Risk factors and treatment strategy for clinical hepatico‐jejunostomy stenosis defined with intrahepatic bile duct dilatation after pancreaticoduodenectomy: a retrospective study
Backgrounds/Purpose
The purpose of this study was to identify risk factors and establish a treatment strategy for clinical hepatico-jejunostomy stenosis defined with intrahepatic bile duct dilatation after pancreaticoduodenectomy.
Methods
The 443 patients who underwent PD from April 2006 to December 2015 were analyzed. Clinical characteristics were compared between patients with and without clinical HJ stenosis, and risk factors for clinical HJ stenosis were analyzed. In addition, the treatment and clinical course of patients with clinical HJ stenosis were retrospectively reviewed.
Results
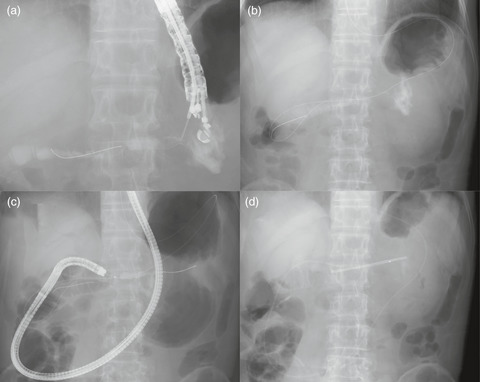
Clinical HJ stenosis defined with intrahepatic bile duct dilatation was identified in 40 patients (9.0%). Multivariate analysis revealed that the independent risk factor for clinical HJ stenosis was the hepatic duct at surgery ≤ 8 mm. Endoscopic HJ stenosis was identified in 36 patients, and 31 patients were treated successfully with double balloon endoscopic retrograde cholangiography; 5 patients required re-anastomosis (n=3) and percutaneous transhepatic biliary drainage (n=2). Complete obstruction of HJ was found in 5 patients, and treatment with DB-ERC was successful in only one patient.
Conclusion
The independent risk factor for clinical HJ stenosis was hepatic duct diameter ≤8 mm. Most cases of endoscopic HJ stenosis were treated successfully with DB-ERC, except in patients with complete obstruction.



留言 (0)