NETs are rare neoplasms. They arise from cells of the diffuse endocrine system, which are mainly dispersed throughout the gastrointestinal, pancreatic, and respiratory tracts. Neuroendocrine cells are derived from the epithelial and neuroectodermal cells. NETs are positive by silver staining and express synaptophysin, neuron-specific enolase, and chromogranin A.
The worldwide prevalence and incidence of NETs have recently increased. The incidence of NET was 1.09 per 100,000 people in 1973 and increased to 6.98 per 100,000 people in 2012 in the United States [2]. Based on data derived from the National Cancer Registry in Japan, the total number of patients treated for gastro-entero-pancreatic NENs (GEP-NENs) in 2016 was 6735, and the age-adjusted overall incidence was 3.53 per 100,000 people. The age-adjusted incidence of each primary NEN is presented in Table 1 [3]. Approximately half of the GEP-NENs involved the rectum (1.82 per 100,000 people), followed by the pancreas (0.697 per 100,000 people). The incidence of ileal NEN is 1% of the total GEP-NENs [3].
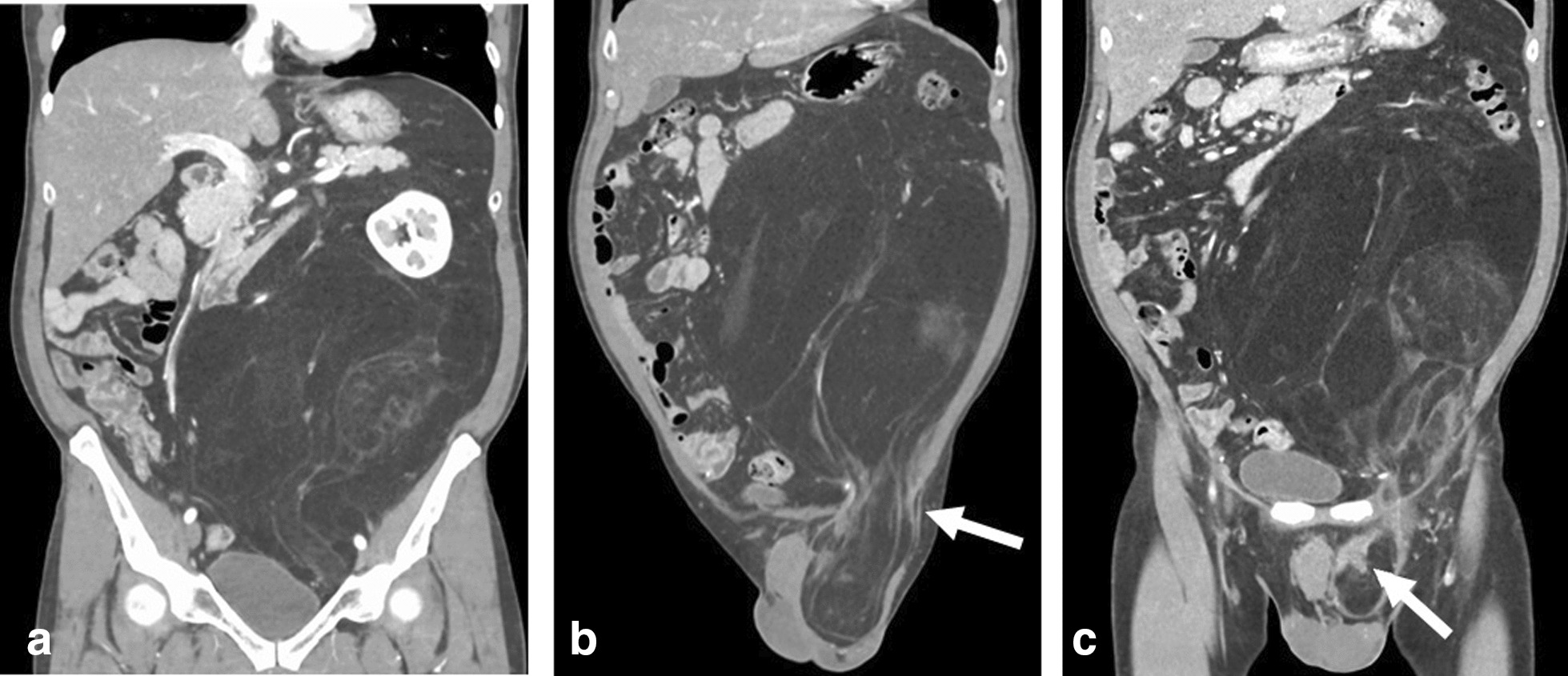
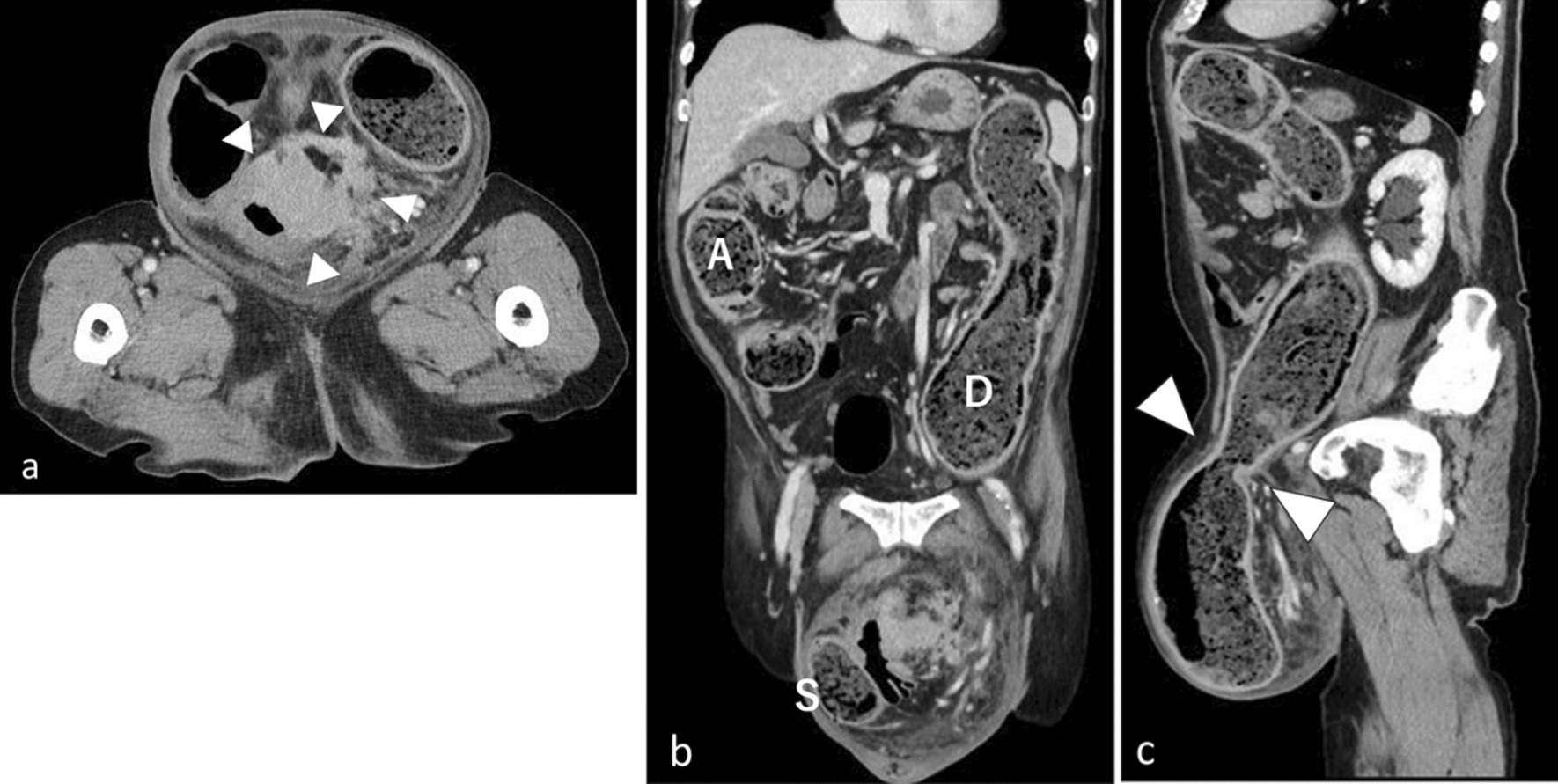
True primary solid tumors of the mesentery include NETs, fibromatoses, neurofibromas, teratomas, germ cell tumors, and primary neoplasms composed of smooth muscle, blood vessels, or fat [4]. Primary mesenteric NETs are very unusual, although secondary mesenteric involvement is common, reported as 40–80%, respectively [5]. We present an extremely rare case of an ileal mesenteric NET with benign or low-grade malignant characteristics on preoperative FDG-PET.
NETs are a subtype of NENs that are defined as epithelial neoplasms with predominant neuroendocrine differentiation. Because neuroendocrine cells are widely distributed throughout the body, NENs can arise in various locations, including the respiratory and digestive systems [6]. The WHO previously proposed a classification scheme for digestive NENs that divides them into three categories based on mitotic count and Ki-67 labeling index value: NET G1, NET G2, and NEC [7]. In particular, a mitotic count of < 2 per 10 high-power fields (HPFs) and/or Ki-67 index of < 3% corresponds to NET G1, a mitotic count of 2–20 per 10 HPFs and/or Ki-67 index of 3–20% corresponds to NET G2, and a mitotic count of > 20 per 10 HPFs and/or Ki-67 index of > 20% corresponds to NEC. In 2019, the WHO revised its former classification scheme and established a well-differentiated subtype of NET G3 from cases previously classified as NEC (Table 2) [8].
Table 2 Classification and grading criteria for NEN (2019) [8]The current gold standard for functional imaging of NETs is somatostatin receptor scintigraphy (SRS) with 111In-diethylenetriaminepentaacetic acid-octreotide [9]. Which is a proliferation marker reflecting the prognosis. FDG-PET is the most widely used nuclear medicine technique for functional imaging of cancer. However, FDG-PET has never been routinely used for imaging NETs, and its diagnostic performance remains unclear. The overall sensitivity rates of diagnostic imaging for NETs were reported to be 89% and 58% for SRS and FDG-PET, respectively [10]. FDG-PET is not sensitive in detecting low-grade primary gastrointestinal NETs. Tumor differentiation can be used to guide the selection of nuclear imaging modalities for staging of gastrointestinal and pancreatic NETs. SRS appears to be more sensitive than FDG-PET for well-differentiated NETs, whereas FDG-PET demonstrates superior sensitivity for poorly differentiated NETs [11]. The tumor presented by us was diagnosed as a benign or low-grade malignant tumor on preoperative FDG-PET. Based on the final pathological diagnosis, the tumor was diagnosed as NET G2. If SRS could have been performed preoperatively in our case, it may have been diagnosed as an NET with strong accumulation at the tumor site. When a neoplastic lesion of the small intestine or mesentery is diagnosed, it is possible that the tumor is an NET, but it is often difficult to confirm the tumor diagnosis preoperatively. However, if FDG-PET and SRS can be performed simultaneously at the time of tumor diagnosis, it may be possible to diagnose NETs, including GRADE.
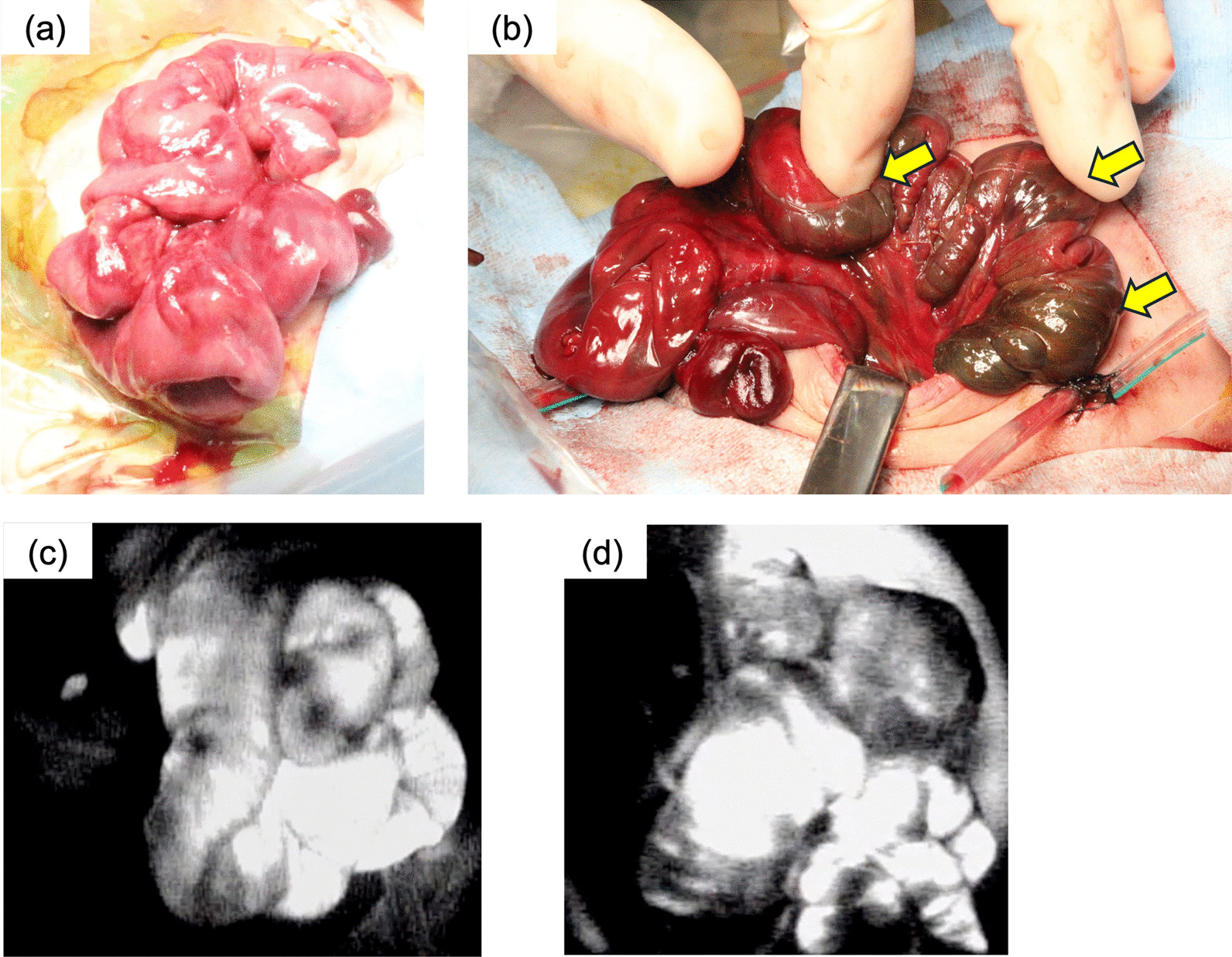
Surgery is the mainstay treatment for localized gastrointestinal NETs, and may be curative in cases of R0 resection. To our knowledge, only 10 cases of primary small intestinal mesenteric NETs have been reported in the literature [5, 12,13,14,15,16,17,18,19,20] (Table 3). Of the 11 patients, including this patient, there were five men and six women, with a mean age of 61.3 (range, 48–74) years. Tumors were localized in the jejunal mesentery in six cases and in the ileal mesentery in five cases. As far as the grade classification of these 11 cases is known, there were no highly malignant G3 cases. Of these 11 surgical procedures, tumor resection was performed in five cases, and small bowel resection including the mesentery, was performed in six cases. In addition, one of the five tumor resections was laparoscopic. Regarding the surgical approach, we initially considered observing the lesion using laparoscopy. However, due to the irregular shape of the tumor and the fact that the tumor was invading the mesentery, we ultimately opted for laparotomy.
Table 3 Resected cases of primary small intestinal mesenteric NETs [5, 12,13,14,15,16,17,18,19,20]







留言 (0)