
記住我
Worldwide, superficial burn wounds are treated with different synthetic and biological dressing materials.1-4 Many of these commercially available dressing materials are expected to accelerate wound healing and reduce scarring. Additionally, patient satisfaction in terms of reduction of pain, dressing changes, and fluid loss is desired.3, 5-10 Owing to the economic pressure in many hospitals, cost remains an important issue. Thus, an ideal cost-effective dressing with the best wound healing properties and high patient satisfaction is required. In this context, pure natural silk, which has been used for medical purposes for thousands of years, seems to be an interesting material. Silkworm silk, consisting of the protein fibroin, is biocompatible, has tunable mechanical properties, and leads to minimal inflammation in host tissue.3, 11 With these advantages, it has become the focus of many wound healing studies in recent years.3, 12 Dressilk (PREVOR, France) is a wound dressing made of pure knitted silkworm silk. After application to the wound, Dressilk first adheres to the wound base, to then slowly dry and peel off as wound healing proceeds.12
In a previous study, we showed that Dressilk is an equivalent alternative to Biobrane, a commonly applied biosynthetic skin substitute, regarding reepithelisation, patient satisfaction during cicatrisation,3 and better results than Polymem in terms of infection and exudation.4 Since then, Dressilk is the standard of care (SOC) for the treatment of superficial, partial thickness burn wounds in our burn centre.
Many other burn centres use the much more expensive Suprathel (Polymedics, Germany), a biosynthetic copolymer wound dressing mainly based on DL-lactic acid on the base of paraffin, for the treatment of partial thickness burns.13 It is expected to promote wound healing, reduce wound infection, and increase patient comfort.13
Therefore, we aimed to compare the widely used but very expensive Suprathel with the rather new and cheaper Dressilk in the clinical setting.
2 METHODSThe present study evaluated prospectively the healing of partial thickness burn wounds after simultaneous treatment with Suprathel and Dressilk in a clinical setting.
This study was reviewed and approved by the Ethical Review Committee of the University of Witten Herdecke, Germany (ethic approval number 5/2017), and the protocols adhere to the Declaration of Helsinki.
Altogether, between May 2017 and May 2018, a total of 20 patients with partial-thickness burns were treated simultaneously with Suprathel and Dressilk.
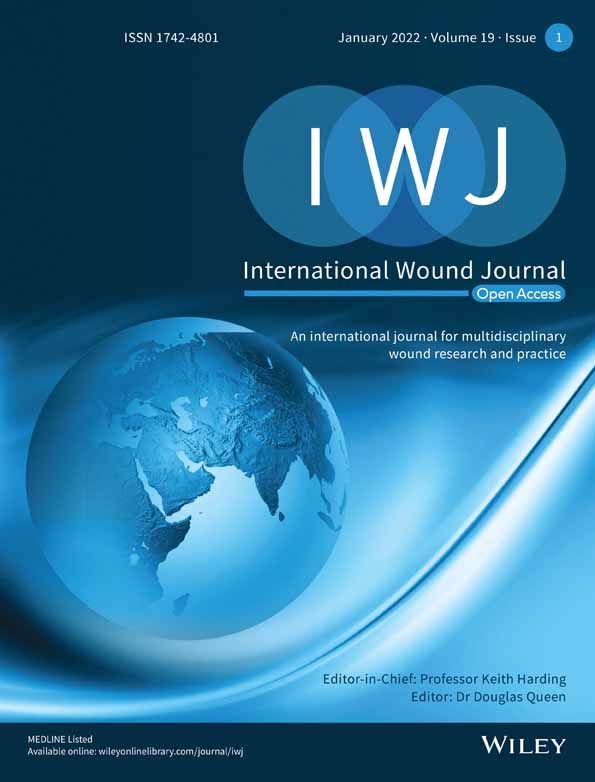
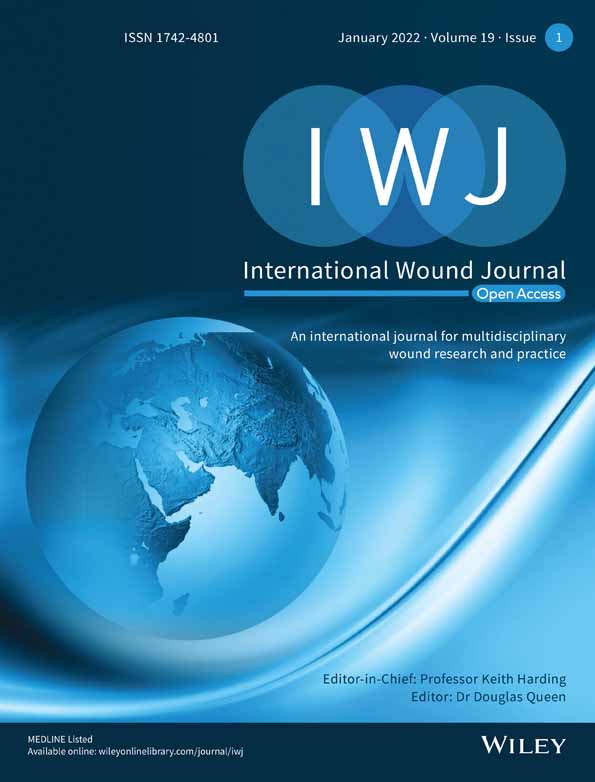
After hospital admission of a patient, burn depth was clinically assessed by a senior burn specialist according to standard clinical characteristics such as skin colour, capillary refill, skin pliability, sensation, presence of blisters, and presence of thrombosed vessels. In case the wound was assessed as superficial and the patient fulfilled the inclusion criteria, then the patient was offered to participate in the study. Complete informed consent was obtained from all patients before the start of the study. After inclusion in the study, the burn wound was mechanically debrided and cleaned with moist Prontosan cotton gaze, then the burned wound was treated partly with Suprathel and partly with Dressilk (Figures 1 and 2). During the first few days, an external dressing with fatty gauze and cotton gauze was placed on top of both dressings until exudation decreased. As reepithelisation proceeded, the dressings were gradually cut back until they could be removed completely.

Partial thickness burn of the right forearm and hand; A, B, before and after debridement; C, during the wound healing with the two dressings (Suprathel marked with the green stripe; D, 3-month follow-up

Partial thickness burn of the left hand; A, after debridement and treatment with the two dressings (Suprathel marked with the green stripe and covered with fatty gauze); B, 12-month follow-up
2.1 Patient enrolmentInclusion criteria were that all patients must be at least 18 years old, have a partial-thickness burn wound caused by contact with a hot surface, flames, or a hot liquid and a wound area ≥0.3% of total burn surface area (TBSA).
Exclusion criteria were lack of acquiescence and understanding of the follow-up examination, presence of inhalation trauma, burns caused by electricity or chemical substances, localisation of the burned area in the face, or an ABSI score of 10 or more.
2.2 Wound evaluationThe wounds were evaluated with the verbal rating scale from 0 to 10 on days 2, 4, 6, 8, 12, 16, 24, and 48 in regard to (1) pain, (2) infection, (3) exudation, and (4) bleeding. Additionally, the wounds were photo-documented regularly. External dressing changes were performed superficially to evaluate infection, exudation, and bleeding.
2.3 Scar evaluationSubsequently, scarring was evaluated after 12 months. The follow-up examination started with a photo documentation, followed by a scar assessment with the Patient and Observer Scar Scale (POSAS) a feasible and reliable assessment scale containing the opinion of both patients and observers.3, 14-18
2.4 Statistical analysisMicrosoft Excel (2017, Microsoft) was used for data analysis and chart creation. After a thorough review of all data, SPSS (Version 21, IBM) was used for final statistical analysis. Statistical significance was accepted at P ≥ .05.
With 20 pairs of data, a difference of two-thirds of SD could be detected (alpha <.05) with sufficient power (80%). Statistically significant differences between the subgroups were identified with the Friedman and Wilcoxon tests.
3 RESULTSBetween May 2017 and May 2018, 20 patients, 12 males and 8 females with partial thickness burn wounds, participated in the clinical trial and the follow-up examination (Table 1). Their mean TBSA was 7.1% (SD 4.88). The mean TBSA treated with silk was 1.8% TBSA (SD 1.05) and Suprathel 2.0%TBSA (SD 1.09). No adverse events occurred.
TABLE 1. Overview of the patient characteristics Patient Sex Age Trauma Cause Treated area with Dressilk Treated area with Suprathel TBSA (%) Days until 95% wound closure Dressilk Days until 95% wound closure Suprathel 1 M 40-60 05/2017 Flame2% TBSA
right forearm
2% TBSA
right hand
10 14 14 2 M >60 05/2017 Hot fluid2% TBSA
left thigh
3%TBSA
right thigh
12 22 22 3 M 20-40 05/2017 Flame4%TBSA
left thigh
4% TBSA
right thigh
9.5 17 17 4 M 40-60 06/2017 Flame2% TBSA
right hand and forearm
2% TBSA
right forearm
5 22 22 5 M 40-60 06/2017 Hot fluid 2.5%TBSA right forearm2.5% TBSA
left forearm
15 13 13 6 M 40-60 09/2017 Flame 0.3% TBSA left D1 + D20.3% TBSA
Left D3-D5
0.8 10 10 7 F 40-60 10/2017 Hot fluid1% TBSA
Right forearm
1% TBSA left upper arm 2 16-24 16-24 8 F 40-60 11/2017 Flame0.3% TBSA
Left hand
0.3% TBSA
Right hand
5 8 8 9 F <20 12/2017 Hot fluid1.5% TBSA
left distal thigh
0.5% TBSA
left proximal thigh
2 16-24 16-24 10 M 20-40 12/2017 Explosion2% TBSA
left upper arm,
2% TBSA
left forearm
11 12 12 11 F 20-40 01/2018 Hot fluid1.5% TBSA
right distal thigh
1% TBSA
right prox. Thigh
2.5 16-24 16-24 12 F 40-60 01/2018 Hot fluid2%TBSA
Right breast
1%TBSA
abdomen
16 19 19 13 M 20-40 02/2018 Hot fluid3.5% TBSA
left hand and forearm
3.5% TBSA
Right hand and forearm
7 21 21 14 M 20-40 03/2018 Hot fluid 0.5% TBSA right prox. Forearm0.5% TBSA
Right hand and forearm
1 12 12 15 M 20-40 03/2018 Flame2% TBSA
right hip
0.5% TBSA
Right hand
6 9 11 16 M 20-40 04/2018 Flame2% TBSA
Thorax, left forearm
2%TBSA
Left upper arm and distal forearm
16 9 9 17 M >60 05/2018 Flame3% TBSA
Right upper arm
3% TBSA
right forearm
7 16 16 18 F 20-40 05/2018 Hot fluid 1% TBSA abdomen1% TBSA
Abdomen, upper leg
4 13 13 19 F 40-60 05/2018 Hot fluid2.5% TBSA
right thigh
2.5% TBSA
right shank
5 16-24 16-24 20 F 40-60 05/2018 Hot fluid2% TBSA
left upper leg and foot
3% TBSA
left shank and forearm
5 16-24 16-24 Abbreviation: TBSA, total burn surface area. 3.1 Wound healingAll wounds healed in the first 24 days, with no complications in the form of infection or bleeding. The exact time until wound close (defined as 95% initial wound area closed) was documented for 15 patients of which 14 patients showed no difference between the two dressings. The wounds of the remaining patients closed between the follow-up examination on days 16 and 24. Solely for one patient different time to wound closure was documented for Dressilk and Suprathel (Table 1). Hereby, the wounds treated with silk were closed 2 days earlier. The exudation of the wounds decreased continuously (Figure 3) without a significant difference between the wound dressings. After day 16, no exudation could be detected. Pain declined continuously (Figure 4) and solely differed significantly between the two dressings on day 2, where the wounds treated with Suprathel showed a lower pain level than the ones treated with Dressilk (P = .025).

Mean exudation of wounds treated with Dressilk und Suprathel in the first 48 days

Mean pain level of wounds treated with Dressilk und Suprathel within the first 48 days
3.2 POSAS—Patient and Observer Scar ScaleIn the 12-month follow-up examination, the POSAS Patient Scale showed no significant difference between the two dressings regarding pain, itching, skin colour, elasticity, skin thickness, and surface structure of the skin (Table 2). Additionally, the POSAS Observer Scale evaluated blood circulation, pigmentation, elasticity, thickness, and surface structure of the skin. Here, solely, the category vascularity (Dressilk mean 1.58, SD 0.84; Suprathel mean 2.05, SD 1.08; P = .047) and the overall opinion (Dressilk mean 1.68, SD 0.58; Suprathel mean 2.21, SD; P = .013) differed between the areas treated with the two dressings significantly (Table 3).
TABLE 2. POSAS Patient Scale after 12 months, no significant differences between the two dressings (Wilcoxon) POSAS Patient Scale categories Dressilk Suprathel P value Pain Mean 1.00 1.00 1.000 SD 0.00 0.00 Itching Mean 1.21 1.16 .317 SD 0.71 0.50 Colour Mean 1.94 2.39 .101 SD 0.94 1.09 Stiffness Mean 1.00 1.33 .059 SD 0.00 0.77 Thickness Mean 1.11 1.28 .414 SD 0.32 0.75 Skin irregularity Mean 1.39 1.56 .429 SD 0.85 1.20 Overall Mean 1.84 1.89 .739 SD 0.96 0.81 Abbreviation: POSAS, Patient and Observer Scar Scale. TABLE 3. POSAS Observer Scale after 12 months POSAS Observer Scale categories Dressilk Suprathel P value Vascularity Mean 1.58 2.05 .047 SD 0.84 1.08 Relief Mean 1.11 1.32 .102 SD 0.32 0.58 Pigmentation Mean 1.89 2.32 .244 SD 0.66 1.49 Pliability Mean 1.00 1.11 .157 SD 0.00 0.32 Thickness Mean 1.05 1.26 .102 SD 0.23 0.65 Surface area Mean 1.00 1.11 .157 SD 0.00 0.32 Overall Mean 1.68 2.21 .013 SD 0.58 1.03 Abbreviation: POSAS, Patient and Observer Scar Scale. 4 DISCUSSIONTo the best of our knowledge, this is the first clinical trial comparing the wound dressings Dressilk and Suprathel intra-individually in partial-thickness burns. The prospective intra-individual study design seemed particularly fitting to minimise pre-existing differences in patients, such as those in comorbidities, wound healing, pain sensation, or scarring.
4.1 Pain and bleedingDressing changes in burn patients are found to be very painful and often result in bleeding. Poor pain control and disruption of the reepithelisation process through dressing changes leading to bleeding can hamper the healing process.19-22 One of the major advantages leading to the frequent use of Suprathel is the relatively painless and often unnecessary removal compared with other synthetic dressings.13, 23 In congruence to this, we showed that, at day 2, the wounds treated with Suprathel seemed to be painless than the wounds treated with Dressilk. Further, one could assume that the less frequent use of analgesics minimises the cardiovascular risk of the patient. Overall, we could not show further significant differences between Suprathel and Dressilk in subjective pain assessment in the following phases of wound healing. Both dressings did not require dressing changes and no bleeding occurred. In previous studies, we showed that pain levels declined in the course of the wound healing, regardless of the type of dressing used.3 In contrast to our recent results, in our previous study, significant differences in pain levels were found only at day 4, with a slightly higher pain level for Dressilk than for Biobrane.3 To the extent that painless healing and handling are supposed to be the supporting arguments for the use of the biosynthetic Suprathel,23, 24 our findings show equal pain levels regardless of the applied wound dressing. These findings are very interesting in regard to a study that showed that pain and, in the later course, itch are the most disturbing scar parameters for the burn victim.25
4.2 Exudation and infectionDuring wound healing in burn injuries, accumulated wound fluid or wound infections have to be managed accurately.26, 27 Burn wounds are associated with a large amount of inflammation with pro-inflammatory cytokines impairing wound healing.28, 29 Dressilk, which consists of a natural material, was already shown to be anti-infective.12, 30-35 Additionally, Ju et al were able to show in a burn rat model that silk fibroin significantly reduces the expression of the pro-inflammatory cytokine IL-1α.36 Because of these properties, a number of antibacterial wound dressings are based on silk fibroin.37 Furthermore, silk sericin, a protein from the silkworm cocoon, was found to ameliorate wound healing by promoting the migration of fibroblast L929 cells.34
Dressilk is also less exudative than other synthetic wound dressings, for example, PolyMem.4 Consistent with this, exudation of wounds dressed with Suprathel or Dressilk continuously decreased until day 16, where wounds were closed and no exudation could be detected anymore (Figure 2). Similar to the well-known Biobrane, Suprathel has been shown to detach from the wound in case of an infection.38 The available literature does not show a high rate of infections in wounds treated with Suprathel, which is in line with our results.24, 38, 39 Similarly, our previous study results showed not only a rapid decrease in exudation rates in dressings such as Dressilk and Biobrane but also no significant differences between the two materials.3
5 SCAR ASSESSMENT 5.1 Subjective scar assessmentThe POSAS Observer Scale showed significant differences in vascularity and the overall opinion between the wounds treated with the two different dressings, with the areas treated with Dressilk being more similar to uninjured skin. Nevertheless, concerning burn rehabilitation, patient satisfaction concerning scaring among burn survivors is of high importance.40 The appearance of the scar majorly influences the patients' opinion about the final result.16, 41 We therefore assessed the scar focusing on patient satisfaction.
The POSAS Patient Scale as a validated tool3, 15, 42, 43 showed no significant differences between Suprathel and Dressilk regarding pain, itchiness, skin colour, elasticity, scar thickness, surface structure, and overall evaluation for the patients after 12 months. Moreover, in our previous study, we were not able to detect significant differences between silk and the compared wound dressings.44 As far as burn rehabilitation starts from the day of the injury,45 both wound dressings seem to have subjectively equal efficacy for the patient according to our results.
6 IMPACTIdeally, scar assessment tools allow an objective statement about the benefits of different wound dressings. Overall, in our study, no major distinctions were found between the two products. In recent studies and skin engineering research, silkworm silk has gained increasing interest as a skin replacement material.31, 46 Furthermore, the high acquisition costs of Suprathel support the use of Dressilk. Suprathel is ~20 times more expensive than Dressilk for a clinical setting. All other treatment costs for the two dressings are identical because, apart from the applied dressing, treatment is identical including costs for personnel, hospital stay, follow-up examinations, and external dressings. Our study results showed that Dressilk is a cost-effective dressing material.
7 LIMITATIONSA critical pain evaluation is often difficult. In this intra-individual study design, with the two dressings being partly placed next to each other, it might be difficult for some patients to differentiate between the two dressings. If possible, the two dressings were placed on similar body parts far apart for better pain evaluation. Apart from this, every patient has an individual pain sensation. Through the intra-individual comparison,
留言 (0)