-CoV-2 infections and neither conflicts among colleagues nor sense of community. Instead, we found significantly higher odds of more conflicts and weaker sense of community when scoring higher on the risk management index indicating a poorer risk management (Table 3, model 1). Furthermore, we found no statistically significant interaction between the risk management index and the incidence rates on conflicts or sense of community among colleagues (Table 3, model 3). Therefore, we report the findings from model 2 (Table 3). Like in model 1, we found that reporting poorer risk management was significantly associated with higher odds of more conflicts and lower odds of fewer conflicts (Table 3, model 2). In addition, reporting a poorer risk management or working in a municipality with high incidence rates was significantly associated with a weaker sense of community among colleagues. We found minimal changes in the estimates of model 2, when adjusting for fear of infection. Our age-stratified analyses of model 2 showed that the association between poorer risk management and a weaker sense of community was driven by the oldest age group (aged ≥60 years) in which we found an odds ratio of 1.53 (95% confidence interval, 1.12 to 2.09).
DISCUSSION Main FindingsWe found that inadequate COVID-risk management was associated with perceived changes in the social environment at work, in terms of more conflicts and a weaker sense of community among colleagues. When analyzed separately, four indicators of COVID-19 risk management stood out as being significantly associated with the social environment at work: unclear guidelines, insecurity regarding organization of work, lack of attention to vulnerable employees, and lack of instruction in the use of PPE.
Working in a municipality with a higher incidence rate of SARS-CoV-2 infections was associated with a perceived weaker sense of community, when adjusted for COVID-19 risk management. Yet, our results did not support the hypothesis that adequate risk management was particularly important in a context where the external health threat (ie, the incidence rate) was higher.
Comparison With Previous FindingsWe observed that inadequate risk management was associated with perceived negative changes in the social environment at work among eldercare personnel during the COVID-19 pandemic. Previous studies suggest that lack of risk management can also have other consequences for frontline employees in the health care and eldercare sector: A recent study found that unclear communication and vague division of responsibilities increased fear of infection among eldercare workers during COVID-19.17 Among other groups of health care workers, insufficient access to PPE, unclear rules regarding the use and management of PPE, and limited specialized training in handling COVID-19 patients have been shown to increase anxiety coming from the perceived unfamiliarity and uncontrollability of the hazards involved.14–16 Another study found that lack of trust in equipment and infection control procedures predicted higher levels of emotional exhaustion and state anger and that limited specialized training and unpreparedness were associated with symptoms of burnout and posttraumatic stress disorder.18 Together, these findings indicate that inadequate risk management has various negative effects on well-being and mental health of health care workers with possible implications for their (clinical) practices. Thus, lack of risk management might reduce the resilience of both employees and organizations during crises.
It is well established that (lack of) social relations are associated with various health outcomes, such as all-cause mortality, self-rated health, mental well-being, and cardiovascular function.27–31 For example, the sense of belonging is strongly associated with mental health outcomes, including depression, loneliness, and social anxiety.32 In the context of our findings, a poorer social environment at work might increase the risk of several negative health outcomes for the individual. One potential pathway through which social factors influence health is by buffering the affective and physiological stress reactivity.33 During the COVID-19 pandemic, a recent study of other frontline employees outside the health care sector found that supervisor support eased emotional exhaustion among employees and that coworker support could even protect against the negative effects of inadequate risk management on mental health, for example, by addressing uncertainties fostered by unclear crisis communication.22 Together, these findings indicate that social relations might buffer the negative effects of working in the health care and eldercare sector during the COVID-19 pandemic.14–18 Thus, in the context of our findings, more knowledge on ways to support organizations to provide adequate risk management is needed to improve the resilience of health care workers through support of a good social environment and thereby their ability of handling the crisis.
Strengths and LimitationsThe study is strengthened by the timing of the data collection, which was initiated approximately 3 months after the first lockdown of the Danish society as a response to the COVID-19 pandemic. The data collection was administered by the labor union, FOA, which has a direct and unhindered access to its members. Because of the legitimacy of labor unions among their members, their involvement enhances an agile data collection during extraordinary situations. The drawback, though, is that our data were not collected with a research purpose, which has had implications for the tools used to assess risk management and the social environment at work. To avoid excluding participants responding “do not know” to questions about risk management, we decided to include these respondents in the group that did not confirm, for example, that guidelines were clear, that management monitored adherence to guidelines, that they had access to PPE, and so on. This decision may have resulted in an underestimation of the difference between exposed and unexposed participants.
A major strength of our study is the inclusion of local incidence rates of SARS-CoV-2 cases, as it enabled us to include an objective indicator of the actual external health threat in our analyses. However, because of the low number of individuals being screened for an infection with SARS-Cov-2 in the first phases of the pandemic, the recorded incidence rates are most likely seriously underreported. Yet, as this underreporting was apparent in all municipalities, we expect that this did not substantially inflict on our results. Theoretically, it could be postulated that the risk management strategies applied in the present study would affect the local incidenc
留言 (0)