
記住我
Migraine is a prevalent, chronic, painful, and burdensome condition that can cause substantial impairment and disability.1–5 The goals of acute treatment are to achieve rapid and sustained freedom from pain, to restore functional ability, and to minimize the use of rescue medications.5 For patients with moderate-to-severe migraine, triptans are recommended as first-line acute therapy (when over the counter analgesics do not suffice), and are widely accepted as standard of care.5 However, a substantial portion of patients are contraindicated to, do not respond to, or cannot tolerate triptan therapy, and until recently there has been a substantial unmet need for these patients.6
Two gepants or calcitonin gene-related peptide (CGRP) receptor antagonists (rimegepant and ubrogepant), and 1 selective serotonin receptor agonist (lasmiditan) have recently been developed for use in the acute treatment of migraine. These therapies are currently recommended for use in adult patients with insufficient response to 2 or more triptans, or for those who experience intolerable side effects or have contraindications to triptans.5 A targeted literature review found that 15% to 25% of patients with migraine fulfill these requirements and may be eligible for rimegepant, ubrogepant or lasmiditan.7
These CGRP receptor antagonists reduce pain and inflammation and have fewer adverse events than older treatments due to their mechanism of action,8–10 and they have no apparent association with medication overuse headache.5Ubrogepant is currently approved by the US Food and Drug Administration (FDA) for the acute treatment of migraine in adults, and rimegepant is a dual-use therapy approved for both acute and preventive treatment.11,12 This dual-use indication of rimegepant, further differentiates it from standard of care therapies and other novel therapies.13,14
Lasmiditan, a selective 5-hydroxytryptamine 1F receptor agonist, has been found to inhibit the acute migraine pathway10,15 and reduce pain and disability.16,17 It is approved by the FDA for the acute treatment of migraine in adults,15 but contrary to the gepants, it has some potential to cause medication overuse headache, abuse, and impaired driving if taken within 8 hours of operating a vehicle.5
All 3 treatments demonstrated efficacy and safety in randomized, double-blind, placebo, controlled trials (RCTs).13,18–26 However, there are no trials that directly compare these treatments with each other.27,28 This makes clinical evidence-based decisions-making difficult.29 Decision-making can be guided by outcome measures that combine both clinical and statistical significance: the number needed to treat (NNT) and number needed to harm (NNH).29,30 These clinically intuitive measures link the effect-size observed in clinical trials to real-world outcomes (namely treatment success and adverse events).31 The combination of NNT and NNH provides a benefit-risk profile of treatments that provides useful information to clinicians. The objective of this study was to determine the NNT and NNH to develop benefit-risk profiles for rimegepant, ubrogepant, and lasmiditan based on a network meta-analysis (NMA) of published clinical trials.28
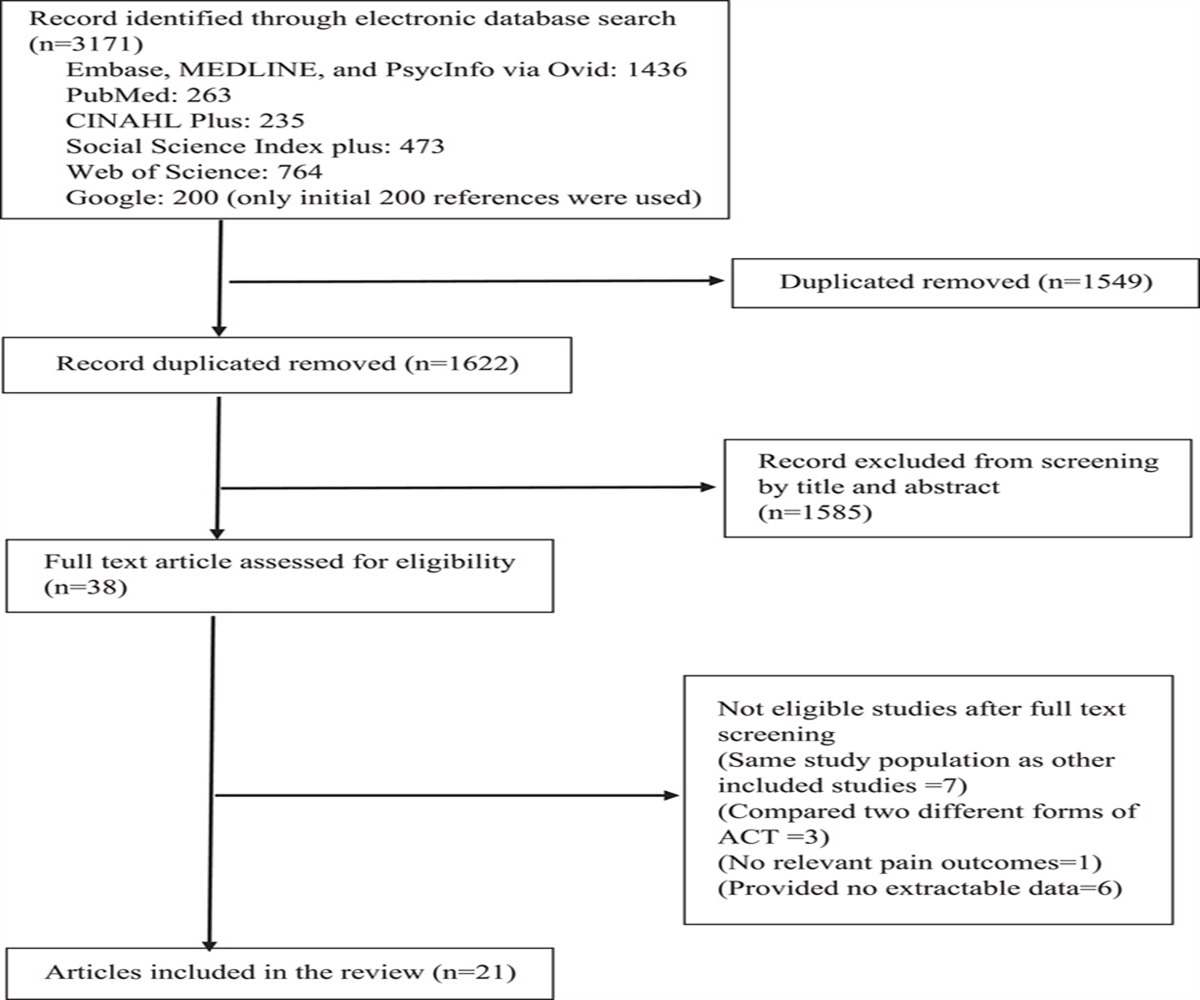
METHODS Data Sources, Searches, and Study SelectionA prespecified protocol and the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were used for a systematic literature review (SLR) of RCTs addressing the efficacy and safety of lasmiditan, rimegepant, and ubrogepant.32 The methods used for the SLR and NMA are detailed in a publication by Johnston et al.28 Briefly, Embase and MEDLINE were searched from inception to July 22, 2019, and hand searches were also conducted. Articles were included or excluded based on population, intervention, comparator, outcome, and study design (PICOS) criteria. The population of interest was adults with migraine who needed acute treatments other than first-line treatments such as NSAIDs or triptans. The interventions and comparators were lasmiditan (50, 100, 200 mg), rimegepant (75 mg), and ubrogepant (25, 50, 100 mg). Efficacy outcomes were pain relief and pain freedom at 2 hours, sustained pain relief and pain freedom from 2 to 24 hours, and freedom from most bothersome symptoms (MBS) at 2 hours. Safety outcomes were dizziness and nausea.
Pain freedom is defined as having no pain 2 hours after treatment, and sustained pain freedom refers to maintaining a pain free state without relapse or the use of rescue medications from 2 to 24 hours postdose. Pain relief is defined as improvement from moderate or severe pain before treatment is initiated, to mild or no pain after at a specific interval after treatment. Freedom from MBS is defined as no migraine associated symptoms such as nausea, phonophobia, photophobia, or vomiting. Pain freedom at 2 hours is recommended as a primary endpoint to measure treatment response in clinical trials, freedom from MBS is recommended as a co-primary endpoint, sustained pain freedom as a composite endpoint, and pain relief is recommended as a secondary endpoint to compare results of various clinical trials.33
RCTs were the only eligible study design. Titles, abstracts, and full text articles were reviewed by 2 independent reviewers, and the Cochrane Risk of Bias Tool was used by 1 reviewer to assess study quality.34 The RCTs identified in the SLR were used to indirectly compare the 3 interventions in an NMA.28
Statistical AnalysisRisk differences (and associated 95% credible intervals [CrIs]), or the incremental proportion of respondents achieving the outcome of interest across treatments, were derived for the efficacy and safety outcomes.28 NNT and NNH were calculated from the risk differences, and used to compare the risk-benefit profile for each acute treatment. NNT is defined as the number of patients (over and above the number who respond in the comparator arm) that need to be treated with the intervention to achieve an additional positive event. NNH is similar but refers to an additional negative (adverse) event relative to the reference treatment (placebo in this case).35,36 NNT and NNH were calculated as the reciprocal of the risk differences between the active interventions and placebo (ie, 1/(proportion achieving an event active treatment−proportion achieving an event placebo).29 Note that CrIs of nonstatistically significant estimates include a risk difference of zero (corresponding to equivalent risk). Due to computational challenges caused by dividing by zero, the upper and lower bounds of presented CrIs for these estimates are not interpretable.
A Bayesian framework was used to fit NMA models based on the NICE Decision Support Unit (DSU) guidelines.37JAGS (V4.3.0) and R (V3.6.1) were used to conduct the analyses. Models included a binomial likelihood incorporating a logit link, and were fixed-effect models.28 This study analyzed published, aggregate clinical trial data, therefore ethical clearance was not required.
RESULTS Search ResultsThe NMA included 5 RCTs conducted in a total of 10,060 patients. The RCTs evaluated the efficacy and safety of lasmiditan 50, 100, and 200 mg oral tablets, rimegepant 75 mg orally disintegrating tablets; and ubrogepant 25, 50, 100 mg oral tablets.13,23–26 The included studies were Study 303 for rimegepant (n=1466),13 ACHIEVE I (n=1672),23 and ACHIEVE II (n=1686)26 for ubrogepant, and SAMURAI (n=2231)25 and SPARTAN (n=3005)24 for lasmiditan.28
Study CharacteristicsAll trials were phase III, multicenter trials spanning 4 to 11 weeks and assessing the acute treatment of a single migraine attack. As summarized in Table 1, studies were well-balanced with regards to baseline patient characteristics. For additional details about trial characteristics, please refer to the original publications or the publication by Johnston et al.28
TABLE 1 - Comparison of Baseline Patient Characteristics Across Included Trials Trial Treatment N Female, n (%) Age, Mean (SD) White, n (%) Migraine With Aura, n (%) Migraines Per Month, Mean (SD) MBS—Nausea, n (%) MBS—Phonophobia MBS—Photophobia ACHIEVE I* Placebo 485 430 (88.7) 40.9 (11.7) 410 (84.5) NR NR 109 (22.4) 104 (21.5) 270 (55.7) Ubrogepant 50 mg 466 418 (89.7) 40.1 (11.7) 383 (82.2) NR NR 99 (21.3) 90 (19.4) 273 (58.6) Ubrogepant 100 mg 485 418 (86.2) 40.6 (12.0) 392 (80.8) NR NR 93 (19.2) 126 (25.9) 266 (54.9) ACHIEVE II* Placebo 499 442 (88.6) 41.7 (12.1) 399 (80) 113 (22.6) 4.6 (1.8) 305 (61.2) 405 (81.1) 442 (88.6) Ubrogepant 25 mg 478 431 (90.2) 41.6 (12.4) 399 (83.5) 128 (26.8) 4.8 (1.8) 312 (65.3) 388 (81.1) 438 (91.7) Ubrogepant 50 mg 488 444 (91.0) 41.2 (12.5) 398 (81.6) 106 (21.7) 4.4 (1.8) 312 (64.0) 393 (80.6) 442 (90.5) Rimegepant Study 303 Placebo 682 580 (85.0) 40.0 (11.9) 518 (76.0) 218 (32.0) 4.5 (1.8) 171 (25.0) 136 (20.0) 375 (55.0) Rimegepant 75 mg 669 569 (85.0) 40.3 (12.1) 495 (74.0) 187 (28.0) 4.6 (1.8) 147 (22.0) 127 (19.0) 395 (59.0) SAMURAI Placebo 617 525 (85.1) 42.4 (12.3) 479 (77.6) 194 (31.4) 5.1 (1.8) 146 (23.6) 131 (21.3) 340 (55.1) Lasmiditan 100 mg 630 512 (81.3) 42.2 (11.7) 471 (74.8) 205 (32.5) 5.1 (1.8) 154 (24.5) 157 (24.9) 318 (50.5) Lasmiditan 200 mg 609 515 (84.6) 41.4 (12.0) 450 (73.9) 195 (32.0) 5.3 (2.3) 149 (24.5) 122 (20.0) 338 (55.5) SPARTAN Placebo 645 545 (84.5) 42.6 (12.9) 516 (80.0) 244 (37.8) 5.5 (2.4) 152 (23.5) 142 (22.0) 320 (49.6) Lasmiditan 50 mg 654 554 (84.7) 42.8 (13.2) 524 (80.1) 226 (34.6) 5.2 (2.0) 149 (22.8) 127 (19.4) 326 (49.8) Lasmiditan 100 mg 635 539 (84.9) 43.4 (12.6) 509 (80.2) 238 (37.5) 5.3 (1.9) 136 (21.4) 131 (20.7) 330 (51.9) Lasmiditan 200 mg 649 536 (82.6) 41.8 (12.4) 522 (80.4) 229 (35.3) 5.3 (1.9) 128 (19.7) 135 (20.8) 330 (50.9)*Ns reported from safety population.
MBS indicates most bothersome symptom; NR, not reported.
Direct comparisons of the interventions were not available, but indirect comparisons were possible due to the placebo arm connecting all included RCTs in the network. As shown in the network diagram, the studies are connected by a common comparator, placebo, which allows for indirect treatment comparisons of relative efficacy and safety (Fig. 1).
 FIGURE 1:
FIGURE 1: Network diagram.
In Tables 2 and 3 the risk differences, NNT, NNH, and 95% CrIs of the efficacy and safety outcomes of interest are presented. NNT for pain freedom at 2 hours versus placebo was lowest for lasmiditan 200 mg (7; 95% Crl: 5, 9), followed by rimegepant 75 mg (8; 95% Crl: 5, 14) and ubrogepant 100 mg (9; 95% CrI: 6, 20). The lowest doses of lasmiditan and ubrogepant had the highest NNT for pain freedom at 2 hours versus placebo (15; 95% CrI: 9, 37 and 15; 95% CrI: 8, 52 respectively for lasmiditan 50 mg and ubrogepant 25 mg). The NNT for sustained pain freedom from 2 to 24 hours was lowest for rimegepant 75 mg (7; 95% Crl: 5, 12), followed by lasmiditan 200 mg (12; 95% CrI: 8, 18) and ubrogepant 100 mg (13; 95% CrI: 7, 33). Personographs are used to visualize the NNT across treatments for pain freedom at 2 hours and sustained pain freedom from 2 to 24 hours in Fig. 2.
TABLE 2 - NNT to Achieve Key Primary and Secondary Efficacy Outcomes (Lasmiditan, Ubrogepant, Rimegepant) Treatment Risk Difference (95% CrI) NNT (95% CrI) Pain freedom at 2 h LAS_50 6.6 (2.7, 11.1) 15 (9, 37) LAS_100 9.9 (6.3, 14.0) 10 (7, 16) LAS_200 15.1 (11.0, 19.6) 7 (5, 9) UBR_25 6.8 (1.8, 12.8) 15 (8, 52) UBR_50 8.1 (4.0, 12.9) 12 (8, 25) UBR_100 10.6 (4.9, 17.4) 9 (6, 20) RIM_75 12.9 (7.3, 19.5) 8 (5, 14) Sustained pain freedom, 2-24 h LAS_50 3.9 (1.0, 7.5) 26 (13, 95) LAS_100 4.9 (2.3, 8.2) 20 (12, 44) LAS_200 8.6 (5.4, 12.5) 12 (8, 18) UBR_25 4.0 (0.2, 9.1) 24 (10, 166) UBR_50 5.3 (2.1, 9.4) 19 (11, 49) UBR_100 7.6 (3.0, 13.5) 13 (7, 33) RIM_75 14.3 (8.3, 22.2) 7 (5, 12) Pain relief at 2 h LAS_50 11.4 (6.1, 16.4) 9 (6, 16) LAS_100 17.2 (13.2, 21.1) 6 (5, 8) LAS_200 17.3 (13.3, 21.1) 6 (5, 8) UBR_25 11.6 (5.4, 17.6) 9 (6, 18) UBR_50 13.2 (8.6, 17.7) 8 (6, 12) UBR_100 13.2 (7.0, 18.9) 8 (5, 14) RIM_75 16.0 (10.7, 20.9) 6 (5, 9) Sustained pain relief, 2-24 h UBR_25 12.4 (6.1, 19.1) 8 (5, 16) UBR_50 16.7 (11.7, 22.1) 6 (5, 9) UBR_100 18.5 (11.9, 25.3) 5 (4, 8) RIM_75 19.0 (13.5, 24.7) 5 (4, 7) Freedom from the MBS at 2 h LAS_50 6.6 (1.5, 12.1) 15 (8, 59) LAS_100 10.7 (6.4, 15.2) 9 (7, 16) LAS_200 12.8 (8.4, 17.4) 8 (6, 12) UBR_25 6.7 (0.8, 13.1) 15 (7, 74) UBR_50 11.4 (6.7, 16.3) 9 (6, 15) UBR_100 10.3 (4.5, 16.7) 10 (6, 22) RIM_75 8.6 (3.3, 14.2) 12 (7, 30)Bold font denotes statistically significant values at a 5% level of significance.
CrI indicates credible interval; LAS, lasmiditan; MBS, most bothersome symptom; NNT, number needed to treat; RIM, rimegepant; UBR, ubrogepant.
Bold font denotes statistically significant values at a 5% level of significance.
Italicized font denotes nonstatistically significant estimates, where the upper and lower bounds of presented CrIs are not interpretable.
CrI indicates credible interval; LAS, lasmiditan; NNH, number needed to harm; RIM, rimegepant; UBR, ubrogepant.
 FIGURE 2:
FIGURE 2: Number Needed to Treat for (A) pain freedom at 2 hours, (B) sustained pain freedom, 2 to 24 hours.
For pain relief at 2 hours, the lowest NNT was 6, which was the same for lasmiditan 100 mg (95% CrI: 5, 8), lasmiditan 200 mg (95% CrI: 5, 8), and rimegepant 75 mg (95% CrI: 5, 9). The NNTs for sustained pain relief from 2 to 24 hours ranged from 5 (95% Crl: 4, 7) for rimegepant 75 mg and 5 (95% Crl: 4, 8) for ubrogepant 100 mg to 8 (95% Crl: 5, 16) for ubrogepant 25 mg. Sustained pain relief from 2 to 24 hours was not reported in the lasmiditan studies. For freedom from MBS at 2 hours, lasmiditan 200 mg had the lowest NNT (8; 95% Crl: 6, 12) and ubrogepant 25 mg the highest (15; 95% Crl: 7, 74). All interventions showed positive and statistically significant results for all efficacy outcomes compared with placebo.
Ubrogepant 25 mg had the highest NNH (54; 95% Crl: −1332, 1379) for dizziness, and ubrogepant 50 mg the lowest (−84; 95% Crl: −1473, 1415); however, these estimates were not statistically significant. Rimegepant 75 mg and ubrogepant 50 mg showed nonstatistically significant point estimates that were better than placebo with regards to dizziness. For nausea, rimegepant 75 mg had the lowest statistically significant NNH at 24 (95% Crl: 4, 229), while ubrogepant 25 mg had the highest NNH at 99 (95% Crl: −2580, 2378) (not statistically significant).
DISCUSSIONLasmiditan, rimegepant, and ubrogepant are all more effective than placebo for the acute treatment of migraine, and all interventions have an acceptable safety profile. The NNT to achieve immediate and sustained pain relief and pain freedom was lower for rimegepant than for all doses of lasmiditan and ubrogepant, with the exception of pain freedom at 2 hours for lasmiditan 200 mg.
NNT to achieve sustained pain relief from 2 to 24 hours was lowest for rimegepant 75 mg and ubrogepant 100 mg and highest for ubrogepant 25 mg. Rimegepant had the lowest NNT to achieve sustained pain freedom from 2 to 24 hours, while lasmiditan 50 mg had the highest NNT for this outcome. When considering safety outcomes, NNH for dizziness and nausea was highest for ubrogepant 25 mg (where rimegepant 75 mg and ubrogepant 50 mg had negative NNTs for dizziness), whereas lasmiditan 200 mg had the lowest NNH for dizziness and rimegepant had the lowest NNH for nausea.
Migraine is a highly individualized disease—the burden of disease varies substantially from person to person, and even within individuals the frequency and severity of migraine attacks fluctuate over time, and in response to certain triggers or life events.38 Therefore, the choice of pharmacological treatment depends on a variety of factors, including patient disease characteristics, patient preference, treatment history, comorbidities, and concomitant medication.5 NNT and NNH are clinically relevant measures, that can optimize clinical decision making and tailor decisions for individual’s needs (eg, by balancing the likelihood of treatment benefit with avoidance of adverse events).31 NNT combines clinical and statistical significance, and may therefore be of interest to clinicians who treat patients with migraine, particularly in the current treatment paradigm where novel treatments are being incorporated into everyday practice.31
These metrics have been used to characterize efficacy and safety in other migraine therapies, for example, a Cochrane review reported a NNT of 6.1 for sumatriptan 50 mg for freedom from pain at 2 hours,39 and 9.5 for sustained freedom from pain at 24 hours postdose.40 These findings are most similar to the 200 mg dose of lasmiditan for freedom from pain at 2 hours, whereas the NNT for rimegepant was lower at 7 for sustained pain freedom from 2 to 24 hours in the current study. Dizziness was reported as an adverse event of sumatriptan, and NNH for dizziness/vertigo was 49 (95% confidence interval: 31, 110) for sumatriptan 50 mg versus placebo (not calculated for nausea).39,40 This is most similar to the NNH for dizziness for the ubrogepant 25 mg dose.
Strengths of this study are that the NMA was based on a connected network of CGRP-antagonist RCTs that were well-balanced with regards to patient characteristics. NMAs combine direct and indirect evidence, to show the relative value or advantages of interventions that have not been compared directly in head-to-head trials. This also allows the treatments to be ranked for each outcome. NMAs provide cross-validation between trial estimates and an increase of statistical power where there are multiple comparisons per connection.
A limitation is that the studies that were included in the NMA only evaluated the treatments for a single migraine attack.29 Therefore, the long-term effects and treatment consistency are still unknown.41,42 In addition, clinical trials for the gepants had some exclusions for patients with cardiovascular disease, raising concerns about whether these treatments could fulfill the unmet need for patients with cardiovascular contraindications to triptans.42 Additional safety data is also needed for lasmiditan in patients with cardiovascular disease.41
CONCLUSIONSThe benefit-risk profiles of lasmiditan, rimegepant, and ubrogepant may improve clinical decision-making in the absence of direct head-to-head comparison trials. Future data from long-term studies and direct comparison of these treatments in head-to-head trials, and including standard of care treatments, would provide more concrete evidence for decision-making.41–43
CLINICAL IMPLICATIONS Novel acute treatments for migraine (lasmiditan, rimegepant, and ubrogepant) are currently recommended for patients with insufficient response, intolerable side effects, or contraindication to triptans. While these treatments have all demonstrated efficacy and safety in RCTs, they have not been compared head-to-head. Risk-benefit profiles were developed based on a NMA of published clinical trials; risk differences were used to calculate the NNT for key efficacy endpoints and NNH for adverse events. The NNT to achieve immediate (2 h) and sustained (2 to 24 h) pain relief and pain freedom was lower for rimegepant than for all doses of lasmiditan and ubrogepant, with the exception of pain freedom at 2 hours for lasmiditan 200 mg. When considering safety outcomes, NNH for dizziness and nausea was highest for ubrogepant 25 mg (where rimegepant 75 mg and ubrogepant 50 mg had negative NNTs for dizziness), whereas lasmiditan 200 mg had the lowest NNH for dizziness and rimegepant had the lowest NNH for nausea. The benefit-risk profiles of lasmiditan, rimegepant, and ubrogepant may improve clinical decision-making in the absence of direct head-to-head comparison trials. REFERENCES
留言 (0)