
記住我


Early sepsis recognition and treatment are essential to reduce the burden of disease.1, 2 Most patients with sepsis will present to EDs either following referral from primary care, via ambulance or as walk in self-referrals.3 Therefore, ED recognition and management of sepsis is a crucial determinant of patient outcomes.3, 4 In Australia, 500 000 patients a year are seen in ED with sepsis.3 In New Zealand (NZ) and Australia 18 000 patients are admitted to an intensive care unit (ICU) with sepsis annually.5 Despite significant advances in emergency and intensive care medicine, morbidity and mortality remain high; particularly in those who develop shock or have significant pre-existing medical comorbidities.6-8 In NZ, the in-hospital and 1-year mortality from sepsis is estimated to be 19 and 38%, respectively.9
A multitude of challenges confront ED clinicians when diagnosing sepsis.10 Foremost, a wide range of infective pathogens and clinical syndromes can cause sepsis. Affected are patients of all ages with a heterogeneous variety, severity and number of pre-existing comorbidities.3, 4 Also, no gold standard or definitive test can reliably diagnose sepsis; therefore, patients rely on the ability of clinicians to accurately interpret presenting symptoms, vital and other clinical signs, and available tests.10 The dynamic, time-pressured and often overcrowded ED environment can also confound matters.1, 3, 10
The initial assessment and management of patients with sepsis is often first undertaken by ED nurses and resident doctors such as ED registrars. Limited evidence exists examining these clinician's perspectives of managing sepsis in a busy ED environment.11, 12 The present study intends to explore the perceptions of ED nurses and doctors, regarding sepsis management in ED; particularly factors that confound the ability to identify, diagnose and manage sepsis within the ED.
Methods Study design and settingThis was a cross-sectional qualitative study conducted between 30 January 2020 and 27 February 2020. Semi-structured focus group interviews were performed to collect data. Included participants are ED nurses and doctors from Wellington Regional Hospital ED, a publicly funded major referral centre in NZ, with an annual census of 75 000 patients. Patients are seen by a triage nurse on arrival and receive a triage code from 1–5 guided by the Australasian Triage Scale framework.13 If sepsis is suspected at triage or during the assessment, they are placed onto a local ‘Adult Sepsis Management’ pathway. There is also a locally designed mobile application, Empiric, which provides local antibiotic guideline advice for prescribers. The Wellington Hospital ED department uses a specialised Emergency Department Information System (EDIS), while hospital inpatient services use the Concerto electronic health record (Orion Health [NZ] Ltd).
Participant selectionA purposeful sample of nurses and doctors currently working in ED were invited to attend a focus group interview. The invitation was designed and reviewed by all investigators prior to distribution to all ED nurses and doctors via the weekly ED bulletin email, on notice boards, during teaching sessions and handover sessions. The arm-length approach was respected and only staff who volunteered to take part were included. All participants received an information sheet prior to the interview and provided written informed consent. No participants withdrew from the study.
Semi-structured focus group interviewsFocus groups were used as a method of obtaining qualitative data through the group sharing of socially contextualised knowledge.14 The approach allows interviewers to determine what knowledge is seen as a reflection of the collective experience, as well as where there is a diversity of thought and opinion on the study topic. The choice of a semi-structured interview method allowed for researchers to elicit information from their pre-prepared questions, while also allowing the participants the opportunity to elaborate on their lived experience and provide other perspectives on the topic not anticipated by the research team.14
Six focus group interviews, each with six to eight participants were conducted in the ED seminar room. This falls within recommended guidelines for focus group size to allow opportunity for all to contribute while still achieving a group dynamic.14 Three interviews had nurse participants and three interviews had doctor participants. To facilitate discussion, participants were matched where possible by experience.
Participants were seated in a circle, including two facilitators who were spaced apart. One facilitator was a female senior ED registrar (AR) and the other was a female senior ED research nurse (JL, HS or JB). A third facilitator was introduced to the group but sat separately in the background (BR). Their role was to observe and moderate the interviews to ensure each focus group covered similar questions and were of similar format. AR, HS and JB had no prior focus group facilitator experience so BR and JL provided training to the investigators on key skills including active listening, thoughtful linguistic choices and avoiding assumptions and leading questions.14
Participants completed a voluntary demographic data collection form detailing their ED work experience. After a brief introduction outlining the research intentions, the facilitators asked a selection of questions that were pre-determined by study investigator consensus (Table 1). All investigators reviewed the data collection instrument and had opportunity to provide feedback and suggest changes. No pilot testing was performed as the questions were written by researchers who possessed clinical and research knowledge regarding sepsis care in ED. The questions were used only as a guide to facilitate discussion. If the question had already been covered during the discussion facilitators would move on. If the discussion was moving beyond the scope of the questions, participants would be redirected. All questions listed were covered in some form during each interview. Disagreements within interviews were allowed to be discussed amicably. Interviews were audio-recorded onto two digital audio recording devices and stored securely. No interviews were repeated. The interviews were transcribed by a professional medical typist who works with BR at Victoria University. The typist had no identifying information relating to the participants and coded voices only.
TABLE 1. Questions from the interview guide for facilitators Interview questions and prompts 1 Can you think of a patient that was treated for sepsis in the department that went particularly well or did not go particularly well and why? 2 What factors in the ED do you think affect the treatment of patients with sepsis? 3 Does the patient's prior health affect your approach? 4 Are there any particular aspects of diagnosis and treatment of sepsis that you find particularly challenging? 6 How do you approach patients who may have sepsis currently? Do you use any clinical tools or guidelines? 7 What can be done in ED to provide equitable care? 8 How regularly do you communicate with the relatives and whanau of patients with sepsis? Do you explain what sepsis is? 9 Have you received any teaching or training on sepsis? Would this be helpful? Data analysisAudio recordings and transcripts were available via a secure password protected shared drive. Two study investigators (AR/JL) cross referenced the transcripts against the recordings to ensure accuracy and verbatim. The transcripts were then uploaded to NVivo 12 (QSR International, Melbourne, Australia) qualitative data analysis software.15 Data were analysed using thematic analysis guided by the six-step framework detailed by Braun and Clark.16
The transcribed interviews were read through multiple times by two study investigators (AR and JL) to ensure familiarity and gain a sense of the dataset as a whole. Following this, the transcripts were coded into nodes by the two investigators independently. This form of data categorisation groups meaningful phrases with similar content. The two investigators compared nodes and discussed similarities and differences. Investigators mutually agreed no new nodes were being created during the fifth and sixth interviews, demonstrating that data saturation had been reached.14 Following this, discussion with a third investigator (NR) was performed to determine subthemes. These subthemes were reviewed and refined until three main final themes were determined. These themes were discussed and agreed by all study investigators. The final report was distributed to study participants for comment. Feedback was positive with no requests for changes or additions.
The COREQ checklist was adhered to during study design and manuscript writing.17 Ethical approval was obtained through the University of Otago Human Ethics Committee (Reference D20/008).
ResultsSample characteristics of the 40 included clinicians are detailed in Table 2. With participants comprising of a mix of professions and years of experience, the focus group method was well-suited to generating data through analogous group interaction.14 The six semi-structured focus group interviews performed had a median length of 33.5 (range 27–38) min.
TABLE 2. Participant demographics and ED work experience n = 40 Frequency Sex, n (%) Female 28 (70) Male 11 (27.5) Prefer not to say 1 (2.5) Ethnicity, n (%) Māori 3 (7.5) Asian 7 (17.5) NZ European 22 (55) Other 8 (20) Occupation, n (%) Registered nurse 18 (45) Resident medical officer 19 (47.5) Trainee intern 3 (7.5) ED work experience (years) Median (IQR); range 2.37 (0.5–5.4); 0.1–25 Wellington ED, median (IQR) 1.0 (0.25–2.5) <12 months, n (%) 12 (30) 1–2 years, n (%) 7 (17.5) 2–3 years, n (%) 2 (5) 3–5 years, n (%) 7 (17.5) 5–10 years, n (%) 8 (20) >10 years, n (%) 4 (10) Other work experience (yes), n (%) ICU 11 (27.5) Medical ward 26 (65) Surgical ward 27 (67.5) Paediatrics 9 (22.5) GP/Community 7 (17.5) Prior focus group participation, n (%) Yes 8 (20) Thematic analysisThe three main themes identified were: clinical management, challenges and delays, and communication. Additional quotations supporting the interpretation of the themes and subthemes are displayed in Table 3.
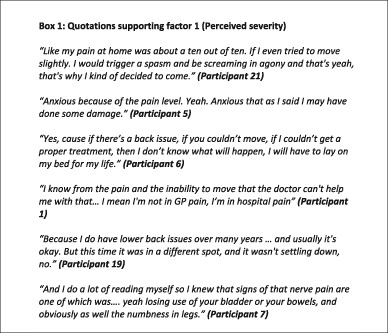
TABLE 3. Themes, subthemes and selected quotations Theme Subtheme Quotations 1.0 Clinical management 1.1 Early recognition of sepsis ‘Like often ambulances, when they're bringing patients in, have already identified that this patient probably had sepsis. And then they're the sort of the ones that tend to go pretty well’ (FG 1 – doctors) ‘You'll know you'll get a sick sepsis coming in. And that's when it goes really well, because you're like, okay, get the pathway, get the bloods, just everything ready to go’ (FG 6 – nurses) 1.2 Auxiliary resources ‘I think use of the protocol that we've got in Wellington is quite helpful. So a triage nurse or someone will say, “I think this person is septic,” and so that means all the bloods and things are done quickly, and they're seen quickly and the goal is fluids, antibiotics quickly’ (FG 4 – doctors) ‘Once the patient is triaged the nurses here are very good at doing all the sepsis stuff. So yeah, doing the IV line, getting the blood cultures, like trying to get a urine. They've got a protocol, they follow it. By the time you get to them three hours later, a lot of the work-up stuff is done’ (FG 3 – doctors) ‘That's true, actually. The number of times that you get the sepsis sheet brought to you by the nurse who's looking after them in the room, and say, “I've done this and this, what do you think?”’ (FG 3 – doctors) ‘It's important to find out when you go somewhere what the local choices are, because they'll have been made in conjunction with the infectious disease, microbiology teams, depending on the sensitivities of the area’ (FG 1 – doctors) ‘The Empiric app is very helpful. That usually guides you whether they've got sepsis – or mild and which antibiotic to give them’ (FG 1 – doctors) 1.3 Triage ‘If we happen to get early identification then we're sweet as, and that really comes down to the triage nurse, which is probably the most difficult job in all of the ED, is the triage nurse’ (FG 3 – doctors) ‘It's quite hard to get an all-round flag that everyone's on the same page, that they know that this patient is at risk of sepsis. There's no like cool red flag that's easily spotted’ (FG 4 – doctors) ‘The triage nurses especially on night shifts, it's the most important thing in the whole department’ (FG 3 – doctors) ‘They wait for hours and deteriorate, if you had triaged them again they would have been a code 2, but you don't realise that they got worse’ (FG 2 – nurses) 2.0 Challenges and delays 2.1 Factors the ED can control ‘Whereas if they presented like that, they would have been immediately a triage 2, into resus. But because they're already in the department, there's like a difficulty escalating it up’ (FG 4 – doctors) ‘I think people sometimes aren't aware how quickly people can actually deteriorate. Like, literally in front of your eyes. And just cause someone was fine half an hour ago, doesn't mean that that they're fine now. And also, then having the courage, to actually then go and say, hey, I'm really worried about this person, I'm not happy with them, they're deteriorating’ (FG 2 – nurses) ‘I think it's also very easy to be like, “Oh, they've had a fast resp rate and a fast heartrate since triage”, they're just staying on that trend and then maybe one other thing changes, and it's hard when you've got full rooms and like a full corridor to maybe pick up on those changes’ (FG 6 – nurses) ‘There definitely doesn't seem to be a standard approach to fluids in sepsis’ (FG 4 – doctors) ‘We are holding off vasopressors and other treatments, and then suddenly we are going downhill, quite quickly. Like, sometimes there is a bit of resistance to start those things’ (FG 6 – nurses) ‘Like sometimes I think there is a reluctance from doctors to like, make that decision, or there's like a kind of tug of war between ICU and whether that referral is made’ (FG 5 – nurses) ‘…trying to look after this woman who like we can't do some things for, because like we can't get IV access, and it took us half an hour to get IV access, and so then it like slows down everything else’ (FG 6 – nurses) ‘Sometimes it's hard with more junior staff. I think that they cause sometimes they'll like see the patient, then they'll sit on them quite a long time before they get a chance to talk to the consultant, or get a chance to follow up. Sometimes they're not as fast as escalating as some more senior doctors’ (FG 6 – nurses) 2.2 Factors the ED cannot control ‘…maybe possibly a code 2 in one room, then a code 3 sepsis in the other room. Like, the acuity of the department, and you might have two corridor patients on top of that’ (FG 5 – nurses) ‘…if the doctors are busy with other unwell patients, it can cause problems getting that patient seen in a timely manner’ (FG 6 – nurses) ‘…they're clearly septic, and they've been in the room for x amount of time, and you know there's only two doctors on a night or whatever, and it's not done – nothing is done’ (FG 3 – doctors) ‘They're in the department, and usually, especially the medical doctors, they are horrifically overrun’ (FG 6 – nurses) ‘…and then you're reliant on the specialties, and they take ages to come down’ (FG 3 – doctors) ‘It's usually the medical staff, they're busy, but they don't always seem that supportive when your patient's deteriorating. And then it – you're in a really awkward position, because then if they're not coming, I'll talk to whoever's around, so the ED staff, but that's not really their patient any more, and it's just kind of a little bit difficult to know like who's listening’ (FG 2 – nurses) ‘Sometimes with the sepsis patients, if they've referred to specialties, ED can at times be a little hands off’ (FG 2- nurses) 2.3 Patient factors ‘So someone's had a collapse, and an injury, you get caught up with treating the injury, and you can miss the sepsis there’ (FG 1 – doctors) ‘Especially in like an English-centric focus, and a patient who speaks … any other second language, they're not going to be able to vocalise their concerns as much, or try and advocate for themselves as much. And so that definitely impacts on how they get triaged, treated, referred. So definitely trying to be a bit more inclusive of other languages in the department’ (FG 4 – doctors) ‘It can be difficult getting a history if the sepsis is causing any confusion, or is it because they've got underlying dementia for example. Or they're just too unwell to explain what happened’ (FG 1 – doctors) ‘The whole health system in New Zealand is set up to be inequitable. It's not set up for Māori’ (FG 3 – doctors) ‘I think being more aware of that. Because then you probably drill down deeper, particularly at places like triage, to try and find out enough so you have got the evidence to prioritise their care. Or do we need to make that another factor in our sepsis assessment process, so that we can say, you know it's an added … like, criteria for likely sepsis. Māori, Polynesian … whoever else is in the risk groups’ (FG 5 – nurses) 3.0 Communication 3.1 Patient, family and whanau ‘I don't know if they understand it in relation to sepsis, as such. They just understand that someone's very unwell, because they have an infection’ (FG 2 – nurses) ‘I say blood infection as well as a local infection if I'm referring, rather than using the word sepsis I think. It's a bit more of an accessible phrase’ (FG 3 – doctors) ‘I think sometimes it's easy to become distracted by the tasks that you're doing. And your patient's family is asking you a question … but you don't really focus on what you're really saying to the patient. Because you're like, right, I've got to do my line, I've got to do my bloods, got to put out these antibiotics, I've got like – let's get these fluids into them, because they're super hypertensive. But actually just stop and processing what your patient's family is saying is really important, so that you can give them an answer they will understand. Instead of just like brushing it off or giving a very quick answer. Cause otherwise the family's going to panic more, and the patient’ (FG 2 – nurses) 3.2 Documentation and clinical systems ‘I think something that's done really poorly, and I've experienced multiple times is that the medical team will come and review a patient, and they'll chart an additional or an alternative antibiotic that they want to be given, but they don't make you aware of that. And it might not be until you've got an opportunity to like, look through your charts, or look through the notes on EDIS [ED documentation system] and the admission note and see that they've made a change’ (FG 5 – nurses) ‘Also it's happening more frequently that they don't write anything on anywhere. So there's nothing on EDIS, there's nothing on Concerto [electronic medical record system], and they've gone up to the ward and not spoken to whichever nurse is supposed to be looking after – so then you're wasting time. That's a big waste of time. And then you've got to plough through the roster, and – you know like, columns and columns on the doctors' roster, oh which one do I contact?’ (FG 5 – nurses) 3.3 Interdisciplinary and between specialties ‘But generally the doctors are pretty good at trusting what we're saying to them’ (FG 6 – nurses) ‘Quite often the ED doctors are really good at coming and being like, “I know that they're going to medicine, but is there anything you need in the meantime”’ (FG 6 – nurses) ‘I had a young guy sitting in the corridor for four hours on a nightshift, and a very astute patient flow nurse walked past and was like “Oh, he looks a bit grey”. He had a CRP [blood marker of infection] of 300 and a necrotic foot under his sheet’ (FG 3 – doctors) ‘It's actually harder finding the specialty doctor. Cause the ED doctors are there. And it might take another 10, 15 minutes for them to come down from the ward’ (FG – 5 nurses) ‘It's a really tricky grey zone, because I appreciate the medical staff do have such a workload that they have to just sort of tick off, tick off and then it gets interrupted by an unexpected event’ (FG 2 – nurses) Clinical managementThis theme provides contextual details around current management of sepsis patients within the study site ED. These factors are expressed through multiple sub-themes: ‘recognition of sepsis’, ‘auxiliary resources’ and ‘triage’.
Early recognition of sepsisParticipants highlighted that early recognition of sepsis was a key factor in successful clinical management leading to better patient outcomes.
‘Yeah, I think recognition is the most important thing for sepsis that's treated well’ (FG 1 – doctors).
Furthermore, it was rare for a patient to deteriorate unexpectedly following review by a senior clinician.
Auxiliary resourcesThe use of auxiliary resources such as the local sepsis pathway and locally developed Empiric app for antibiotic selection, were beneficial to clinicians. The pathway empowered nurses to prioritise tasks and advocate for management decisions.
‘On a very busy day, with the protocol there, it was quite quick to make sure everything was checked off and not missed’ (FG 2 – nurses).
The Empiric app was commended for providing area-specific sensitivity information and promoting antibiotic stewardship.
TriageIt was acknowledged how difficult the crucial role of triage is and how challenging it is to identify sepsis within the short timeframe available for assessment. Sepsis lacks a cardinal marker so it can be difficult to determine who needs higher acuity codes. Nurses described difficulties differentiating between the appropriate Australasian Triage Scale codes for patients with sepsis, who fall between a code 2 (treatment acuity 10 min) and code 3 (treatment acuity 30 min).
‘So we've got that triage code 2, code 3, which separates … the degree of sepsis, but everything's a continuum. So you'll have people that are almost a 2, but not quite maybe’ (FG 5 – nurses).
Challenges and delaysVarious challenges and delays to clinical care and ongoing management of sepsis patients were identified. This was the largest theme from the study, and is divided into the sub-themes ‘factors the ED can control’, ‘factors the ED cannot control’ and ‘patient factors’.
Factors the ED can controlEscalating care for patients with sepsis proved to be a challenge for both ED doctors and nurses. For doctors, escalating care in those initially triaged as lower acuity that deteriorated and required a higher acuity area, such as resus, was an issue. The nurses reported difficulties noticing subtle downward trends of vital sign observations, particularly when ED was busy or overcrowded.
‘I think it's also very easy to be like, “Oh, they've had a fast resp rate and a fast heartrate since triage”, they are just staying on that trend and then maybe one other thing changes, and it's hard when you have got full rooms and like a full corridor to maybe pick up on those changes’ (FG 6 – nurses).
The doctors reported feeling stressed due to the lack of clear consensus regarding treatment options such as intravenous (IV) fluid volumes, vasopressor use and admission criteria to the ICU.
‘You know … a lot of septic patients are flooded with multiple litres before considering other treatments’ (FG 4 – doctors).
This was noted to delay management decisions, particularly among more junior clinicians. Delays to IV access also impeded prompt administration of fluids and antibiotics.
Factors the ED cannot controlDepartmental overcrowding due to hospital bed block and high patient volume adversely affected patient flow and care of patients with sepsis.
‘I just think mostly when it's not going well, it's when you've got a very high workload. Like that's – basic … it's always going to be hard’ (FG 6 – nurses).
These factors prevent patients being brought into ED cubicles from the waiting room or patients are assessed in ED corridors; lacking privacy, dignity and limiting thorough assessment. These issues are augmented at night when staffing levels are further reduced.
There can be disputes regarding responsibility of management decisions among patients with sepsis who are under or awaiting care from specialty teams.
‘…which suggests that it's a case of different teams getting confused over who's going to take responsibility for the patient’ (FG 5 – nurses).
This adversely affected the nursing team who reported being unsure who to escalate their concerns to. Specialty doctors have other competing priorities and workload demand that can also delay care.
Patient factorsMultiple factors centred on the heterogeneity of patients who present with sepsis. Presentations of the young and old were challenging, and often in the aged, confounded by comorbidities and multiple or unclear complaints. It was also challenging when patients did not present with ‘classic’ symptoms of sepsis.
‘Like, I've got a patient at the moment who is septic, but she's got so much stuff going on that, there's just too much, like the sepsis is kind of a small part of it’ (FG 6 – nurses).
Communication barriers for patients for whom English was not their first language made assessment challenging for clinicians. There was an awareness that these patients were less able to communicate their needs and presenting features.
Equity of care for patients was a key theme noted in all focus groups. All participants acknowledged the disparities in health outcomes between Māori and non-Māori in NZ. Regarding sepsis, participants perceptions were that Māori patients presented later and with increased severity of illness. There were concerns for a lack of awareness among fellow clinicians of the increased risk Māori patients have with regards to sepsis, impacting triage decisions.
‘Had a Māori man in his 50s who had Type 2 diabetes, and presented with a red leg. And was like was a triage like 4 or 5. And no one even thought to do a temperature. And he was crashingly septic in the waiting room for like four hours, overnight, you know’ (FG 3 – doctors).
Participants had suggestions for improving care, such as adding ethnicity as a risk factor to the current sepsis pathway.
CommunicationThe final theme highlights how communication can affect the management of patients with sepsis. This theme is divided into the sub-themes: patient and family/whanau (Te Reo Māori-language for extended family); documentation and clinical systems; and interdisciplinary and between specialties.
Patient and family/whanauED clinicians had an aversion to using the term ‘sepsis’ when talking to patients and their families, based upon an assumption that the term is not understood outside of the medical profession.
‘I don't feel like the word sepsis really means much to most family members. I think words like bad infection usually gets through a bit quicker. The only thing I think is tricky is communicating how unwell somebody is sometimes. Explaining that it's quite a significant illness to have’ (FG 1 – doctors).
Communication to patients and their families can have an additional layer of complexity due to the sometimes time-critical interventions necessary for the very unwell.
Documentation and clinical systemsNurses were concerned about poor documentation and communication of patient management plans leading to delays in care. For example, written antibiotics prescriptions not being communicated by the prescriber or the lack of documentation of management plans in the EDIS system. The latter requiring nurses to make time-consuming follow-up phone calls to specialty teams.
Interdisciplinary and between specialtiesIn general, participants reported positive interactions and mutual collegial respect between ED nurses and doctors. Communication with specialties outside ED was more challenging due to issues with internal communication systems such as finding the correct phone number. There was an appreciation that this was also impacted by workload demand of specialty teams.
‘…but I think sometimes communication's lacking a little bit, because they're – the medical staff are so time pressured as well to go on and review the next patient’ (FG 5 –nurses).
DiscussionSepsis continues to be one of the leading causes of morbidity and mortality in hospital; but the majority of this is preventable with early recognition and timely care.18 Few studies exist that explore what ED nurses and doctors experience when caring for patients with sepsis. This qualitative study identified three key themes regarding factors that affect sepsis care in ED: clinical management, challenges and delays and communication. The results highlight the important and often complex interactions of clinical, systemic and organisational structures. Early recognition of sepsis undoubtedly leads to better outcomes for patients.1, 3, 19 There are inherent challenges with regards to identifying patients with sepsis in the ED environment promptly and efficiently.20, 21 Primarily, a large variety of pathogens underlie patient's conditions and clinical presentations.2 This is confounded by patients who are poor historians, have multiple co-morbidities or have atypical symptoms, as highlighted in our study and other literature.12, 22
Triage was noted to be the most difficult task facing ED nurses. It may not always be possible to diagnose sepsis at triage.20 More detailed assessment may be first required, or patients may progress to sepsis or septic shock during their ED or hospital stay. A study in 2015, conducted prior to the introduction of the sepsis 3 definition, noted that the Australasian Triage Scale system only leads to moderate accuracy and moderate agreement between nurses regarding sepsis identification.21 Furthermore, patients triaged to lower acuity treatment areas face a significant delay to antibiotic treatment.23 Therefore, this may be an area to focus quality improvement and nurse education strategies. A qualitative study exploring ED nurse perceptions and experience recognising sepsis in an Australian ED also highlighted the important role nurses have with regards to sepsis recognition, particularly at triage. The authors advocated for the development of nurse inclusive sepsis pathways in ED.11
Having a clinical pathway for sepsis was highly valued by clinicians. Nurses reported feeling empowered by the pathway enabling them to prioritise tasks, promptly care for patients and highlight when to escalate care. The introduction of a locally developed antibiotic guideline smart-phone application (Empiric) was seen to foster better antibiotic stewardship and reduced antibiotic decision time for doctors. Another qualitative study published recently supports the use of clear evidence-based clinical pathways in ED.12
Currently in NZ, the New Zealand Sepsis Trust (NZST) and Best Practice Advocacy Centre New Zealand have localised some of the UK NICE sepsis pathways.24 The NZST has recently drafted a New Zealand Sepsis Action Plan,25 and ED recognition and management is a key strategic focus area. Clearer consensus regarding fluid and vasopressor use are coveted; the ARISE study group are currently conducting research aiming to address this.26 Other qualitative studies in ED advocate for nurse initiated fluid treatment in sepsis,22 particularly in busy environments. Such strategies warrant further clinical review but could in future be included in sepsis pathways.
Difficulty recognising deterioration when workload demands are high, particularly regarding vital signs, was a key finding in the present study. Patients with sepsis are a cohort with one of the highest risks of unrecognised deterioration.21 Evidence demonstrates that high patient load, particularly of high acuity patients, and patient flow demands, impede the ability of nurses to recognise sepsis.
留言 (0)