Search terms such as “fumigants”, “methyl bromide”, “hydrogen phosphide” “hydrogen cyanide”, “sulfuryl fluoride”, “chronic health effects”, “chronic exposure” “examinations” and surveillance” were also searched in PubMed, Medline and the Cochrane Database of Systematic Reviews. This paper also referenced international guidelines from various countries and key occupational health and safety agencies such as Occupational Safety and Health Administration (OSHA), National Institute of Safety and Occupational Health (NIOSH), Health Safety Executive (HSE), Health Protection Agency (HPA), Enviromental Protection Agency (EPA) and the various Safety Data Sheet (SDS) of the fumigants on reported chronic effects.
Of note, while physicians should also screen for symptoms and signs of acute toxicity and prior episodes of acute exposures during routine medical examination, this paper will mainly focus on the chronic health hazards of Methyl Bromide, Hydrogen Cyanide, Hydrogen Phosphide and Sulfuryl Fluoride and outline guidance to identify chronic health hazards during routine medical examinations.
Methyl bromide
Methyl Bromide (MeBr), also known as bromomethane or monobromomethane is a broad-spectrum pesticide with a long history of use as a fumigant. MeBr is a colourless gas at room temperature which has no odour or taste at low concentrations. At high concentrations, MeBr has a musty or fruity odour. In the gaseous state as fumigants, MeBr, is more than three times as dense as air and may collect in low spots and poorly ventilated places and can penetrate many substances such as concrete, leather and rubber [5,6,7,8,9].
MeBr is well absorbed via inhalation and is rapidly distributed to many tissues including lungs, adrenal glands, kidneys, liver, nasal turbinate, brain, testes, and adipose tissues. It can also penetrate the blood brain barrier, affecting the Central Nervous System (CNS) [5, 7, 9, 10]. It has a half-life of 12–14 days and is excreted in urine and via exhalation. Of note, a lachrymatory agent such as chloropicrin is often added to act to MeBr as a sensory warning agent. Chloropicrin has a pungent odour and causes eye irritation and its main health effects are lacrimation, irritation, cough and chest pain [5, 7, 11].
The Global Harmonised System of Classification and Labelling of Chemicals (GHS) classifies MeBr as toxic [12]. Fatalities have occurred amongst fumigators who were exposed to MeBr during application or who have prematurely re-entered fumigated premises [5]. MeBr methylates the sulfhydryl groups of enzymes and causes cellular disruption and reduced glutathione levels [7, 9,10,11,12]. Importantly, the cellular disruption occurs primarily in the CNS subsequently causing progressive neurological dysfunction. It has been reported that MeBr has a greater potential for toxicity than do other organic bromides because of its greater lipophilicity which provides increased access to the brain [18]. Of note, it is postulated that methanol, which is a metabolite of methyl bromide, may also contribute to the neurologic and visual effects in high levels of exposure [7, 9,10,11,12].
Chronic exposure to MeBr may result in neurological effects such as peripheral neuropathy, impaired gait, behavioural changes, mental confusion, lethargy, loss of coordination and muscle weakness [7, 9, 11, 13]. Visual impairment arising from optic atrophy has been reported following chronic exposure [9]. In fact, Chavez et al. reported that a fumigator who was chronically exposed to MeBr developed paraesthesia of the extremities, dysesthesias, and visual impairment secondary to optic atrophy [14]. MeBr is also listed as a skin irritant and so, repeated exposure may cause contact dermatitis [7, 9, 11]. However, there is no evidence that MeBr can induce.
sensitization [9, 15]. Of note, while chronic exposure to MeBr results in mild kidney or liver damage, elevated liver enzymes, proteinuria and haematuria is often seen after acute exposure only [4]. As such, liver function tests, renal panel and urine analysis have little value in evaluating for chronic exposure to MeBr.
A meta-analysis by Budnik et al. reported that overall exposure to MeBr is associated with an increased risk of prostate cancer with an odds ratio of 1.21 [16]. However, the International Agency for Research on Cancer has classified MeBr as a Group 3 carcinogen due to inadequate evidence to its carcinogenicity [6, 7, 9, 12]. No reproductive or teratogenic effects have been reported [6, 7, 9, 12].
Routine medical examinations should therefore identify workers who have medical conditions involving CNS, skin, liver, renal and respiratory system. For example, as MeBr is a skin irritant, workers with eczema can be at a higher risk of developing irritant reactions if exposed. The evaluation should also include a systemic evaluation of symptoms and signs to assess if workers have undiagnosed medical conditions such as kidney disease, chronic lung disease, skin conditions. Workers who have pre-existing medical conditions involving these systems should be counselled on the potential risk of exposure to MeBr and the increased susceptibility of developing health hazards.
Medical examinations should also entail (i) a skin examination looking for evidence of contact dermatitis, frostbite, or burns; and (ii) neurological examination particularly focusing on gait, peripheral and cerebellar systems looking for neurological features of chronic exposure. In patients with abnormal neurological features, physicians can consider performing laboratory investigations such as a full blood count (FBC) to rule out other causes of peripheral neuropathy. For example, megaloblastic anaemia secondary to B12 deficiency could result in peripheral neuropathy, thus negating Methyl Bromide as the cause of the deficit. In addition, direct fundoscopy and visual acuity should also be undertaken to look for optic atrophy. Such routine examinations aid in identifying chronic health effects that could have resulted from exposure at work. Likewise, workers who, upon examination are detected to have abnormal examination findings should be evaluated further to ascertain fitness to work (refer to Table 1). Of note, While blood bromide can be measured at the end of the shift at the end of the work week, it is only useful if it is done within 1 to 2 days following exposure and hence will not be a good indicator of chronic exposure. There is currently no recognised biological occupational exposure limit for urine bromide [11, 17].
Table 1 Overview of routine medical examinations
Hydrogen phosphide
Hydrogen Phosphide otherwise known as Phosphine or Trihydrogen Phosphide is a colourless gas and has an odour of garlic or decaying fish [18, 19]. Of interest, the level at which humans detect the odour of Hydrogen Phosphide does not provide sufficient warning of dangerous concentrations [18,19,20]. Exposure to gaseous Hydrogen Phosphide is mainly via inhalation, and is rapidly absorbed and is distributed throughout the body leading to the effects on the respiratory, cardiovascular, and CNS [18].
Hydrogen Phosphide inhibits the body’s ability to produce proteins [18,19,20,21]. Furthermore, it has been postulated that Hydrogen Phosphide inhibits cytochrome c oxidase and mitochondrial oxygen uptake. However, this has not been proven in-vivo studies [21]. Most of the absorbed phosphine is excreted in exhaled air and minor amounts are oxidised and excreted in the urine as hypophosphite and phosphate. The biological half-life of phosphine has not been reported and may be difficult to estimate [18, 19]. Of note there are no biological indicators for exposure to phosphine [19].
The chronic effects of long-term or repeated exposure to Hydrogen Phosphide are generally distinct from acute poisoning. Of note, published data on chronic health effects to Hydrogen Phosphide are limited [17]. Several international guidelines have highlighted that health effects due to repeated exposures can result in bronchitis with cough, phlegm, or shortness of breath, anaemia, speech and motor disturbances, toothache, swelling of the jaw, mandibular necrosis, and spontaneous fractures [19, 21,22,23]. Hydrogen Phosphide is not considered to be mutagenic in vivo. It is not classified as a human carcinogen. No reproductive or teratogenic effects from exposure have been reported [24].
As Hydrogen Phosphide is a respiratory irritant, those with impaired pulmonary function, would be susceptible to the irritant effects of Hydrogen Phosphide [22]. As such, workers who have chronic lung conditions should be deemed unfit for work. Additionally, workers should also be counselled to stop smoking, as it can exacerbate the respiratory effects. For example, a study analysing percentage changes in FEVI and FVC suggested that smoking behaviour and occupational exposure significantly “affected percentage changes in lung function” [25].
Routine medical examination should therefore include (i) history, examination and full blood count evaluating for anaemia; (ii) history of soft tissue swelling, jaw pain, dental problems, and discharge looking for evidence of mandibular necrosis; (iii) neurological examination evaluating for chronic effects of Hydrogen Phosphide such as motor and speech deficits; and (iv) respiratory history and examination (refer to Table 1). Workers with abnormal findings should undergo further evaluation. For example, a worker with abnormal findings indicating mandibular pathology should undergo further imaging such as Intraoral (periapical and bitewing) and panoramic radiographs [26].
A baseline spirometry should be done at the pre-licence examination to establish a reference point for future surveillance and assess worker’s respiratory function to ascertain fitness to work [20]. Spirometry should be repeated if worker has abnormal respiratory examination findings, or symptoms from the routine medical examinations. ACOEM proposed that a “confirmed decline of FEV1 of 10–15% as compared to baseline lung function, requires further medical evaluation” [27].
Hydrogen cyanide
Hydrogen Cyanide (HCN) is a systemic chemical asphyxiant with a bitter almond odour which is often described as having a “musty old sneakers smell” [28,29,30]. Unfortunately, the odour does not provide adequate warning of hazardous concentrations. Due to its small size and moderate lipid solubility, HCN is rapidly absorbed and distributed into body tissues. Following inhalation, HCN is distributed to the lungs, blood, brain and kidneys. On the other hand, post ingestion, it is found in the stomach or other parts of the gastrointestinal tract mostly [28, 30, 31].
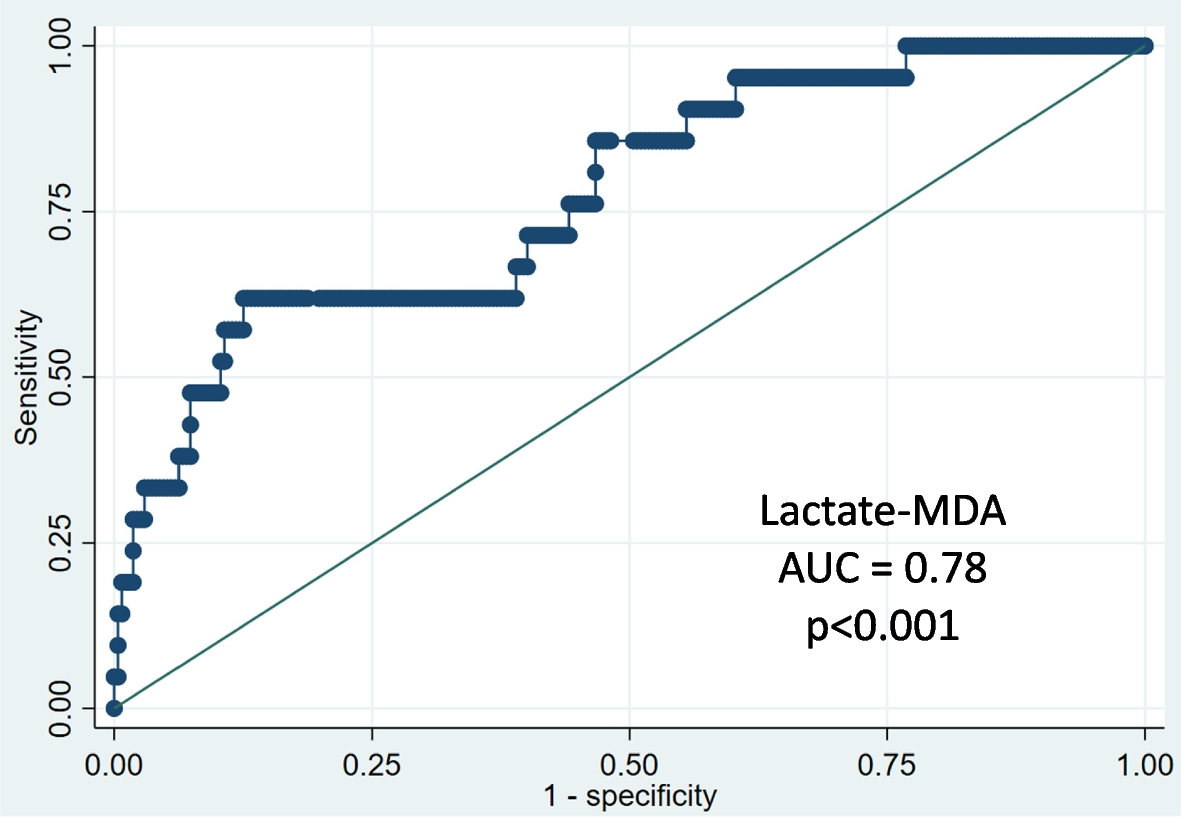
HCN interferes with the normal use of oxygen by nearly every organ of the body and does so via various mechanisms of toxicity. Firstly, cyanide ion blocks oxidative respiration thus causing tissue hypoxia especially affecting the tissues with high metabolic demand such as CNS which are key targets for toxicity [28, 30,31,32]. Such inhibition of oxidative metabolism gives rise to lactic acidosis. Secondly, cyanide induces the release of neurotransmitters such as N-methyl-D-aspartate (NMDA), resulting in seizures [28, 30,31,32]. Thirdly, release of biogenic amines also results in the pulmonary and coronary vasoconstriction [28, 30,31,32].
It is postulated that HCN is irreversibly metabolised via the enzyme rhodanese to the less toxic form of cyanide known as thiocyanate [25, 29]. Rhodanese can be found in mitochondria of tissues and commonly found in liver, kidney, brain, and muscles [28, 32]. Majority of absorbed cyanide is excreted as thiocyanate in the urine while small amounts are excreted unchanged in lungs, saliva, sweat, urine or converted to carbon dioxide in expired air. The plasma half-life of HCN is 2 to 3 h [28, 32].
Chronic exposure may result in non-specific symptoms such as headache, fatigue, and anorexia. Respiratory tract irritation, breathlessness, hoarse voice and chronic rhinitis have also been reported [28, 30,31,





留言 (0)