
記住我
Pancreatic cancer is the fourth leading cause of cancer-related mortality in the United States and, in 2022, it is estimated that 62,210 new cases of pancreatic cancer will be diagnosed in the US resulting in 49,830 deaths.1 Over the next decade, it is predicted that the incidence of pancreatic cancer will rise to approximately 88,000 cases per year, and that mortality will increase to approximately 63,000 deaths per year, making PDAC the second leading cause of cancer death in the United States by 2030.2
The PRODIGE 4/ACCORD 11 trial that compared FOLFIRINOX to gemcitabine as first-line treatment for metastatic pancreatic cancer established FOLFIRINOX as the new standard of care for patients with advanced pancreatic cancer. The median overall survival of 11.1 months in the FOLFIRINOX group was nearly double that of the 6.8 months reported in the gemcitabine group.3 The objective response rate was also higher [31.6% vs. 9.4%]. Despite these benefits, grade 3/4 toxicities were increased with FOLFIRINOX including neutropenia [18.7% vs. 45.7%], febrile neutropenia [0.6% vs. 5.4%], diarrhea [1.2% vs. 12.7%], and neuropathy [0% vs. 9%].3
Nab-paclitaxel [Abraxane] is an albumin-bound cremophor-free formulation of paclitaxel, which in combination with gemcitabine, has been shown to improve overall survival compared with gemcitabine alone in patients with metastatic pancreatic cancer.4 Irinotecan, an agent that is hydrolyzed to SN-38, an inhibitor of topoisomerase I, lacks significant activity in pancreatic cancer as a single agent and the combination of irinotecan plus gemcitabine failed to improve survival compared with gemcitabine alone.5 Although irinotecan may be synergistic when used in combination with oxaliplatin and fluorouracil, its overall contribution to FOLFIRINOX might be at the cost of significant toxicity.
The optimal management of locally advanced and borderline resectable pancreatic cancer remains controversial with no internationally embraced standard approach. The trend has been toward management with neoadjuvant or upfront chemotherapy in an effort to increase changes of margin-negative resection and early control of occult micrometastatic disease. That said, patients with locally advanced disease often do not have a sufficient cytoreductive response to initial therapy to allow for subsequent R0 resection. In 2015, the results of a single-arm study evaluating FOLFIRINOX in the locally advanced and borderline resectable setting were released. In total, 77 patients were enrolled, and the authors reported a response rate of approximately 28%; however, only 27 [35%] patients underwent surgical resection. The one-year progression-free survival [PFS] was 59%.6 Philip et al reported results from treatment with combination gemcitabine and nab-paclitaxel in the locally advanced setting. Sixty-two [58%] of 107 enrolled patients completed induction treatment and 17 [16%] underwent surgery; of these, 7 achieved a R0 resection, 9 had a R1 resection. The median PFS was 10.9 months and median overall survival was 18.8 months.7 Another single-arm phase II study published in 2018 of 48 patients with untreated borderline resectable PDAC treated between August 2012 and August 2016 with neoadjuvant FOLFIRINOX followed by radiation reported more robust responses. In this study, patients were restaged after 8 cycles of FOLFIRINOX and received either short-course chemoradiotherapy [5 Gy×5 with protons] with capecitabine if radiographic resolution of vascular involvement was needed, or long-course chemoradiotherapy with capecitabine or fluorouracil if there was persistent vascular involvement. Of the 48 patients, 56% had short-course chemoradiotherapy; 35% received long-course chemoradiotherapy, and R0 resection was achieved in 31 of 48 patients [65%; 95% CI, 49-78%].8 To date, despite this promising data, there has been no published phase III randomized control trial data to guide treatment for locally advanced and borderline resectable pancreatic cancer.
The Brown University Oncology Research Group [BrUOG] previously reported a phase I study in which irinotecan was removed from FOLFIRINOX and substituted with nab-paclitaxel [FOLFOX-A].9 This study included patients with newly diagnosed advanced, unresectable pancreatic adenocarcinoma. The maximum tolerated dose of nab-paclitaxel, when combined with FOLFOX, was 150 mg/m2. Neuropathy was the most significant toxicity reported. Grade 3 neuropathy developed in 2 of the first 6 patients at 10 and 11 cycles of FOLFOX-A. After an amendment to reduce oxaliplatin to 68 mg/m2 [20% reduction] if grade 2 neuropathy developed, no additional patients developed grade 3 neurotoxicity. Twenty-one of 35 patients [60%] had a partial response and the median overall survival for patients with metastatic disease was 15 months.
BrUOG-292 and BrUOG-318 are two open-label concurrently run prospective single-arm phase II studies that evaluated FOLFOX-A in patients with metastatic and locally advanced/borderline resectable pancreatic cancer respectively.
MATERIALS AND METHODS Study DesignBetween 6/2014 and 11/2019, patients with either metastatic or locally advanced/borderline resectable pancreatic cancer were enrolled onto BrUOG-292 and BrUOG-318, respectively. The primary end point of both studies was overall response rate. The secondary end points were PFS, overall survival, and toxicities. All patients provided written informed consent. The studies were carried out in accordance with the Declaration of Helsinki. The study protocols were approved by the institutional review board and was registered at clinicaltrials.gov NCT02080221[BrUOG 292] and NCT02578732 [BrUOG 318].
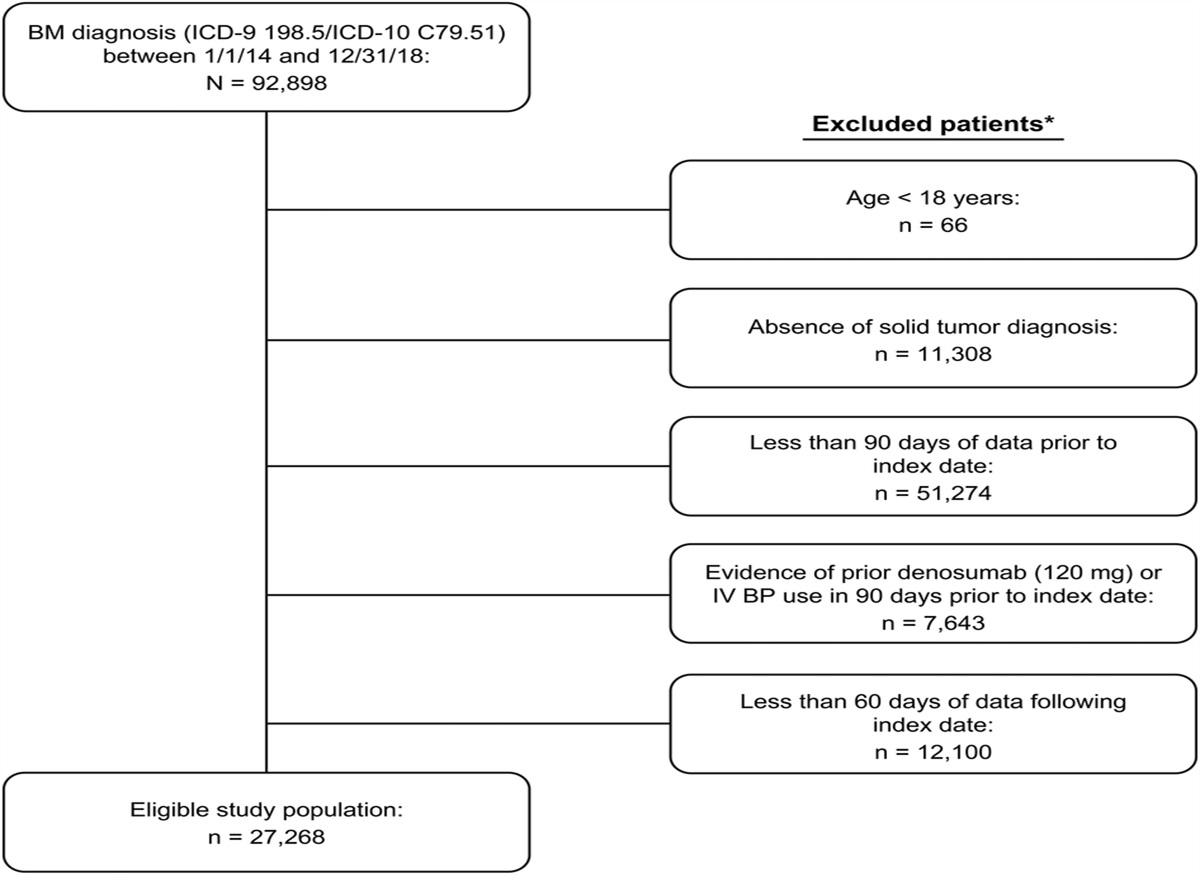
EligibilityPatients were eligible if they had histologically proven adenocarcinoma of the pancreas and were treatment-naive. Patients with metastatic pancreatic ductal adenocarcinoma [PDAC] were enrolled on BrUOG-292 whereas patients with locally advanced or borderline resectable pancreatic cancer were enrolled on BrUOG-318. Borderline resectable and locally advanced[unresectable] status was determined based on NCCN guidelines and tumor board recommendations. The patient were required to have an Eastern Cooperative Oncology Group [ECOG] performance status of 0 or 1 and age of ≥18 years. An absolute neutrophil count >1500/mm3, platelet count >100,000/mm3, hemoglobin >9.0 g/dL, aspartate transaminase and alanine transaminase ≤2.5×ULN [for patients with liver metastases, AST&ALT ≤5×ULN], total bilirubin ≤1.5×ULN, alkaline phosphatase ≤2.5xupper limit normal [unless bone metastases were present and in the absence of liver metastasis], creatinine ≤1.5 mg/dL, and creatinine clearance >60 mL/min was necessary before enrollment. Other exclusion criteria included prior chemotherapy for pancreatic cancer, or major surgery within 3 weeks of the start of study treatment. Patients with a plastic stent or any pre-existing neuropathy [grade 1 or higher] were not eligible; patients with metal stents were allowed. A computer tomography scan [CT scan] of the chest and abdomen were required within 28 days of study enrollment.
TreatmentTreatment consisted of 5-FU, 1200 mg/m2/d as a continuous intravenous (IV) infusion over 46 hours, leucovorin, 400 mg/m2 IV over 2 hours for 1 day, and oxaliplatin, 85 mg/m2 IV over 2 hours for 1 day, and nab-paclitaxel, 150 mg/m2 IV over 30 minutes for 1 day. One cycle was 14 days. Myeloid growth factors could be administered as prophylaxis against neutropenia or febrile neutropenia at the discretion of the treating physician. Patients could receive a maximum of up to 12 cycles. Patients with locally advanced or borderline resectable disease could stop treatment after 6 cycles and receive radiation therapy and/or surgical exploration if feasible.
Evaluation and Follow-upBefore treatment initiation, all patients underwent a complete medical evaluation that included a history and physical examination, routine laboratory studies, carbohydrate antigen 19-9 [CA19-9], vital signs, body weight, height, and evaluation of ECOG performance status. Abdominal and chest computed tomography, magnetic resonance imaging, or Positron emission tomography were performed within 6 weeks before treatment initiation. computed tomography scans were repeated every 3 months during treatment as per institutional standard of care. During the treatment period, patients were followed every 2 weeks with clinical and laboratory evaluations. All adverse events [AEs] and toxicities were recorded according to the National Cancer Institute’s Common Terminology Criteria for Adverse Events [NCI-CTCAE, version 4.0].
Statistical AnalysisOverall response rate [ORR] was defined as proportion of patients who achieved a complete or partial response as their best overall response based on international criteria proposed in the Revised Response Evaluation Criteria in Solid Tumors [RECIST] Guideline version 1.1.10 overall survival [OS] was calculated from the date of initiation of FOLFOX-A to the date of death. PFS was calculated from the date of initiation of treatment to the date of disease progression. The outcomes of OS, PFS, and Response rate were calculated with the corresponding 95% CI. OS and PFS were estimated using the Kaplan-Meier method. All statistical analyses were performed using STAT.
In BrUOG 292, we hypothesized that FOLFOX-A would increase median survival by 3 months compared with standard gemcitabine with the null hypothesis being FOLFOX-A will perform less than or equal than gemcitabine using historical control. Survival with gemcitabine alone is approximately 6.5 months and we assumed that FOLFOX-A would improve survival up to 9.5 months. A sample size of approximately 50 patients provided a power [1-β] of 75% to reject the null hypothesis with a type I error probability [α] of 0.2.
An ORR of 31.6% was reported with use of FOLFIRINOX in the phase III PRODIGE 4/ACCORD 11 in patients with mPDAC and ORR of approximately 28% was reported in a single-arm study of FOLFIRINOX in locally advanced and borderline resectable PDAC published in 2015.3,6 In BrUOG 318, we hypothesized that FOLFOX-A would achieve a response rate of at least 40%. A response rate of ≤20% would not be considered worthy of future evaluation. Specifically, the hypothesis to be tested was: H0: P≤p0 versus H1: P≥p1 [where the true response probability is denoted as p, an uninteresting level of probability is denoted as p0 and the desirable target level as p1]: A Simon’s optimal two-stage design was used in BrUOG 318. The first 24 evaluable patients were to be assessed for response in the first stage. The trial would be terminated early for futility if 5 or fewer responses are observed in these patients, and it would be concluded that the true response rate was unlikely to be >40%. If at least 6 responses were observed, accrual would continue in the second stage, until a total of 60 evaluable patients were enrolled. If 18 or more of the 60 had a response, it would be concluded that the treatment regimen had sufficient activity to warrant further investigation. The characteristics of this study design were as follows: the probability of type I error [one-sided alpha] was 0.04 and power of 93%. The Brown University Oncology Research Group Data Safety Monitoring Committee voted to close accrual after completion of the first stage of BrUOG 318 owing to slow accrual and to facilitate the combined reporting of BrUOG 292 and BrUOG 318.
RESULTS Patient CharacteristicsBetween 6/2014 and 11/2019, 50 patients with metastatic pancreatic cancer and 28 patients with locally advanced/borderline resectable disease were enrolled on BrUOG-292 and BrUOG-318 at Lifespan Cancer Institute at Rhode Island Hospital and The Miriam Hospital in Providence, Rhode Island, respectively. Two patients did not receive study treatment and were not assessable. The characteristics of the 76 assessable patients are shown in Table 1. The median age of participants were 66, 64% were male, and 66% had an ECOG performance status of 0. All patients had ductal adenocarcinoma histology and 66% involved the pancreatic head. In BrUOG 292, the liver was the most common site of metastatic disease.
TABLE 1 - Baseline Characteristics of Patients with Locally Advanced/Borderline (BrUOG 318), Unresectable, and Metastatic (BrUOG 292) Pancreatic Adenocarcinoma Treated with FOLFOX-A Characteristics BrUOG 318 (N=28) BrUOG 292 (N=48) Age Median (yr) 65 66 Sex, No. (%) Male 16 (57) 31 (62) Female 12 (43) 19 (38) Race White 21 (75) 45 (90) Black/unknown 3/4 5 (10) ECOG PS, No. (%) 0 21 (75) 30 (60) 1 7 (25) 20 (40) CA19-9, μ/mL Median (range) 292 (4-27,237) 1206 (1-724,035) Disease extent, no. (%) Locally advanced 14 (50) 0 Borderline 14 (50) 0 Metastatic 0 50 Site of primary tumor, no. (%) Head 16 (57) 34 (68) Other 12 (43) 16 (32) Site of metastasis, no. (%) Liver NA 37 (74) Lung NA 6 (12) Lymph node NA 6 (12) Omentum NA 4 (8)ECOG indicate Eastern Cooperative Oncology Group; BrUOG, Brown University Oncology Group; PS, performance status; yr, years old.
The median number of cycles administered on BrUOG-292 was 8 [range 1-12]. Patients with stable or ongoing disease response after completion of FOLFOX-A generally received maintenance 5-FU infusion or gemcitabine. On BrUOG-292, 30 [60%] patients required dose reductions after a median of 3 cycles, largely owing to fatigue [14/30], diarrhea, thrombocytopenia, and neurotoxicity.
The median number of cycles received on BrUOG 318 was 6 [range 1-10]. Fourteen patients enrolled in BrUOG-318 received concurrent chemoradiation with capecitabine after achieving stable disease or partial response as specified by protocol after 6 cycles. On BrUOG-318, 11 [39%] patients required dose reductions and dose delays mostly secondary to fatigue, diarrhea, thrombocytopenia, and neurotoxicity. After treatment, 4 patients underwent surgical resection with negative margins [3 borderline resectable and 1 locally advanced].
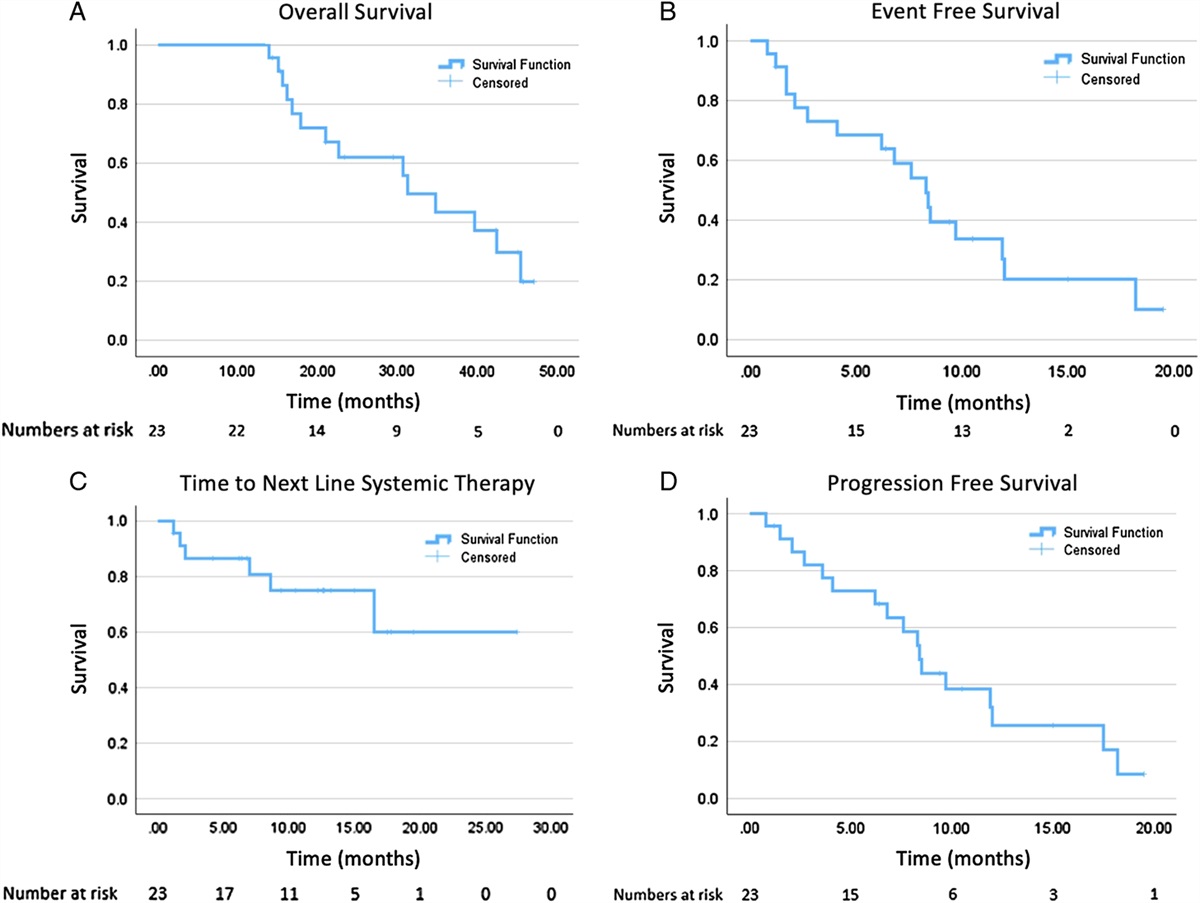
The median follow-up for BrUOG-292 was 40 months [95% CI 23-NR]. Of the 48 evaluable patients, a complete radiographic response was confirmed in 2 patients [4%], partial response in 12 patients [25%], stable disease in 12 patients [25%], and progressive disease in 22 patients [56%] [Table 2]. The estimated 1-year PFS rate was 21% [95% CI 11-33%], with a median PFS of 5 months [95% CI 3-7; Fig. 1A, Table 2]. The estimated 1-year OS rate was 42% [95% CI 28-55%], with a median OS of 11 months [95% CI 8-17; Fig. 1B, Table 2].
TABLE 2 - Efficacy Results of Patients with Metastatic (BrUOG 292) and Locally Advanced/Borderline Resectable (BrUOG 318) Pancreatic Cancer Treated with FOLFOX-A Objective response rate BrUOG 292 BrUOG 318 Patient population Metastatic disease Locally advanced and borderline resectable Medial follow up (mo) 40 32 Number of patients (evaluable) 48 28 Complete response, No. (%) 2 (4) 0 (0) Partial response, No. (%) 12 (25) 12 (43) Stable disease, No. (%) 12 (25) 12 (43) Progressive disease, No. (%) 22 (56) 4 (14) Overall survival, mo, median (95% CI) 11 (8-14) 22 (14-NR) Progression-free survival, mo, median (95% CI) 5 (3-7) 11 (6-18)BrUOG indicates Brown University Oncology Group.
 FIGURE 1:
FIGURE 1: A, Progression-free survival (PFS) of 48 patients with metastatic pancreatic cancer treated with FOLFOX A on BrUOG 292. The median PFS was 5 months (95% CI, 3-7). B, Overall survival (OS) of 48 patients with metastatic advanced pancreatic cancer treated with FOLFOX-A on BrUOG 292 . The median OS was 11 months (95% CI, 8-17). C, PFS of 28 patients with locally advanced/borderline resectable pancreatic cancer FOLFOX A on BrUOG 318. The median PFS were 11 months (95% CI, 6-18). D, OS of 28 patients with locally advanced/borderline resectable pancreatic cancer FOLFOX A on BrUOG-318. The median OS were 22 months (95% CI, 14-NR).
For BrUOG-318, the median follow-up was 32 months [95% CI 25-45]. Of the 28 evaluable patients, a partial response was confirmed in 13 patients [46%], stable disease in 11 patients [40%], and progressive disease in 4 patients [10%], respectively, Table 2. The estimated 36-month PFS rate was 15% [4-32], with a median PFS of 11 months [95% CI 6-18; Fig. 1C, Table 2]. The estimated 36 month OS rate was 37% [95% CI, 18-56], with a median OS of 22 months [95% CI, 14-NR; Fig. 1D, Table 2].
Treatment-related ToxicityIn general, FOLFOX-A was well tolerated in this population. Treatment-related AEs among patients enrolled in BrUOG-292 are listed in Table 3. Most AEs were grade 1 or 2. Grade ≥3 toxicities were uncommon with fatigue, diarrhea, and neutropenia being most common; seen in ≥10% of patients. Serious adverse event [SAEs] were reported in 13 treated patients and thought to be related to disease progression in the majority of cases. Treatment related SAEs included thrombocytopenia, pneumonitis, nausea, vomiting, and diarrhea.
TABLE 3 - Adverse Events of Patients with Metastatic (BrUOG 292) and Locally Advanced/Borderling Resectable (BrUOG 319) Pancreatic Cancer Treated with FOLFOX-A Table BrUOG 292 BrUOG 318 Adverse events Total No. (%) ≥Grade 3 No. (%) Grade 4 No. (%) Total No. (%) ≥Grade 3 No. (%) Grade 4 No. (%) Hematologic toxicities Neutropenia 21 (42) 12 (24) 2 (4) 18 (64) 5 (18) 2 (7) Thrombocytopenia 36 (72) 1 (2) 1 (2) 16 (57) 1 (3) — Anemia 30 (60) 2 (4) — 18 (64) — — Nonhematologic toxicities Peripheral sensory neuropathy 33 (66) 1 (2) — 24 (85) 1 (3) — Diarrhea 20 (40) 5 (10) — 14 (50) 6 (21) — Anorexia 13 (26) 3 (6) — 10 (35) — Vomiting 12 (24) 3 (6) — 4 (14) 1 (3) — Nausea 21 (42) 4 (8) — 12 (42) 3 (10) — Fatigue 36 (72) 20 (40) — 25 (89) 11 (39) — Mucositis (oral) 6 (12) — — 4 (11) 1 (3) — Arthralgia 2 (4) — — 1 (3) 1 (3) — Weight loss 30 (60) 2 (4) — 18 (64) 1 (3) — Elevated AST/ALT 22 (44) 2 (4) — 11 (39) 1 (3) — Elevated alkaline phosphatase 37 (74) 3 (6) — 20 (71) — —ALT indicates alanine aminotransferase; AST, aspartate aminotransferase; BrUOG, Brown University Oncology Research Group.
In BrUOG-318, hematologic and gastrointestinal toxicities were frequently seen but mostly grade 1 or 2. Fatigue was common and reached grade ≥3 in 39% of patients. Nausea, diarrhea, and neutropenia also reached grade ≥3 and were seen in more than 10% of patients [Table 3]. SAEs were reported in 7 treated patients and, as in BrUOG-292, predominantly related to disease progression. Treatment related SAEs included diarrhea and possible cardiomyopathy. There were no treatment-related deaths.
DISCUSSIONIn BrUOG 292 and 318, FOLFOX-A was an effective first-line treatment option for patients with metastatic, locally advanced, and borderline resectable pancreatic adenocarcinoma with an ECOG performance status of 0-1. PFS, response rate, and median overall survival among metastatic patients were comparable to FOLFIRINOX.
When the initial PRODIGE4/ACCORD11 trial was published in 2012, the striking improvement in outcomes, both OS and PFS between FOLFIRINOX versus gemcitabine alone were unprecedented in their magnitude. This study established FOLFIRINOX as the standard first-line therapy of metastatic pancreatic cancer in fit patients and it remains so today. The primary limitation of this regimen is tolerance. Even in the young, fit, predominantly male population without biliary obstruction enrolled in this trial, >70% required dose modification. The safety profile of FOLFOX-A may be more favorable than FOLFIRINOX; the majority of AEs were grade 1 or 2 and the most common treatment-related grade ≥3 AEs occurring in more than 10% of patients were fatigue, diarrhea, and neutropenia. Grade 3 neuropathy was surprisingly uncommon that was likely because of close monitoring and prompt dose reduction if any grade II symptoms developed. The median number of cycles completed on BrUOG-292 and BrUOG-318 were 8 and 6, respectively. In BrUOG 318, treatment was often stopped after 6 cycles [as defined per protocol] so patients could receive concurrent radiation with capecitabine. Four patients [14%] on BrUOG-318 were able to undergo R0 resection surgery.
The true benefit of FOLFIRNOX may be more prominent in less advanced stages of disease. The phase III PRODIGE24-ACCORD24/CCTG-PA6 trial evaluating adjuvant mFOLFIRINOX versus gemcitabine in 493 patients with resected PDAC demonstrated a median DFS of 21.6 months vs 12.8 months and median OS of 54.4 months and 35.0 months favoring FOLFIRINOX.11 Increasingly, chemotherapy has been administered neoadjuvantly in both borderline and locally advanced PDAC owing to potential advantages of facilitating margin negative resection [R0] and early systemic control by treating micrometastasis. A meta-analysis published by Janssen et al, in 2019, analyzed 24 studies involving 313 patients with borderline resectable PDAC treated with FOLFIRINOX. The resection rate was 67.8% with an R0-resection rate of 83.9%; median OS was 22.2 months.12 In ESPAC-5F, a four-arm, prospective, multicenter randomized phase II trial, 90 patients with borderline resectable PDAC were randomized to receive neoadjuvant gemcitabine/capecitabine versus FOLFIRINOX versus CRT versus immediate surgery. Primary end points were recruitment rate and resection rate [R1/R0]; secondary end points included OS and toxicity. The resection rates were 62% for immediate surgery and 55% for neoadjuvant therapy; R0 resection rate was 15% and 23% [P=0.721].13 Although the difference in R0 resection rate was not different between the two arms, there was a statistically significant survival benefit—the 1-year survival rate of 40% versus 70% favored neoadjuvant therapy. Although the resections rates were not as high amongst patients receiving neoadjuvant FOLFOX-A in BrUOG 318, the median OS of 22 months is comparable.
Acknowledging that this was a small, single-institution study and that these findings are difficult to compare directly with those of large randomized phase III trials or larger multicenter phase II trials, FOLFOX-A seems to have relatively less gastrointestinal toxicities when compared with FOLFIRINOX with similar efficacy in the metastatic setting. Although the rates of R0 resection were inferior compared with the historical data from similar phase II trials utilizing FOLFIRINOX neoadjuvantly in borderline resectable and locally advanced PDAC, the median OS was 22 months despite only 4 patients [14%] ultimately undergoing R0 resection. Currently, there are two ongoing trials [PRIMUS-001 and PRIMUS-002] comparing FOLFOX-A to the standard regimen of gemcitabine and nab-paclitaxel in pancreatic cancer. PRIMUS 001 is a multicenter, randomized, open-label, phase II trial comparing FOLFOX-A with gemcitabine and nab-paclitaxel in patients with metastatic pancreatic cancer. PRIMUS 002 compares FOLFOX-A with gemcitabine and nab-paclitaxel in the neoadjuvant setting. Both studies include integrated biomarker assessments of DNA damage response.14
ACKNOWLEDGMENTThis study was supported by Celgene.
REFERENCES 1. Siegel RL, Miller KD, Fuchs HE, et al. Cancer statistics, 2022. CA: A Cancer J Clin. 2022;72:7–33. 2. Rahib L, Smith BD, Aizenberg R, et al. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res. 2014;74:2913–2921. 3. Conroy T, Desseigne F, Ychou M, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. New Engl J Med. 2011;364:1817–1825. 4. Von Hoff DD, Goldstein D, Renschler MF. Albumin-bound paclitaxel plus gemcitabine in pancreatic cancer. New Engl J Med. 2014;370:479–480. 5. Rocha Lima CM, Sherman CA, Brescia FJ, et al. Irinotecan/gemcitabine combination chemotherapy in pancreatic cancer. Oncology. 2001;15:46–51. 6. Marthey L, Sa-Cunha A, Blanc JF, et al. FOLFIRINOX for locally advanced pancreatic adenocarcinoma: results of an AGEO multicenter prospective observational cohort. Ann Surg Oncol. 2015;22:295–301. 7. Philip PA, Lacy J, Portales F, et al. Nab-paclitaxel plus gemcitabine in patients with locally advanced pancreatic cancer (LAPACT): a multicentre, open-label phase 2 study. Lancet Gastroenterol Hepatol. 2020;5:285–294. 8. Murphy JE, Wo JY, Ryan DP, et al. Total neoadjuvant therapy with FOLFIRINOX followed by individualized chemoradiotherapy for borderline resectable pancreatic adenocarcinoma: a phase 2 clinical trial. JAMA Oncol. 2018;4:963–969. 9. Safran H, Charpentier KP, Perez K, et al. FOLFOX+Nab-paclitaxel (FOLFOX-A) for advanced pancreatic cancer: A Brown University Oncology Research Group Phase I Study. Am J Clin Oncol. 2016;39:619–622. 10. Eisenhauer EA, Therasse P, Bogaerts J, et al. New response evaluation criteria in solid tumours: revised RECIST guideline (version 1.1). Eur J Cancer. 2009;45:228–247. 11. Conroy T, Hammel P, Hebbar M, et al. FOLFIRINOX or gemcitabine as adjuvant therapy for pancreatic cancer. New Engl J Med. 2018;379:2395–2406. 12. Janssen QP, Buettner S, Suker M, et al. Neoadjuvant FOLFIRINOX in patients with borderline resectable pancreatic cancer: a systematic review and patient-level meta-analysis. J Natl Cancer Inst. 2019;111:782–794. 13. Ghaneh P, Palmer DH, Cicconi S, et al. ESPAC-5F: four-arm, prospective, multicenter, international randomized phase II trial of immediate surgery compared with neoadjuvant gemcitabine plus capecitabine (GEMCAP) or FOLFIRINOX or chemoradiotherapy (CRT) in patients with borderline resectable pancreatic cancer. J Clin Oncol. 2020;38:4505-. 14. Graham JS, Valle JW, Evans TRJ, et al. PRIMUS-001: an adaptive phase II study of FOLFOX-A (FOLFOX and nab-paclitaxel) versus AG (nab-paclitaxel and gemcitabine) in patients with metastatic pancreatic cancer, with integrated biomarker evaluation (ISRCTN75002153) – Part of Precision-Panc. J Clin Oncol. 2018;36:TPS4158–TPS4158.
留言 (0)