
記住我








Fine-needle aspiration (FNA) biopsy of a thyroid nodule is a mini-invasive diagnostic procedure used to confirm or exclude the malignancy of the nodule. Nodular disease is characterized by the disordered growth of thyroid cells often associated to the gradual development of fibrosis, areas of hemorrhage, or lymphocyte infiltration; it affects about 3% to 7% of adults who undergo objective examination.1
Current guidelines on the diagnosis and management of thyroid nodules2,3 recommend that FNA biopsy be carried out on capsular or paratracheal nodular lesions, those suspected of lymph-node or extrathyroidal involvement, and those in patients with a positive personal or family history of thyroid carcinoma or with consistent clinical symptoms (dysphonia); moreover, the nodules must present marked hypoecogenicity, lobulated irregular margins, anomalous vascularization, and calcifications, in addition to having a diameter of more than 10 mm.
Complications of FNA procedures are extremely rare. Those described in the literature are the following: pain at the site of intervention, infections, swelling of the neck, and the formation of small hematomas inside the gland, which are spontaneously reabsorbed within a few days.2 Particular caution should be exercised, however, in patients on anticoagulant therapy.3,4 Indeed, in a study of 593 patients who underwent FNA, hematomas were documented in 2 of the 144 patients who were on anticoagulant therapy, whereas, in the 449 patients who were not taking anticoagulants, 4 episodes of bleeding were observed.5
An even rarer complication is that of massive hemorrhage associated to the rapid onset of dyspnea due to deviation and compression of the trachea and requiring emergency surgical decompression.6–14 Moreover, cases of death after FNA are practically unknown in the literature.15,16
Here, we present the case of a woman affected by multinodular goiter who underwent diagnostic FNA biopsy of a thyroid nodule. After the procedure, she suffered a massive hemorrhage of the thyroidal and perithyroidal tissues, which caused cyanosis and worsening dyspnea; she died 6 hours later.
CASE REPORT Case HistoryA 78-year-old woman, who was obese (body mass index, 33.4 kg/m2) and affected by multinodular goiter, underwent medical examinations, including thyroid echography, which revealed an increase in the size of some nodules. The endocrinologist suggested that an FNA biopsy be taken of a nodule that presented also inhomogeneous ultrasound appearance and internal vascularization.
During the FNA procedure, which was performed under ultrasound guidance, no problems arose. About 30 minutes after the end of the procedure, the patient, who was not taking antiplatelet/anticoagulant drugs, left the outpatient clinic and went to lunch. During her meal, the woman began to feel discomfort in her neck. Once back home, she took an analgesic and lay down to rest. After about 2 hours, however, the woman began to suffer from swelling of the neck, dysphonia, and worsening dyspnea. The general practitioner was alerted, and the woman was promptly taken to the emergency department; although resuscitation maneuvers (cardiopulmonary resuscitation, tracheal intubation, central venous cannulation, and advanced medication administration) were carried out for about 40 minutes, the patient was pronounced dead 6 hours after the FNA procedure.
Autopsy and Histological FindingsThe public prosecutor ordered an autopsy to ascertain the cause of death and to investigate any hypothesis of professional liability on the part of the doctor who had performed the FNA. External examination revealed a large swelling, of soft consistency, in the anterior cervical region, leakage of blood from the mouth, and the marks of needle puncture on the right wrist and in the fold of the left elbow. The rest of the external examination was unremarkable.
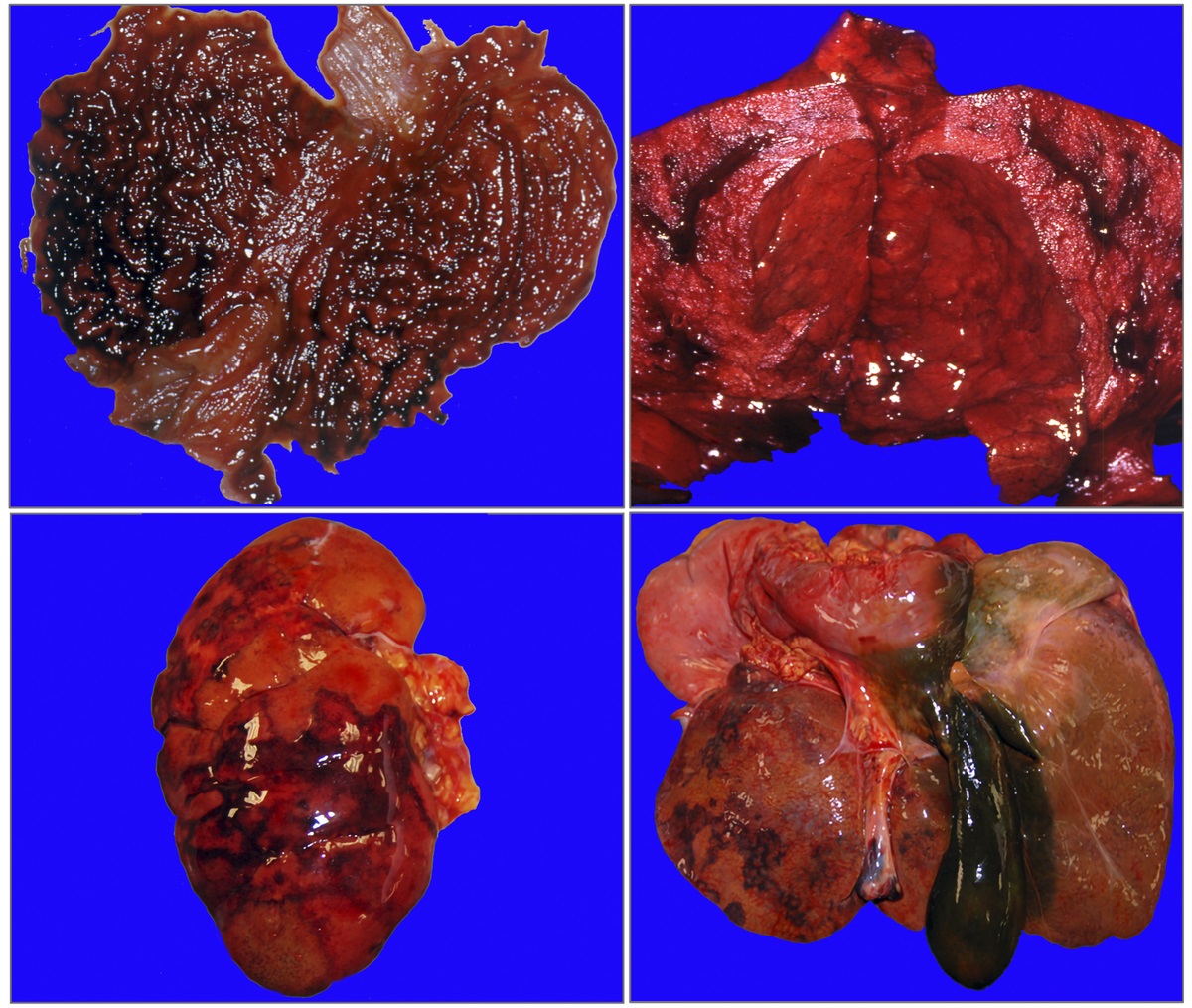
On section, a massive hematoma within the neck muscles and subcutaneous tissue of the supraclavicular region, especially on the right, was noted. At the right side of the suprasternal notch, at the base of the neck, an abundant collection of blood was found (Fig. 1).
 FIGURE 1:
FIGURE 1: Massive hemorrhagic infarct involving the neck muscles and subcutaneous tissue of the supraclavicular region, especially on the right.
The trachea presented blood leakage on compression, and coagulated blood was found along its entire length; the macroscopic architecture of the thyroid was completely disrupted by the hemorrhage. The lungs, which were congested and edematous, leaked pinkish foam when pressed, whereas the remaining visceral organs were markedly anemic but unremarkable. The heart weighted 400 g; the coronary arteries were elastic, and there were no signs of atherosclerosis.
After fixation in formalin, sampling of the organs of the neck was carried out. During this operation, a 3 × 15 cm area of hemorrhagic infiltration was observed at the level of the supraglottic plane, in the right lateral region of the esophagus (Fig. 2A). Posterior to the course of the trachea, a large quantity of coagulated blood was seen, whereas the right jugular vein presented an interruption of a few millimeters along the vertical axis (Fig. 2B). Eight samples were taken, one of which included the vein at its presumed point of rupture, whereas the others consisted of sections of the neck region affected by the hemorrhagic infarct.
 FIGURE 2:
FIGURE 2: Organs of the neck after fixation in formalin. A, Area of hemorrhagic infiltration at the level of the supraglottic plane, surrounding the right lateral region of the esophagus. B, Interruption of a few millimeters along the vertical axis of the right jugular vein.
Histological analysis revealed a thyroid architecture characterized by multiple colloidocystic nodes and a structure disrupted by a fibrosclerotic process constituted by hyaline connective tissue arranged in bundles that tended to segment the gland. In addition, a granulomatous process with foreign body-type giant cells, reactive to colloid extravasation and microhemorrhages, was seen (Fig. 3A). The overall picture was characterized by ubiquitous recent hemorrhages, with more marked hemorrhagic extravasations in the perithyroid tissues and in the lobules of adipose tissue (Fig. 3B); in this setting, 3 medium-caliber veins with lacerated walls, apposition of fibrin meshes, and reactive lymphogranulocytic infiltrate were found (Fig. 3C).
 FIGURE 3:
FIGURE 3: Histological findings. A, Granulomatous process with foreign body-type giant cells, reactive to colloid extravasation and microhemorrhages in the thyroid gland (hematoxylin and eosin [H&E], ×20). B, Marked hemorrhagic extravasations in the thyroid tissues (H&E, ×20). C, A medium-caliber vein of the perithyroid tissues with lacerated wall (H&E, ×20). D, Laceration of small thickness of the jugular vein, in the absence of inflammatory reaction (H&E, ×20).
With regard to the full-thickness lesion of the jugular vein, histology revealed a laceration of small thickness (2 mm) in the absence of inflammatory reaction (granulocytic or lymphocytic elements in the vessel wall); moreover, the vein appeared dystrophic, with marked thinning and loss of the normal smooth muscle component of the wall (Fig. 3D).
The cause of death was attributed to the compression of the vascular and nervous structures of the neck and obstruction of the upper airways, secondary to abundant dissecting hemorrhages in the thyroidal and perithyroidal tissues due to vascular lesions of the adjacent veins after FNA of the thyroid nodule.
DISCUSSIONHere, we report a rare case of death due to massive hemorrhage of the thyroid parenchyma and of the perithyroidal tissues after an FNA procedure.
Multinodular nontoxic goiter is a chronic disease characterized by enlargement of the thyroid in the absence of neoplastic alterations. The enlarged gland typically presents macroscopic irregular nodules. Histological examination of the nodules reveals flattened or cuboid epithelial lining cells and, occasionally, papillae that protrude into the follicular lumen. The frequent presence of hemosiderin deposits and cholesterol granulomas is indicative of a previous hemorrhage. Single follicles or clusters of follicles separated by dense fibrosis with dystrophic calcifications may also be observed. Hemorrhage and chronic inflammation are frequent.17,18
The development of a massive hemorrhage capable of determining compression of the vascular-nervous structures of the neck and obstruction of the upper airways, threatening the life of the patient, is an extremely rare complication of needle aspiration procedures of nodules in a context of a multinodular goiter. Indeed, although the thyroid is a richly vascularized organ, bleeding of the parenchyma and the surrounding tissues is a sporadic event and is generally self-limiting, causing only mild symptoms. Fatal cases are extremely rare.
A thorough review of the literature reveals that only 12 cases of thyroid hemorrhages after needle aspiration procedures have been described (Table 1). This complication proved fatal in only 2 cases.15,16
TABLE 1 - Cases of Thyroid Hemorrhages After Needle Aspiration Procedures According to the Literature Authors Sex; Age, y Thyroid Disease Symptoms Reported After FNA Type of Complication Anticoagulant or Antiplatelet Drugs Death of the Patient Case 1 Katagiri et al6 F, 47 Nodule Neck swelling, pain, dyspnea Massive hematoma No No Case 2 Noordzij and Goto7 F, 60 Lymphocytic thyroiditis Dyspnea, pain, ecchymosis, neck swelling 4 × 5 × 7 cmSpecifically, Kakiuchi et al15 reported the case of a 68-year-old woman who underwent FNA to investigate the nature of a mass involving the left lobe of the thyroid. After the procedure, she returned home and was found dead about 6.5 hours later. Autopsy revealed a large laryngeal edema and a massive hemorrhage on the anterior and lateral surfaces of the gland. Death was attributed to obstruction of the upper airways due to the massive perithyroidal hemorrhage.
The second fatal case was reported by Strachan et al.16 This involved a 79-year-old woman who was affected by a voluminous thyroid nodule that extended to the upper mediastinum and which was in contact with the anterior wall of the trachea. After an FNA procedure, she died before reaching the emergency department. Autopsy indicated an acute hemorrhage originating inside the thyroid gland as the cause of death.
Both cases involved elderly women (older than 65 years): this population, because of an increased venous fragility, is at greater risk of developing fatal vascular complications during routine procedures.
In the remaining cases reported in the literature, bleeding was less severe, and prompt surgical decompression was able to save the patients' lives.
Two possible mechanisms responsible for bleeding have been described: anomalous vascularization of a multinodular goiter, which increases the fragility of the vessels and hence the probability of their rupture, and the creation of arteriovenous shunts in the setting of thyroid parenchyma with disrupted architecture.19,20
In the case reported here, disruption of the parenchymal structure was observed. Indeed, histological examinations revealed a colloid nodular goiter with severe fibrosclerotic sequelae secondary to previous thyroiditis. This condition had weakened the thyroid vessels, which appeared dystrophic. A minimal trauma, caused by the needle aspiration procedure, was therefore sufficient to trigger a progressive intrathyroidal bleeding.
Moreover, the histological findings corroborated this hypothesis. The hemorrhagic infarct, in the thyroidal and perithyroidal areas and in the vicinity of the adjacent lacerated veins, displayed margination and the interposition of reactive lymphogranulocytic elements, which typically appear 5 to 6 hours after a hemorrhagic trauma. This time lapse is therefore consistent with the circumstantial data, which attest that the FNA procedure was carried out at 11.00 am and that the patient died at 5.30 pm.
Thus, within a few hours, the hemorrhage swelled the volume of the gland, causing external compression of the vascular-nervous structures of the neck and acute obstruction of the upper airways, leading to respiratory insufficiency.
With regard to the jugular vein lesion observed during autopsy examination, histological examination would be more consistent with the injury to not have occurred synchronous with the rupture of the thyroid vessels, given the absence of intralesional and perilesional granulocytic inflammatory reaction (as was documented in the thyroid tissues). A jugular vein lesion occurred during FNA of thyroid nodule would determine an inflammatory reaction with apposition of fibrin meshes and reactive lymphogranulocytic infiltrate. Furthermore, the woman was taken to the emergency department where resuscitation maneuvers, including central venous cannulation, were carried out.
These elements indicate that the laceration of the jugular vein occurred during resuscitation maneuvers carried out in limine vitae.
The present article describes an extremely rare complication of a needle aspiration procedure; indeed, only 2 other fatal cases are reported in the literature.
In this particularly complex case, only careful and complete investigation of the circumstantial data and autopsy and histological findings enabled the correct diagnosis to be made. The fixation and histological examination of the specimen affected by the hemorrhage proved to be of fundamental importance. In addition to identifying the site of bleeding, they enabled a differential diagnosis to be made between lesions caused by needle aspiration and those caused by resuscitation maneuvers.
The case reported is not only of medicolegal interest but also of clinical relevance. First of all, operators who perform needle aspiration procedures should always inform their patients of the hemorrhagic risk, albeit minimal. Equally important are the knowledge and application of the guidelines, to prevent the occurrence of complications. These precautions are also important in terms of avoiding medicolegal disputes. Particular caution should be exercised when dealing with subjects who present risk factors. In such cases, it is advisable to carry out detailed preoperative tests, prolong the observation period after the procedure, and, at the moment of discharge, carefully instruct the patient as to the alarm symptoms of a possible ongoing hemorrhage. Prompt recognition of hemorrhagic complications increases the possibility of therapeutic intervention and, therefore, of survival.6,9,12,13
From the medicolegal standpoint, the case did not have penal repercussions, in that the public prosecutor deemed that the operator who performed the FNA was not liable to penal prosecution, on the grounds that there was no clear evidence of culpable conduct. In the civil court, however, the patient's family members were awarded damages, given that the causal link between the procedure and the patient's death was established within the terms of the preponderant scientific evidence.
REFERENCES 1. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association guidelines task force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26:1–133. 2. Polyzos SA, Anastasilakis AD. Clinical complications following thyroid fine-needle biopsy: a systematic review. Clin Endocrinol (Oxf). 2009;71:157–165. 3. Gharib H, Papini E, Garber JR, et al. American Association of Clinical Endocrinologists, American College of Endocrinology, and Associazione Medici Endocrinologi medical guidelines for clinical practice for the diagnosis and management of thyroid nodules — 2016 update. Endocr Pract. 2016;22:622–639. 4. Lyle MA, Dean DS. Ultrasound-guided fine-needle aspiration biopsy of thyroid nodules in patients taking novel oral anticoagulants. Thyroid. 2015;25:373–376. 5. Abu-Yousef MM, Larson JH, Kuehn DM, et al. Safety of ultrasound-guided fine needle aspiration biopsy of neck lesions in patients taking antithrombotic/anticoagulant medications. Ultrasound Q. 2011;27:157–159. 6. Katagiri H, Lefor AK, Kubota T, et al. Massive hematoma after fine-needle aspiration of the thyroid. Surgery. 2016;160:245–246. 7. Noordzij JP, Goto MM. Airway compromise caused by hematoma after thyroid fine-needle aspiration. Am J Otolaryngol. 2005;26:398–399. 8. Yoshida M, Miyata M, Maeda H, et al. Massive thyroid hematoma developing after a fine-needle aspiration biopsy. Intern Med. 2012;51:3223–3224. 9. Donatini G, Masoni T. Is fine-needle aspiration cytology for thyroid nodules a routine and safe procedure? A series of emergency cervicotomies following FNAC. Langenbecks Arch Surg. 2010;395:873–876. 10. Park MH, Yoon JH. Anterior neck hematoma causing airway compression following fine needle aspiration cytology of the thyroid nodule: a case report. Acta Cytol. 2009;53:86–88. 11. Lee YS, Baek HS, Park TS, et al. Bilateral intrathyroidal hemorrhage after fine needle aspiration completely resolved by compression without thyroidectomy. Endocrine. 2013;43:460–461. 12. Roh JL. Intrathyroid hemorrhage and acute upper airway obstruction after fine needle aspiration of the thyroid gland. Laryngoscope. 2006;116:154–156. 13. Hor T, Lahiri SW. Bilateral thyroid hematomas after fine-needle aspiration causing acute airway obstruction. Thyroid. 2008;18:567–569. 14. Donatini G, Masoni T, Ricci V, et al. Acute respiratory distress following fine needle aspiration of thyroid nodule: case report and review of the literature. G Chir. 2010;31:387–389. 15. Kakiuchi Y, Idota N, Nakamura M, et al. A fatal case of cervical hemorrhage after fine needle aspiration and core needle biopsy of the thyroid gland. Am J Forensic Med Pathol. 2015;36:207–209. 16. Strachan MW, Dalvi M, Ainsworth R, et al. Fatal haemorrhage following fine needle aspiration of the thyroid. J R Coll Physicians Edinb. 2016;46:166–167. 17. De Groot LJ, Jameson JL. Endocrinology Adult and Pediatric : The Thyroid Gland. 6th ed. Philadelphia, PA: Elsevier Saunders; 2013. 18. Fagin JA, Mitsiades N. Molecular pathology of thyroid cancer: diagnostic and clinical implications. Best Pract Res Clin Endocrinol Metab. 2008;22:955–969. 19. Lee JK, Lee DH, Cho SW, et al. Acute airway obstruction by spontaneous hemorrhage into thyroid nodule. Indian J Otolaryngol Head Neck Surg. 2011;63:387–389. 20. Dell'Aquila M, De Matteis A, Bolino G, et al. Death due to external compression of the trachea in a patient with multinodular hemorrhagic goiter. Forensic Sci Med Pathol. 2019;15:509–512.
留言 (0)