
記住我
In sub-Saharan Africa, the prevalence of depression among persons living with HIV (PLWH) ranges from 9% to 32% (1,2). In areas such as postconflict northern Uganda, with estimated rates of depression as high as 70%, PLWH remain particularly vulnerable to developing depression (3). Insufficient attention to identifying and addressing mental health needs of PLWH has been recognized as a barrier to meeting World Health Organization guidelines for universal antiretroviral therapy (ART) in this population (4,5).
Previous research has shown that untreated depression among PLWH is associated with adverse HIV treatment outcomes, including suboptimal medication adherence, viral nonsuppression, and increased mortality (6–9). These challenges are more prominent in postconflict settings where extreme poverty, food insecurity, and poor access to psychological care are common (10). Research is emerging in sub-Saharan Africa and other low- and middle-income countries on the development and evaluation of mental health interventions for PLWH (11–16). A recent systematic review of mental health interventions for PLWH in low- and middle-income countries indicated strong evidence that the common mental health problems that PLWH face—including depression, anxiety, and posttraumatic stress disorder—are responsive to first-line psychological treatments (17).
There remains a need to understand the underlying mechanisms through which mental health interventions impact HIV treatment outcomes. The outcome of prior research on this subject has been variable, with some studies reporting improved depression and HIV treatment outcomes (18), whereas others report only improved depression outcomes (19). More recent meta-analyses indicate that depression treatment improves ART adherence and viral suppression (20,21).
In Uganda, we developed culturally sensitive group support psychotherapy (GSP) as a first-line treatment of depression in rural primary care settings. A prior feasibility study (22) and pilot randomized clinical trial (23) of this intervention served to test procedures, recruitment, retention, and outcomes. Evaluation of process outcomes (24) indicated that acquisition of knowledge and skills enhanced social connections, support, and positive coping strategies, which led to a reduction in depression symptoms. However, the sustainability and impact of these interventions on HIV treatment outcomes were not studied.
Subsequently, we used a cluster randomized controlled trial to examine the intent-to-treat GSP effects through 24 months by comparing GSP with an active comparison, group HIV education (GHE) (25). At 12 months, GSP was more effective in treating mild to moderate depression in PLWH than GHE. Improvements in HIV treatment outcomes were greater among GSP than GHE participants; however, this difference was not statistically significant.
The current analysis aimed to document intent-to-treat GSP effects on HIV treatment outcomes for 24 months. GSP effects were compared with GHE on depression, ART adherence, and viral load suppression 24 months after treatment. We also investigated the mediating role of sequential changes in depression and ART adherence at 12 months in the relationship between GSP and viral load suppression at 24 months. We hypothesized that GSP may lead to a sustained greater reduction in depression when compared with GHE, which would lead to improved ART adherence and viral suppression.
METHODS Study DesignWe report the 2-year outcomes of a pragmatic two-arm cluster randomized trial where 30 HIV clinics across three districts (Gulu, Kitgum, Pader) in postconflict northern Uganda were randomly assigned to deliver either GSP or GHE. HIV clinics eligible for the trial nominated at least four lay health workers (LHWs) involved in HIV care who were able to read and write, and who resided within the villages served by the clinic.
Participants were PLWH on ART, 19 years and older with major depression, and antidepressant naive. Individuals with high suicide risk, severe medical disorder (e.g., pneumonia or active tuberculosis) psychotic symptoms, or hearing or visual impairment were excluded. Mild to moderate depression and adherence rates ≥95% were evaluated at baseline and 6, 12, 18, and 24 months after treatment. Viral load was obtained from medical charts at baseline and at 12 and 24 months after treatment.
Details of the recruitment have been published elsewhere (26). The study protocol is published (27) and registered in the Pan African Clinical Trials Registry PACTR201608001738234. The study was approved by both the Makerere University College of Health Sciences Research Ethics Committee and the Uganda National Council of Science and Technology. At the end of the treatment, all participants received 8000UGX (US $2.16) to defray transportation costs. The group facilitators received 80,000 UGX ($21.62) for compensation. Figure 1 summarizes the trial profile.
 FIGURE 1:
FIGURE 1: Flow diagram of trial health centers and participants. GHE = group HIV education; GSP = group support psychotherapy.
Randomization and MaskingHealth center managers were invited to a stakeholders’ meeting at the district’s local government offices where our study purpose and procedures were explained to facilitate district leadership understanding of the trial. We randomized at the level of health centers by urn randomization (health center managers separately picked a paper containing the intervention allocation from a basket; ratio 1:1). By design, both experimental and control interventions were identifiable to participants and outcome assessors, but masked to the Data and Safety Monitoring Board, and data analysts up to 12 months after treatment.
ProceduresPrimary care health workers delivered a health talk on depression to clients in the waiting area. Clients who felt that they had experienced symptoms of depression were invited for further evaluation. Clients diagnosed with major depression were approached by research assistants who explained study procedures, determined eligibility, and then obtained informed consent. Each client who gave informed consent received baseline assessments with a standardized questionnaire. Recruited participants from the same village were assigned to a trained LHW residing in or near their village to receive either GSP or GHE.
The contents of the GSP and GHE interventions were described in previous publications (23,24). GSP was delivered in eight weekly sessions, each lasting 2 to 3 hours. Participants were divided into sex-specific groups of 10 to 12 participants. Trained lay health workers delivering the intervention were of the same sex as the participants, and delivered the intervention material following a scripted manual. The target community was involved in the development of this intervention, thus making it culturally sensitive intervention. Cultural sensitivity is defined as being aware that cultural differences and similarities between people exist and affect values, learning, and behavior (28,29).
In developing GSP, a qualitative study of perceptions of depression and its local treatment strategies among the target population was completed (30). The most commonly used coping skills were similar to those previously reported in other African studies (31), such as faith/religion, social support, communal activities, distraction, acceptance, and cognitive reframing or meaning making. We designed GSP sessions to begin and end with rituals, such as a cultural song, dance, or prayer chosen by participants. Homework assignments were designed to enhance participation in communal activities and enhance social connections.
The first session addressed issues related to the group process, expectations, ground rules, and commitment after which participants were paired and each pair asked to interact in the week and provide feedback on their activity. The second session addressed triggers, symptoms, treatment options for depression, and the relationship between depression and HIV. Thereafter, participants were asked to communicate with community members and share newly learned knowledge. In our previous research, the target community attributed the cause of depression to ancestral spirits and witchcraft (30); hence, there is a need for a session on psychoeducation, which has been shown to increase treatment engagement and reduce attrition (32).
In sessions 3 and 4, group participants shared their most painful experiences. Thereafter, participants were encouraged to share other problems with a trusted elder in their household or community. Previous research has shown that catharsis is followed by decreased tension, increased mental clarity and feelings of well-being, and emotional stability (33,34). In sessions 5 and 6, GSP participants shared ways in which they cope with depression, whereas the group facilitator provided guidance on the use of positive and negative coping skills. In previous research (30), unhelpful coping strategies have been associated with depression in PLWH (35).
The last two sessions were dedicated to income-generating skills. Our previous research revealed a need for an intervention that focused on treatment of depression symptoms and skills development to improve participant livelihood (30). Poor mental health interacts with poverty in a negative cycle, and researchers have called for development of interventions that could break this cycle (36).
The first GHE session focused on rationale for HIV education and orientation, and the second session focused on the progression of HIV. The third and fourth sessions covered transmission and prevention of HIV infection, and the fifth and sixth sessions covered mother-to-child transmission. The last two sessions focused on basic facts about ART. Group members were allowed to ask questions at the end of every session (for details of the training of the lay health workers, see Supplemental Digital Content 1, Boxes 1 and 2, https://links.lww.com/PSYMED/A866).
Strategies to ensure fidelity in both arms included the use of standardized intervention materials, structured health worker training, and ongoing supervision. LHWs delivered the interventions following a manual translated into the local language and were supervised by trained health center workers who had participated in the earlier pilot trial (23).
OutcomesWe assessed depression using the major depressive episode module of the Mini-International Neuropsychiatric Interview (6.0; based on the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition) (37). Functioning was evaluated using a five-item locally developed function assessment measure (38). Items were derived from qualitative interviews with individuals and their caregivers in the target population about participant expectations regarding function outcomes (38). The five categories of tasks assessed included household (e.g., washing clothes), field (e.g., grazing animals), social (e.g., attending social events) and job-related or school-related tasks (e.g., participating in income-generating activities), and tasks related to personal hygiene (e.g., bathing). Participants were asked to rate their ability to do a given task on a 3-point scale, with responses ranging from 0 (“No, I am not able”), and 1 (“Yes, but not like before”), to 2 (“Yes, I am able to”). Summary scores ranged from 0 to 10. The measure attained a Cronbach α reliability coefficient of .86 in this study population.
The SAD PERSONS scale was used to assess suicide risk (39) at each assessment point. Also, the total number of suicide attempts before each time point was recorded. The study cohort was monitored closely for suicide attempts and other adverse events (AEs). All trained lay health workers in both intervention arms made weekly home visits to remind caregivers to closely monitor and report any AEs. When a suicide attempt occurred, it was reported to LHWs and the study team, who took steps to confirm the incident. Once confirmed, the incident was reported to the principal investigator, the institutional review board, and the data safety and monitoring board (for details on AEs, see Supplemental Digital Content 1, https://links.lww.com/PSYMED/A866).
Adherence to ART was measured by one question: “during the past week, on how many days have you missed taking all your medication doses?” Using the responses, we computed a binary variable with <95% adherence coded 0 and those with ≥95% adherence rates coded 1. Viral load was assessed every 12 months and at variable times for each PLWH (standard in Uganda). Visits to assess viral loads preceded the study visits for the 6-month interval assessments, and we did not assess the difference in timing. Measures of viral load were obtained from the medical charts of study participants, but the actual assay used to measure viral load in the laboratory was not recorded. We computed a binary variable where individuals with <1000 viral copies per milliliters were categorized as being suppressed (coded 1), whereas those with ≥1000 as nonsuppressed (coded 0).
Statistical AnalysesData were analyzed using STATA version 16. First, we conducted bivariate analyses using cluster adjusted χ2 tests and t tests to compare baseline variables between GSP and GHE participants. We also conducted bivariate analyses to compare these variables between those who completed all follow-up assessments (completers) and those who had not (noncompleters). Given the clustered nature of our data and the need to adjust for covariates in our analyses, missing values were multiply imputed 20 times assuming a joint multivariate normal distribution (Supplementary File 1, https://links.lww.com/PSYMED/A866). We used the postestimation STATA program how_many_imputations to determine the number of imputations needed (40). A multivariate normal regression model allows interdependencies within clusters and enables all clusters to be imputed simultaneously. Furthermore, simulation studies have shown that assuming an MVN distribution leads to reliable estimates given a large sample size even when the normality assumption is violated (41–43).
Specifically, the STATA command mi set was used for these imputations. We then used the STATA command mi impute mvn to specify the imputation model and to create 20 imputed datasets. Sex, age, education, marital status, employment, and intervention arm were used for these imputations. We did not include transformed variables in the imputation model.
All regression models used to evaluate the effect of GSP on depression and HIV treatment outcomes were estimated using multiply imputed data. Four separate models were analyzed in which the dependent variables were depression, function scores, ART adherence, and viral suppression. In each model, the independent variables included intervention arm, time (ordinal variable in 6-month units capturing the effect of time), and the interaction of study arm by time (capturing the effect of each additional unit of time among GSP participants relative to GHE participants). See detail in Supplemental Digital Content 2, https://links.lww.com/PSYMED/A867.
Given that randomization was performed at the cluster (health center) level, some baseline variables were not comparable between the study arms at baseline. Therefore, multiple imputation was used given the adjustment of covariates in the multilevel mixed regression models. All multilevel regression models were adjusted for covariates (employment status, marital status, function scores) repeated measures nested within person and person nested within health worker (44). Therefore, the models contained random intercepts at the health worker and person levels (three-level models). In the mediation analyses using generalized multilevel structural equation modeling (GSEM), only a random intercept term for health worker was introduced (two-level models).
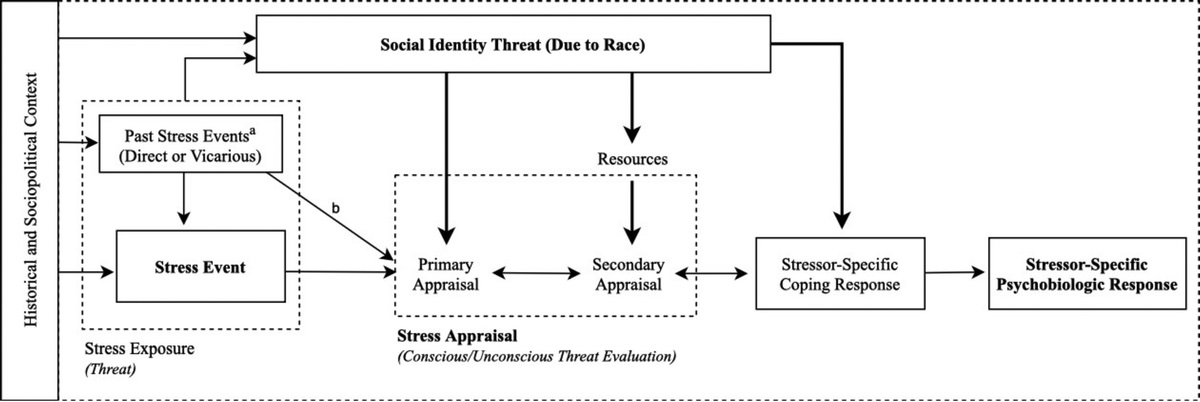
In the mediation model (Figure 2), viral suppression is the dependent variable, therapy group is the independent variable, and depression and ART adherence are the two mediators. We used GSEM to estimate coefficients for depression on therapy group (β1), ART adherence on therapy group (β5), and ART adherence on depression (β2), as well as coefficients for viral suppression on depression (β6), viral suppression on ART adherence (β3), and viral suppression on therapy group (β4), while considering the nesting of the data into therapy groups (45). All models included time and therapy group and its interaction. For binary outcomes, the Stata command gsem was used with a binomial family distribution and a logit link.
 FIGURE 2:
FIGURE 2: Generalized multilevel structural equation modeling to estimate coefficients for depression on therapy group (β 1), ART adherence on therapy group (β 5), and ART adherence on depression (β 2), as well as coefficient for viral suppression on depression (β 6), viral suppression on ART adherence (β 3), and viral suppression on therapy group (β 4), while taking into account the nesting of the data into therapy groups. All models included time and therapy group and its interaction. Arrows denote associations; ε in circles represents error terms for each of the outcome (Y) and mediators (M1, M2) regressions. X, therapy group (group support psychotherapy coded 1, group HIV education coded 0); M1, depression symptoms; M2, ART adherence; ART, antiretroviral therapy; Y, viral suppression.
We conducted cross-sectional mediation analyses using the nlcom (nonlinear combination) STATA command to compute the indirect effect coefficients and their standard errors at each time point as shown in Table 1 (46). Next, we used sequential mediation analysis to examine if the effects of therapy group on viral load at 24 months were mediated by sequential changes in depression and ART adherence at 12 months (47). We again used nlcom command to compute the indirect effect coefficients and their standard errors for depression and ART adherence at 12 months separately and thereafter obtained indirect effects for sequential changes in depression and adherence. We then computed the total indirect effect by summing up the indirect effects through depression and ART adherence at 12 months in the relationship between therapy group and viral suppression at 24 months with the indirect effects through depression in the relationship between therapy group and ART adherence. Lastly, we ran nlcom to compute the total effects by combining direct effect of therapy group on viral suppression at 24 months and the total indirect effects. Bootstrap standard errors and bootstrap bias-corrected confidence intervals were computed for all effects (48).
TABLE 1 - Cross-Sectional Direct, Indirect, and Total Effects of Group Support Psychotherapy Through Depression and ART Adherence on Viral Suppression β SE Bootstrapped 95% CI p Baseline Indirect effects through adherence −0.010 0.005 −0.020 to 0.0001 .053 Indirect effects through depression 0.013 0.007 −0.001 to 0.027 .059 Indirect effects through depression and adherence 0.003 0.01 −0.014 to 0.02 .723 Total indirect effects −0.470 0.214 −0.889 to −0.051 .028 Total effects −1.052 0.359 −1.76 to −0.348 .003 12 mo after treatment Indirect effects through adherence −0.0014 0.004 −0.01 to 0.006 .730 Indirect effects through depression −0.038 .011381 −0.060 to −0.015 .001 Indirect effects through depression and adherence −0.039 0.012 −0.063 to −0.015 .001 Total indirect effects 1.336 0.215 0.915 to 1.756 <.001 Total effects 1.184 0.358 0.48 to 1.89 .001 24 mo after treatment Indirect effects through adherence 0.007 0.005 −0.002 to 0.016 .124 Indirect effects through depression −0.089 0.023 −0.135 to −0.043 <.001 Indirect effects through depression and adherence −0.081 0.024 −0.128 to −0.035 .001 Total indirect effects 3.14 0.226 2.69 to 3.58 <.001 Total effects 3.421 0.372 2.69 to 4.15 <.001ART = antiretroviral therapy; SE = standard error.
Between September 13 and December 15, 2016, we assessed 1473 individuals, of whom 1140 were recruited from health centers offering GSP (n = 578) or GHE (n = 562). Figure 1 illustrates the trial profile. Regarding intervention attendance, 33 of 578 GSP (6%) and 15 of 562 GHE (3%) participants missed all sessions. Individuals who did not attend any group session were not excluded from follow-up assessments. Four hundred fifty of 578 GSP (78%) and 502 of 562 GHE (89%) participants attended all eight group sessions. Details of group session attendance by intervention group have been included in Supplemental Digital Content 1, https://links.lww.com/PSYMED/A866. Comparisons of baseline variables between the treatments arms are shown in Table 2. More detail is included in Supplemental Digital Content 3, Table 1, https://links.lww.com/PSYMED/A868. Attrition was greater in the GHE than GSP group at 24-month follow-up (84 [15%] versus 43 [7%]). In comparison to study completers, noncompleters were more likely to be male (56% versus 25%), had more viral nonsuppression (42% versus 30%), less suicide risk (72% versus 56%), and more hazardous alcohol consumption at baseline (40% versus 29%; Supplementary Digital Content 1, https://links.lww.com/PSYMED/A866).
TABLE 2 - Baseline Study Population Characteristics Variable GSP (n = 578), n (%) GHE (n = 562), n (%) Cluster-AdjustedGSP = group support psychotherapy; GHE = group HIV education; SD = standard deviation; ART = antiretroviral therapy.
By the 24-month follow-up study visit, we had recorded 89 serious AEs in 49 participants. These included 25 suicide attempts, 35 hospital admissions, and 29 deaths. Four of the deaths were completed suicides (GSP, 2; GHE, 2), and 25 were medical related deaths (GSP, 17; GHE, 8). All the 25 study participants who attempted suicide were referred to the district hospital or health centers for management. However, of these, only 12 had the resources to access hospital care. The rest were kept under close observation by relatives, caregivers, and lay health workers who made weekly home visits. AEs reported by 24 months after the end of treatment are summarized in Supplemental Digital Content 1, https://links.lww.com/PSYMED/A866.
Depression CasesFewer GSP than GHE participants met the criteria for major depression at 6 months (2% versus 30%; adjusted odds ratio [aOR] = 0.013, 95% confidence interval [CI] = 0.004–0.035), 12 months (2% versus 41%; aOR = 0.011, 95% CI = 0.004–0.029), 18 months (1% versus 29%; aOR = 0.013, 95% CI = 0.004–0.036), and 24 months (1% versus 25%; aOR = 0.002, 95% CI = 0.0002–0.018). See detailed results in Supplemental Digital Content 3, Table 2, https://links.lww.com/PSYMED/A868. Figure 3 in Supplemental Digital Content 4, https://links.lww.com/PSYMED/A869, illustrates the multilevel mixed-effects regression model of GSP effects on depression using raw data (complete cases) adjusted for baseline employment, marital status, function scores, and ART adherence.
Function ScoresGSP participants had higher function scores than those receiving GHE at 6 months (mean [standard deviation ] = 9.87 [0.86] versus 6.83 [2.85]; β =4.10, 95% CI = 3.75–4.44), 12 months (mean [SD] = 9.85 [0.76] versus 5.94 [2.94]; β =5.07, 95% CI = 4.71–5.43), 18 months (mean [SD] = 9.88 [0.82] versus 6.18 [2.86]; β =4.82, 95% CI = 4.48–5.16), and 24 months (mean [SD] = 9.99 [0.47] versus 6.59 [3.24]; β =4.49, 95% CI = 4.13–4.86). See detailed results in Supplemental Digital Content 3, Table 3, https://links.lww.com/PSYMED/A868. Figure 4 in Supplemental Digital Content 4, https://links.lww.com/PSYMED/A869, illustrates the multilevel mixed-effects regression model of GSP effects on functioning using raw data (complete cases) adjusted for baseline employment, marital status, and ART adherence.
ART AdherenceMore GSP than GHE participants reported ≥95% adherence rates at 12 months (94% versus 86%; aOR = 7.01, 95% CI = 3.10– 18.81), 18 months (97% versus 84%; aOR = 58.14, 95% CI = 16.64–203.16), and 24 months (96% versus 88%; aOR = 20.88, 95% CI = 5.78–75.33). See detailed results in Supplemental Digital Content 3, Table 2, https://links.lww.com/PSYMED/A868. Figure 1 in Supplemental Digital Content 4, https://links.lww.com/PSYMED/A869, illustrates the multilevel mixed-effects regression model of GSP effects on ART adherence using raw data (complete cases) adjusted for baseline employment, marital status, and function scores.
Viral SuppressionThe proportion of study participants with viral suppression was comparable between the two groups 12 months after treatment (89% versus 84%; aOR = 1.08, 95% CI = 0.57–2.02). However, 24 months after treatment, the GSP group had a significantly greater proportion of participants with viral suppression compared with the GHE group (96% versus 88. %; aOR = 3.38, 95% CI = 1.02–11.02) See detailed results in Supplemental Digital Content 3, Table 2, https://links.lww.com/PSYMED/A868. Figure 2 in Supplemental Digital Content 4, https://links.lww.com/PSYMED/A869, illustrates the multilevel mixed-effects regression model of GSP effects on viral suppression using raw data (complete cases) adjusted for baseline employment, marital status, function scores, and ART adherence.
The Relationship Between Therapy Groups and Viral Suppression at 24 Months Through Sequential Changes in Depression and ART Adherence at 12 MonthsSequential mediation analyses indicated the indirect effects through sequential changes in depression and ART adherence at 12 months in the relationship between GSP and viral suppression at 24 months were small but significant (β = −0.039, 95% CI = −0.063 to −0.015). On addition of the indirect effects through depression in the relationship between therapy group and ART adherence, the total indirect effects through depression and ART adherence at 12 months (β = 1.396, 95% CI = 0.975–1.816) became large and significant indicating that the improvement in ART adherence through reduction in depression contributes greatly to the mediation effects through which GSP leads to viral suppression. The total effect of GSP on participants’ viral suppression at 24 months after treatment remained significant in this sequential model (β = 1.67, 95% CI = 0.69–2.35) although less than what we observed in the cross-sectional mediation model (β = 3.42, 95% CI = 2.69–4.15). Table 3 shows the detail of total and indirect effects of GSP through sequential changes in depression and ART adherence at 12 months on viral suppression at 24 months.
TABLE 3 - Indirect and Total Effects of Group Support Psychotherapy Through Depression and ART Adherence at 12 Months (T2) on Viral Suppression at 24 Months (T3) β SE Bootstrapped 95% CI p Intervention → depression (T2) → adherence (T3) Indirect effects through depression 1.38 0.022 0.943 to 1.807 <.001 Total effects 3.06 0.976 1.154 to 4.983 .002 Intervention →depression (T2) → viral suppression (T3) Indirect effects through depression −0.038 0.0114 −0.060 to −0.015 .001 Total effects 0.240 0.252 −0.252 to 0.735 .339 Intervention →adherence (T2) → viral suppression (T3) Indirect effects through adherence −0.0014 0.004 −0.01 to 0.006 .730 Total effects 0.277 0.250 −0.214 to 0.768 .269 Intervention→ depression (T2) → adherence (T2) → viral suppression (T3) Indirect effects through depression and adherence −0.039 0.012 −0.063 to −0.015 .001 Total indirect effects 1.396 0.214 0.975 to 1.816 <.001 Total effects 1.674 0.366 0.955 to 2.393 <.001ART = antiretroviral therapy; SE = standard error; CI = confidence interval.
This study examined the long-term effect of culturally sensitive GSP delivered by lay health workers compared with an active comparison, GHE, on depression and HIV treatment outcomes. The intervention had significant short-term effects on depression and functioning, which were sustained in the long term. These results were generally consistent with our prior study of GSP delivered by diploma-level mental health workers, which showed similar improvements of depression and functioning overtime (23). Studies demonstrating positive long-term effects of psychological interventions for depression are limited (49,50). Indeed, the literature has generally shown diminishing effects of psychological treatments for depression with time (51). The striking sustained reductions in depression speak to the potential utility of GSP and require replication in other low-resource settings.
The beneficial effects of GSP may be attributed to its active ingredients (emotional and social support, positive coping skills, and income-generating skills), which are potent buffers against depression. GSP allows participants to interact with one another as they execute their livelihood projects (30). Although participants no longer receive guidance from a trained LHW after the completion of GSP, they continue to receive social support from one another, which may buffer group members from developing depression in the long term (30). Furthermore, the stress-buffering model asserts that social support mitigates the relation between stressful life events and depression (52,53). It is plausible that increased social support, connections, and networks may mitigate the impact of various stressors and reduce depression (54).
The improvement in depression and functioning observed in GHE groups could be explained by therapeutic factors common to both interventions, such as a supportive environment, and therapeutic alliance, which generate positive feelings. However, because GHE lacks the active elements of GSP, such as opportunity to express emotions, and acquisition and practice of positive coping skills and livelihood skills, positive feelings generated might not be sustained.
In keeping with findings from similar studies of psychological interventions for HIV-related depression (20), our study showed that a reduction in depression was accompanied by improved ART adherence in the long term. Two years after the end of interventions, the proportion of those with self-reported ≥95% ART adherence had increased by almost 22% in the GSP group compared with only 7% in the control group. Some prior studies of cognitive-behavioral therapy integrated with adherence counseling for
留言 (0)