
記住我

Disclaimer: Early release articles are not considered as final versions. Any changes will be reflected in the online version in the month the article is officially released.
Author affiliations: National Center for Global Health and Medicine, Tokyo, Japan (Y. Miyazato, K. Yamamoto, G. Yamada, S. Kubota, M. Ishikane, M. Ueno, A. Matsunaga, T. Miyoshi-Akiyama, Y. Ishizaka, N. Ohmagari); National Center for Global Health and Medicine, Chiba, Japan (M. Sugiyama)
A 32-year-old man from France living in Tokyo was admitted to the National Center for Global Health and Medicine after experiencing shortness of breath and fever. He had received the first dose of the BNT162b2 (Pfizer-BioNTech, https://www.pfizer.com) vaccine 5 days before admission. After vaccination, he experienced a fever, systemic joint pain, nausea, and vomiting. The patient sought care because of these persistent symptoms.
At admission, the patient was experiencing dyspnea as well as chest and back pain that worsened during inhalation. The patient was obese (body mass index 42.1 kg/m2). He had no history of smoking, illegal drug use, or international travel. When he received the vaccine, Japan was experiencing its largest coronavirus disease (COVID-19) surge, but he had no known exposure to patients with COVID-19. At admission, he had a body temperature of 38.1°C and peripheral oxygen saturation (SpO2) of 95% on room air (Table). He had no notable jugular venous dilation, chest crackles, peripheral edema, or rashes.
Figure
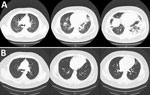
Figure. Chest computed tomography (CT) images of a male patient in Japan who was hospitalized with multisystem inflammatory syndrome. A) CT performed at hospital admission revealed infiltration in bilateral lower lobes....
Laboratory test results showed an elevated inflammatory response and cardiac enzymes (Table). Chest computed tomography (CT) showed smooth interlobular septal thickening, mixed lesions with ground-glass opacitie, and infiltrates in the bilateral lower lobes (Figure, panel A). Electrocardiography showed slight ST segment elevations in leads I, aVL, V1, and V2. Echocardiography showed no pericardial effusion, myocardial edema, or decreased wall motion. Real-time PCR results were negative for severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Loop-mediated isothermal amplification did not detect Legionella pneumophila. We used FilmArray version 1.3 (bioMérieux, https://www. biomerieux.com) to conduct a respiratory panel on respiratory specimens and a meningitis/encephalitis panel on serum specimens to detect herpesvirus, enterovirus, and cytomegalovirus; results of both panels were negative.
One day after admission, the patient’s dyspnea and hypoxemia worsened, and he experienced profuse cold sweats. His SpO2 dropped to 90% despite 10 L/min of oxygen supply. We suspected severe respiratory failure resulting from COVID-19 vaccine–related systemic inflammation and congestive heart failure. Therefore, we treated the patient with intravenous methylprednisolone at a dose of 1 mg/kg/day (125 mg/day) and with diuretics and noninvasive ventilation (NIV). The next day, his symptoms and hypoxemia greatly improved. He tapered off both treatments; he no longer needed ventilation 2 days after treatment and completed the course of steroids by the day of discharge, 7 days after admission. One month after discharge, CT was performed to confirm the improvement in the lung lesions (Figure, panel B).
Testing showed that SARS-CoV-2 spike IgG and neutralizing activities were significantly elevated 5 days and 23 days after the first COVID-19 vaccination dose had been administered (Appendix Figure 1). Moreover, SARS-CoV-2 nucleocapsid IgG in the serum was positive 5 days after COVID-19 vaccination. On the basis of these findings, we hypothesize that the patient had an asymptomatic or mild SARS-CoV-2 infection before vaccination. After his discharge, we measured a panel of 67 cytokines and chemokines from the patient and 3 healthy controls for comparison (Appendix, Table, Figure 2).
This case emphasized 2 clinical issues. First, severe respiratory failure can occur after COVID-19 vaccination, and steroids effectively alleviated this complication. Second, multisystem inflammatory syndrome in adults (MIS-A) can occur after COVID-19 vaccination in a previously infected patient and can manifest as respiratory distress. In cases of respiratory failure after the vaccination, a previous SARS-CoV-2 infection should be considered.
Postvaccination myocarditis has been reported as more common in male than female patients (1). Bozkurt et al. described mild cases (1); however, severe cases have also been reported (2). Although our patient’s myocardial damage was not severe, we suspected myocarditis based on his elevated troponin I level after COVID-19 vaccination. Vaccine-related myocarditis typically develops after the second vaccination, but it has been reported after the first vaccination of patients who had COVID-19 previously (1). Therefore, we considered the possibility of myocarditis after the first vaccination in this patient, because his serology results suggested a history of COVID-19. Moreover, his respiratory failure, severe inflammation, and serologic test results strongly suggesting a history of COVID-19 led us to suspect MIS-A, as reported by Morris et al. (3). Although the association between the COVID-19 vaccine and MIS-A development is unclear (4), the patient in our case fulfilled the clinical criteria of severe cardiac illness, hypotension, vomiting, and fever. In addition, his laboratory results showed elevated C-reactive protein levels, ferritin levels, interleukin-6 levels, and erythrocyte sedimentation rate. He also exhibited serologic positivity for SARS-CoV-2. These findings were consistent with the definition of MIS-A (5). This case showed that vaccination was a possible trigger of MIS-A in a patient who had a history of COVID-19.
The treatment for postvaccination myocarditis and MIS-A has not been standardized. As demonstrated in our case, immunosuppressive therapy, particularly corticosteroids, improved the prognosis. Intravenous immunoglobulin, anakinra, and infliximab have been used to treat multisystem inflammatory syndrome in children (6,7); a previous case report documented their role in treating MIS-A (8).
Dr. Miyazato is a clinical fellow in the Disease Control and Prevention Center at the National Center for Global Health and Medicine. His primary research interests are sexually transmitted diseases and clinical infectious diseases.
The conclusions, findings, and opinions expressed by authors contributing to this journal do not necessarily reflect the official position of the U.S. Department of Health and Human Services, the Public Health Service, the Centers for Disease Control and Prevention, or the authors' affiliated institutions. Use of trade names is for identification only and does not imply endorsement by any of the groups named above.
留言 (0)