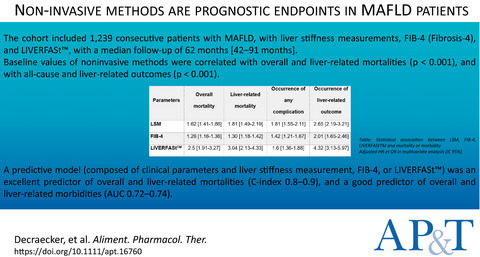
We read with interest the editorial from Dr Ogawa and thank him for his comments about our research.1, 2 Concerning the possibility that patients with high PIVKA-II levels at baseline could harbour hepatocellular carcinoma (HCC) nodules at the time of direct-acting antivirals (DAA) initiation, in our cohort last HCC surveillance imaging was performed within 3 months before the start of the treatment. As our study was retrospective and conducted in a clinical practice setting, we could not perform a second-level imaging technique such as enhanced dynamic computed tomography (CT) or magnetic resonance imaging (MRI). We agree that a CT/MRI could be useful to definitely exclude the possibility of HCC existence at baseline. However, such assessments are not recommended in clinical practice setting by international guidelines, also in patients with elevated biomarkers (including alpha-fetoprotein).3 Nevertheless, in order to rule out the potential bias of patients with baseline elevated PIVKA-II levels and/or early HCC onset in our study, we conducted three additional sub-analyses, by excluding patients with baseline PIVKA-II>100 mAU/ml (Model A), PIVKA-II> 60 mAU/ml (Model B) and patients with HCC development <12 months after the end of DAA treatment (Model C). Results of these analyses are reported in Table 1: in all models, end of treatment (EOT)-PIVKA-II was re-confirmed as an independent predictor of HCC development, while the best cut-off for HCC prediction identified at ROC curve analysis remained unchanged from the overall analysis (>41 mAU/ml). According to the three models, the 4-year cumulative probability of HCC in patients with or without EOT-PIVKA-II>41 mAU/mL resulted 18.2% vs 1.9% (P < 0.0001) in Model A, 21.2% vs 2% (P < 0.0001) in Model B and 15.4% vs 0.4% (P < 0.0001) in Model C, respectively.
TABLE 1.
End-of-treatment (EOT) predictors of HCC development, when excluding patients with baseline PIVKA-II>100 mAU/mL (Model A), >60 mAU/mL (Model B) or patients with HCC onset <12 months after EOT (Model C)
EOT variables
EOT variables category
Univariate analysis
a
Multivariate analysis
a
HR (95% CI)
P value
HR (95% CI)
P value
Model A
Diabetes
Yes vs No
3.72 (1.66-8.31)
0.001
5.35 (2.05-14.0)
0.001
ALP (U/L)
Continuous
1.01 (1.00-1.02)
0.01
—
—
GGT (U/L)
Continuous
1.01 (1.00-1.02)
0.0001
1.01 (1.00-1.02)
0.03
Albumin (g/dl)
Continuous
0.29 (0.11-0.74)
0.01
—
—
AFP, log ng/ml
Continuous
2.16 (1.23-3.79)
0.01
2.60 (1.33-5.04)
0.04
PIVKA-II, log mAU/ml
Continuous
4.03 (2.43-6.69)
<0.0001
3.59 (2.00-6.41)
<0.0001
Model B
Diabetes
Yes vs No
4.12 (1.71-9.90)
0.002
4.69 (1.76-12.49)
0.002
ALP (U/L)
Continuous
1.01 (1.00-1.02)
0.01
—
—
GGT (U/L)
Continuous
1.01 (1.00-1.02)
0.005
—
—
Albumin (g/dl)
Continuous
0.23 (0.09-0.62)
0.004
—
—
AFP, log ng/ml
Continuous
2.01 (1.07-3.80)
0.03
2.57 (1.36-4.86)
0.004
PIVKA-II, log mAU/ml
Continuous
4.09 (2.33-7.22)
<0.0001
4.31 (2.37-7.85)
<0.0001
Model C
Diabetes
Yes vs. No
2.70 (1.06-6.87)
0.04
—
—
GGT (U/L)
Continuous
1.01 (1.01-1.02)
0.005
1.01 (1.01-1.02)
0.01
Albumin (g/dl)
Continuous
0.35 (0.13-0.93)
0.03
—
—
PIVKA-II, log mAU/ml
Continuous
2.98 (1.91-4.66)
<0.0001
3.00 (1.85-4.86)
<0.0001
Note
Variables not statistically significant at univariate analysis: age, gender, BMI, HCV genotype, ALT, AST, bilirubin, creatinine, platelets, varices, DeltaAFP, DeltaPIVKA.
Abbreviations: AFP, alpha-fetoprotein; ALP, alkaline phosphatise; EOT: end of treatment; GGT, gamma-glutamyl-transferase, PIVKA-II, protein induced by vitamin K absence or antagonist-II; HCC, hepatocellular carcinoma.
In Model C, after excluding patients with HCC development <12 months after EOT, 20 patients still had baseline PIVKA-II>100 mAU/ml without any evidence of HCC development during a subsequent median follow-up of 52 (7-60) months. Therefore, despite the high specificity of increased PIVKA-II levels for HCC, some HCC-free patients still display persistently increased PIVKA-II levels. Interestingly, in our study, PIVKA-II levels correlated with some features associated with advanced liver disease, such as increased bilirubin, low albumin, and Child-Pugh score (Table S1).2
In conclusion, while our study was the first to investigate the role of PIVKA-II in a large cohort of patients with HCV-related cirrhosis treated with DAA, further (prospective) research is needed to confirm the clinical meaning, the diagnostic and predictive value of PIVKA-II for HCC diagnosis and surveillance in such patients.
Elisabetta Degasperi collected, analysed the data and wrote the paper, Roberta D'Ambrosio and Pietro Lampertico critically revised the manuscript. All authors approved the final version of the manuscript. The authors' declarations of personal and financial interests are unchanged from those in the original article.2









留言 (0)