
記住我
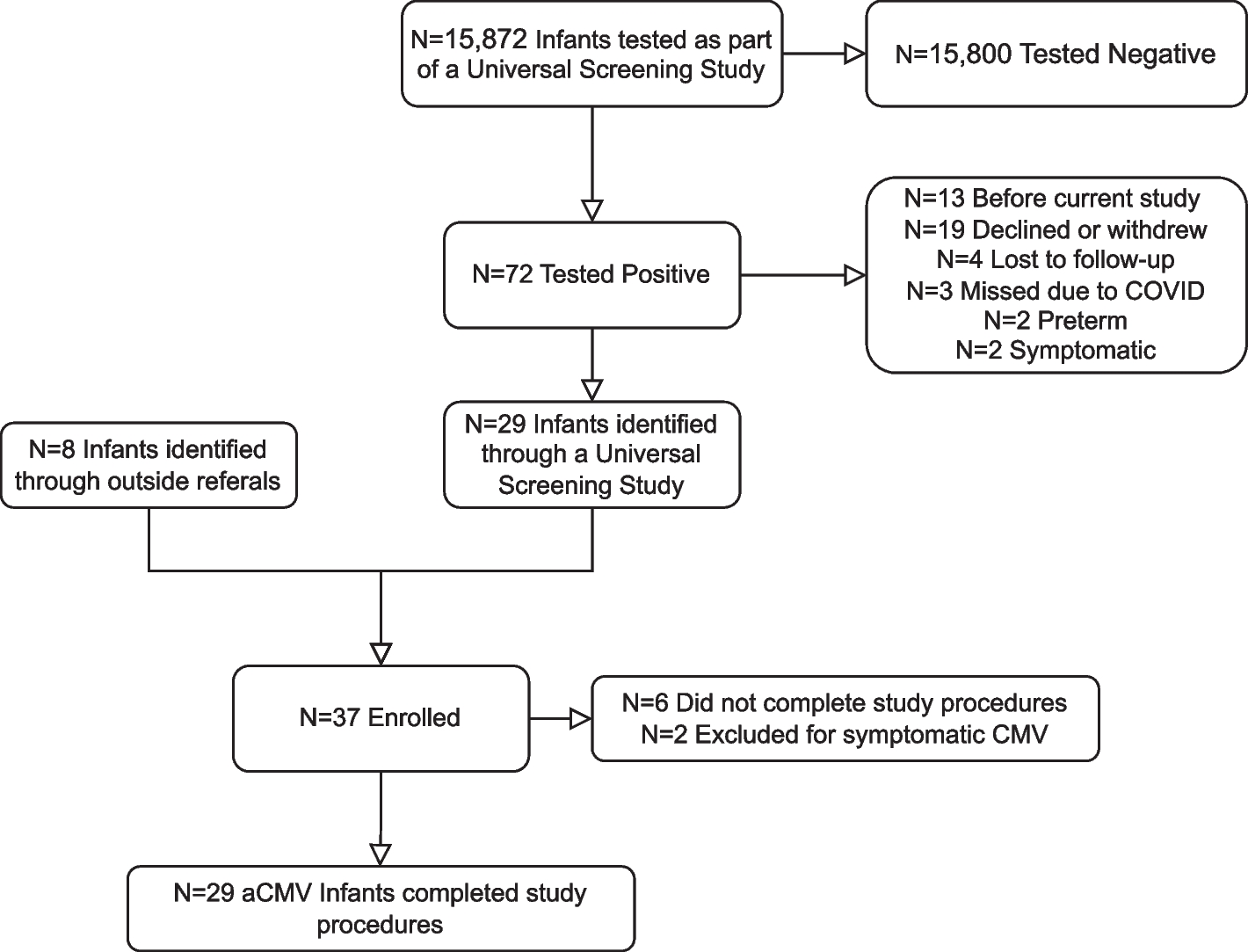
This prospective case-control cohort study comprised two waves of data collection. A total of 162 24–33-month-old toddlers were recruited from parenting websites or local pediatric clinics in northern Taiwan (Fig. 1). We assessed their expressive vocabulary using the Mandarin Chinese version of the Words and Sentences Forms of the MacArthur-Bates Communicative Developmental Inventories Toddler Form (MCDI-T) [25] to screen toddlers with delayed expressive language. Out of 162 toddlers, 65 were included in the data collection at time 1. The matching criteria for LT toddlers included chronological age (within 1 month of birthdate), native language (Mandarin), birth order, and sex. Due to the strict matching criteria, 91 TLD participants who did not match LT participants on the criteria mentioned above and who completed only the MCDI-T were excluded from the final data analysis. Furthermore, one toddler diagnosed with autism spectrum disorder (ASD) and five toddlers with cognitive delays were also excluded. Among the 65 participants who completed both waves of data collection, 32 toddlers were in the LT group, and 33 were in the TLD group. The inclusion criteria for LT toddlers were the same as those in other studies [15, 26,27,28]. In particular, for the LT group, word production performance should be at or below the 15th percentile on the MCDI-T, whereas that for the TLD toddlers should be at or above the 25th percentile. Behavior problems of children were collected via parental reports [29]. One LT toddler and two TLD toddlers did not participate in subsequent follow-up (time 2) and were excluded. For the final data analysis of this longitudinal study, 31 LT toddlers (22 boys) and 31 TLD toddlers (22 boys) completed the data collection. The mean TLD and LT participant ages for the two data collection points were 27.59 (SD = 2.46) and 27.54 (SD = 2.60) months at time 1 and 50.88 (SD = 2.46) and 51.37 (SD = 2.53) months at time 2, respectively.
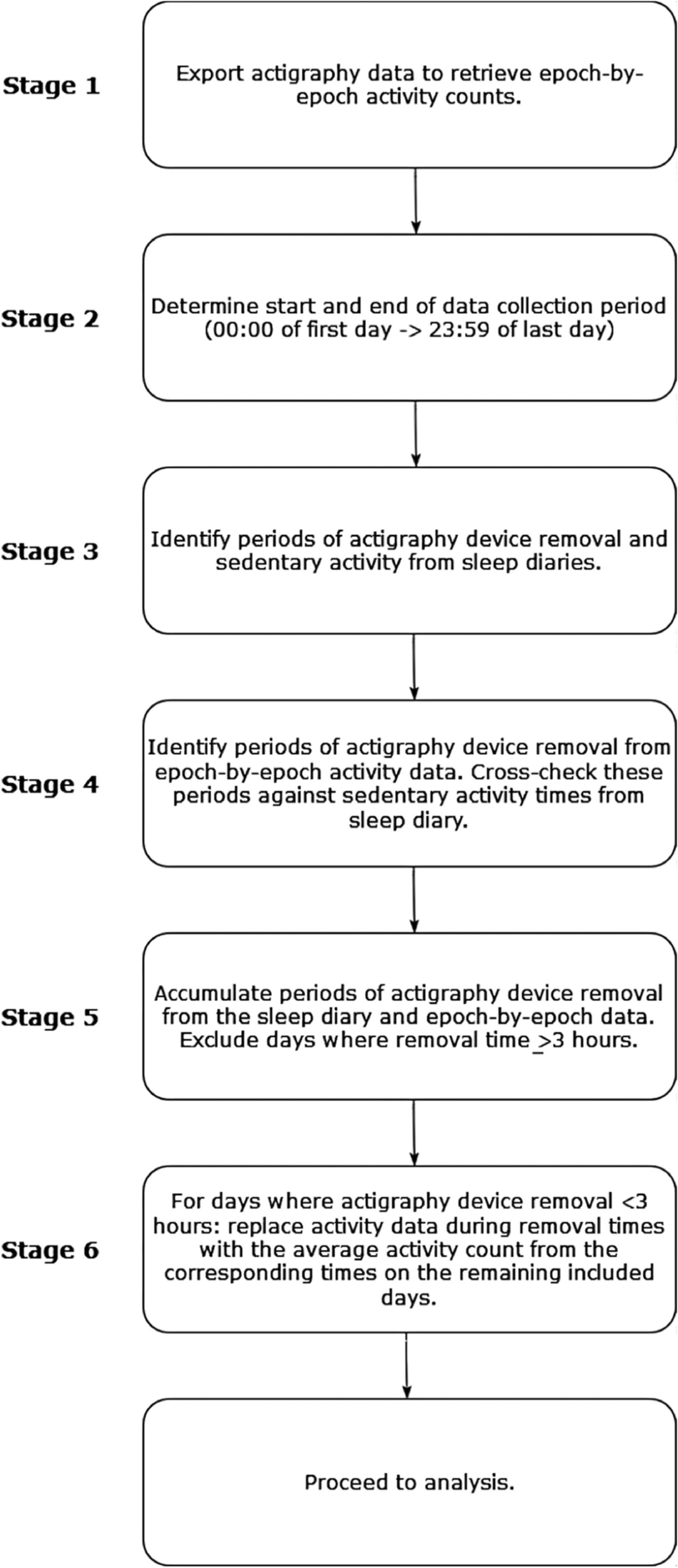
Fig. 1
Flowchart of study design, N = 62. Notes: ASD, autism spectrum disorders; CLDS-R, Child Language Disorder Scale-Revised; MCDI-T, Mandarin-Chinese version of the MacArthur-Bates Communicative Developmental Inventories Toddler; M-CHAT, Modified Checklist for Autism in Toddlers
At time 1, the Modified Checklist for Autism in Toddlers (M-CHAT) [30] was used as a screening tool to identify toddlers at high risk for ASD, and the Bayley Scales of Infant and Toddler Development, Third Edition (Bayley-III) [31] was used to identify children with cognitive delays. Furthermore, according to parental reports, all toddlers were born full term (gestational age > 36 weeks) with birth weights over 2500 g; no complications were encountered during pregnancy or delivery. Additionally, the participants had no other critical incidents, chronic diseases, or sensory-motor deficits.
Table 1 presents the participants’ demographic characteristics at age 2 (time 1). Although there were no differences between the TLD and LT groups (ps > .05) in demographic factors, 16.13% of TLD toddlers had a history of otitis media compared to 9.68% of LT toddlers. We also observed that few TLD or LT toddlers attended daycare. Approximately, 50% of TLD and LT toddlers had their parents as their primary caregivers. Over 70% of TLD and LT toddlers’ parents were educated at the university level and above, and over 50% of the toddlers were from middle- or high-income families. The two groups were similar in the history of otitis media, language exposure environment, and socioeconomic status.
Table 1 Sociodemographic characteristics of participants at age 2Table 2 presents participants’ cognitive and language scores at ages 2 (time 1) and 4 (time 2). No significant differences were noted in cognitive abilities by age in either of the two groups (ps > .05). The LT group exhibited lower receptive and expressive language skills than the TLD group at ages 2 [Fs(1, 60) = 16.48 and 143.65, respectively, ps < .001, ηp2s = .22 and .71] and 4 [Fs(1, 60) = 53.68 and 70.63, ps = .001, ηp2s = .47 and .54].
Table 2 Cognitive and language scores in the TLD and LT groupsMeasuresAssessment of language abilitiesWe assessed the participants’ vocabulary production at age 2 with the Words and Sentences Forms of the MCDI-T [25], which has been used to assess toddlers aged 16–36 months. Additionally, the participants’ receptive and expressive language abilities at age 2 were assessed using the receptive and expressive language subscales of the Bayley-III, which has been used to assess toddlers aged 16–42 months [31].
The Mandarin Chinese version of the Child Language Disorder Scale-Revised (CLDS-R) [32] was employed to assess participants at age 4 and included the two core subtests for auditory comprehension and expressive communication. The CLDS-R has been used to assess children aged 3–6 years.
Assessment of behavior problemsAt ages 2 and 4 years, behavior problems were assessed using the Mandarin Chinese version of the Child Behavior Checklist (CBCL-MC) for children aged 1.5 to 5 years [33]. Parents rated each item as 0 (not true), 1 (somewhat or sometimes true), or 2 (very true or often true). The scores were aggregated on eight syndrome subscales and three main scales. Scores on the emotionally reactive (e.g., “Disturbed by any change in routine”), anxious/depressed (e.g., “Unhappy, sad, or depressed”), somatic complaints (e.g., “Headaches (without medical cause)”), and withdrawn (e.g., “Shows little affection toward people”) subscales were aggregated to comprise the internalizing scale score. Similarly, the attention (e.g., “Can’t sit still, restless, or hyperactive”) and aggression (e.g., “Demands must be met immediately”) subscale scores were aggregated to comprise the externalizing scale score. Finally, the remaining two subscales, sleep problems (e.g., “Wakes up often at night”) and other problems, were combined with the internalizing and externalizing scales to comprise the total problems scale score. For the three main scales and seven syndrome subscales, except for the other problems syndrome subscale, raw scores could be converted to normalized T scores. The behavior problems status for the individual main scale and subscale scores were dichotomized as elevated (1 = the presence of behavior problems) or normal (0 = the absence of behavior problems). According to the CBCL’s definition, subscale scores below the 93rd percentile are considered normal, whereas scores at or above the 93rd percentile (T score ≥ 65) are considered elevated. For the major scales, scores below the 85th percentile are considered normal, whereas scores at or above the 85th percentile (T score ≥ 60) are considered elevated.
Assessment of cognitive abilitiesThe cognitive scale of the Bayley-III [31], administered in Mandarin Chinese, was employed to evaluate the participants’ cognitive abilities at age 2. This scale has been applied to children from birth to 42 months. At age 4 (i.e., over 42 months old), the participants’ cognitive abilities were measured using the Mandarin Chinese version of the Nonverbal Index (NVI) of the Wechsler Preschool and Primary Scale of Intelligence, Fourth Edition (WPPSI-IV) [34]. This test was designed for assessments in children aged 2 years and 6 months to 7 years and 11 months.
ProcedureAll tests were administered in a quiet room. Before testing, the researcher informed the parents of the research procedures, after which the parents provided their informed consent. The test administration duration for each wave was 1–1.5 h. Furthermore, the Bayley-III, the WPPSI-IV, and the CLDS-R tests were administered by a licensed clinical psychologist specializing in developmental psychopathology. The Research Ethics Committee of National Taiwan University, Taiwan, approved this study.
Data analysis planThe aim of the study was to examine the temporal stability of behavior problems in LT children compared to TLD children from toddlerhood to preschool age. First, to understand the relationship between changes in T scores from ages 2 to 4 in the LT and TLD groups and total problems, a group (LT versus TLD) by time (age 2/time 1 versus age 4/time 2) mixed-model ANOVA was performed. To assess the relationship between changes in T scores at both ages in the two groups and internalizing and externalizing behaviors and syndromes, 2 × 2 repeated-measures multivariate analyses of variance (MANOVA) was performed to adjust for chance significance due to multiple testing. Additionally, sleep problems subscale scores were not included in the internalizing and externalizing scales; rather, a 2 × 2 mixed-model ANOVA was conducted to test the sleep problem syndrome scores. The above tests adopted a significance level (α) of p < .05. Furthermore, each MANOVA was followed by 2 × 2 mixed-model ANOVAs for each dependent variable; where appropriate, degrees of freedom were adjusted using the Greenhouse-Geisser procedure when indicated necessary by Mauchly’s sphericity test. Furthermore, p-values were adjusted according to the Bonferroni procedure to guard against type-1 errors. Therefore, follow-up ANOVAs with internalizing and externalizing behaviors as dependent variables adopted a significance level (α) of p < .025 (=.05/2), those with internalizing syndromes (emotionally reactive, anxious/depressed, somatic complaints, and withdrawn) as dependent variables adopted p < .0125 (=.05/4), and those with externalizing syndromes (attention and aggression) as dependent variables adopted p < .025 (=.05/2). Effect sizes from the ANOVAs and MANOVAs were calculated using partial eta square (ηp2), which can be translated directly into percent of variance explained. Cohen [35] provided a basic framework for interpreting these effects as small (ηp2 = .01), moderate (ηp2 = .06), or large (ηp2 = .15). Due to small sample sizes, p-values less than or equal to 0.10 and ηp2 greater than or equal to .06 were considered to indicate trends. If behavior problems of LT children were more temporally stable than those of TLD children during toddlerhood and preschool age, a significant main effect of group would be found in the above tests.
Next, Fisher’s exact tests were conducted to test the differences in the percentages of participants with behavior problems between the LT and TLD groups for each of the CBCL scales and subscales at ages 2 and 4. Fisher’s exact test was also used to further understand whether the proportion of the presence of behavior problems at ages 2 and age 4 versus only at age 2 differed between LT children and TLD children. These tests were considered significant using a Bonferroni-corrected α level, as in the ANOVAs mentioned above. Due to small sample sizes, p-values less than or equal to 0.10 were considered to indicate trends. Finally, with each CBCL scale and subscale, the association of vocabulary size with concurrent behavior problems (i.e., at age 2) and those that develop over time (i.e., at age 4) among toddlers was examined by logistic regression analyses. All statistical analyses in this study were conducted using IBM SPSS Statistics 22.0.
留言 (0)