
記住我
Japan is experiencing both an ageing population and a decline in birth rate that is unparalleled in the rest of the world. It is estimated that the elderly (< 65) made up 27.7% of the population in 2017.1, 2 Japan can be said to be faced with a ‘super-ageing’ society. Along with the rapid ageing of society, the number of people with dementia has increased.3 A similar trend is being seen in other countries, particularly in developed countries. In 2015, an estimated 47 million people were living with dementia worldwide, and this number is projected to triple by 2050.4
Alzheimer's disease (AD), which is the most common cause of dementia, is an incurable and progressive neurodegenerative disorder. At present, AD cannot be treated completely, although several medications such as acetylcholinesterase inhibitors can slow the disease's progression. In addition to pharmacotherapy, nonpharmacologic therapy is a potential pathway for treating dementia.5 People with dementia may benefit from nonpharmacologic approaches, including cognitively engaging activities, physical exercise and socialisation.6 However, as with pharmacotherapy, nonpharmacologic therapy cannot cure dementia. Consequently, there is an increasing need to prevent dementia, and many municipalities in Japan have launched a dementia prevention program (DPP).7 Effective dementia prevention strategies would provide substantial benefits by improving quality of life, prolonging independent life expectancy and reducing economic costs and social burdens.8
Multiple potential risk factors, such as depression, cardiovascular and cerebrovascular disease, diabetes, cognitive function, physical function, self-rated health and lifestyle characteristics, are reported to be associated with the incidence of dementia.8, 9 Thus, the incidence of dementia can be reduced by exercising moderately in daily life to prevent lifestyle diseases. An important purpose of the DPP is to help the elderly understand the factors associated with the incidence of dementia and to live a daily life that carries less risk of developing dementia.
Although efforts to prevent dementia have grown popular over time, there are no proven modalities for preventing dementia.10 In 2016, Kobe City held a dementia prevention class for citizens in each city ward. Each class consisted of six programs. Other municipalities adopt a similar method, holding programs once or twice a week for approximately 10 days, after which the programs cease. Because dementia, particularly AD, is a neurodegenerative disease that progresses over the long-term, adopting a long-term approach to prevent and treat the disease is desirable. However, to continuously manage a DPP for a large number of citizens, a municipal office requires a large budget and significant human resources. Ideally, a DPP should be run more efficiently with limited resources.
In this study, we conducted intensive interventions for all participants and divided them into a booster training group (BTG) and a non-booster training group (NonBTG). Then, we compared the cognitive and physical function changes between the two groups. Many previous intervention studies on dementia prevention compared the cognitive function changes between an intervention group and a non-intervention group, but they did not compare the changes after conducting a common intensive DPP in all participants. The main aim of this study is to clarify the following two points: (i) short-term effects of intensive training (once a week for 10 sessions); and (ii) longitudinal effects of regular booster training (once every 3 months) following intensive training and conducted over a 2-year period.
METHODS ParticipantsThe sample population comprised community-dwelling elderly aged at least 70 years who were flagged as being at high risk for mild cognitive impairment (MCI)/dementia because of unfavourable answers on the cognitive domain of the ‘Kihon Checklist’ in 2015 and consequently participated in a dementia prevention education program organised by Kobe City in 2016. The Kihon Checklist, which has been developed by the Japanese Ministry of Health, Labour and Welfare, is a simple 25-item questionnaire used to identify frail citizens, and includes three items (Q18–20) on subjective cognitive function (the cognitive domain).11, 12 We deemed participants in the current study to be at risk for future dementia. We excluded from the study subjects who had been diagnosed with dementia by a medical doctor, in addition to subjects with obvious dementia symptoms (Mini-Mental State Examination (MMSE) score of ≦ 23 at baseline evaluation), mental disorders and severe motor disabilities. We also excluded subjects who were absent from more than three intensive training sessions out of 10 and subjects who did not receive booster training every 3 months in the BTG.
Study settingThe baseline assessment of cognitive and physical function for 57 elderly participants included the following elements: an MMSE, Five Cognitive Tests (Five Cog), a Cognitive Function Instrument (CFI), a Timed Up & Go Test (TUG), a grip strength evaluation, a Geriatric Depression Scale (GDS), an EQ-5D, and a Physical Activity Scale for the Elderly (PASE). The intensive training program was conducted for 2 h per week for 10 days. After the last intensive training, the assessment performed at baseline was reapplied. Participants were then divided randomly into two groups: a BTG and a NonBTG. The BTG received booster training once every 3 months after the intensive training period, whereas the NonBTG did not. We monitored both groups every 6 months during follow-up assessment. We conducted four follow-ups (FU-1–FU-4) over approximately two and a half years.
DPP training sessions were held in a group for 2 h at a time. We conducted the DPP once a week for 10 sessions during the intensive training period, and once every 3 months as booster training for the BTG following the intensive training. The DPP comprised physical exercise (aerobic exercise, stretching, and strength training), cognitive training, dual task training, nutrition education by a dietitian and lectures on dementia. Aerobic exercise was performed for approximately 15 min in a standing or sitting position with music, and strength training was repeated with either a light or moderate load depending on the participant's physical function in consideration of their health risks. Cognitive training included the tasks such as working memory, calculation (the four basic arithmetic operations), spotting the difference between two similar pictures and reading aloud. As dual task training, exercise and cognitive tasks were performed simultaneously, such as calculation while walking. The lectures explained the factors related to the incidence of dementia and recommended physical and cognitively engaging activities, communication with neighbours, a well-balanced diet and a moderate amount of sleep in daily life. The contents of the DPP were chosen from seemingly effective interventions for reducing cognitive decline in previous studies.13
We performed the baseline assessment in November 2017.
Statistical analysisThe Mann–Whitney U-test was used to compare the results of the assessments of the BTG and NonBTG participants at post-intensive training (PIT). To investigate the effects of the intensive training, the respective outcome measures evaluated at baseline and PIT were compared using the Wilcoxon signed rank test.
We used a linear mixed-effects model to analyse the effects of the booster training. Dependent variables were the scores of outcome measures for each assessment period (‘time’). Independent variables were ‘group’ (BTG or NonBTG) (a fixed factor) and a within-subjects factor (a variable factor). We transformed the scores of outcome measures using the Box Cox transformation. For the outcome measures for which we observed a significant interaction using a liner mixed-effects model, we conducted a pairwise comparison in each case using Bonferroni's correction. The significance threshold was set at P < 0.05. Statistical analysis was carried out by JMP®15 (SAS Institute Inc., Cary, NC, USA).
Outcome measurements The primary outcome measure for establishing effectiveness was the change of cognitive function using the MMSE score. Secondary outcome measures included the changes in Five Cog, CFI, TUG, grip strength, GDS, EQ-5D and PASE. Details of the outcome measures are as follows. The MMSE14 can be used to assess mental status both systematically and thoroughly. It is an 11-question measure that tests five areas of cognitive function; these are orientation, registration, attention and calculation, recall and language. The maximum score is 30. A score of 23 or below is indicative of cognitive impairment. The Five Cog15 was developed especially for older Japanese adults as a screening instrument to detect cognitive decline. It is a group assessment tool for cognitive functions that consists of five subtests (attention, memory, visuospatial, language and reasoning). A high score indicates better functioning. The CFI16 is a screening tool for detecting early changes in the activities of daily living arising from cognitive decline. It comprises 14 questions that are related to reduced functional ability arising from cognitive impairment. The CFI score is calculated by ascribing 1 point for ‘Yes’, 0 points for ‘No’ and 0.5 points for ‘Maybe’. The CFI questionnaire includes ‘self’ and ‘partner’ versions; this study uses the ‘self’ version. The TUG17 is a simple test used to assess a person's mobility and it requires both static and dynamic balance. It measures the time that a subject takes to rise from a chair, walk three metres, turn around, walk back to the chair and sit down. The GDS18 is a screening test that is used to identify depression symptoms in older adults. The scale is a self-reported instrument that adopts a ‘Yes/No’ format on a short form containing 15 questions. EQ-5D19 is a standardised measure of health status developed by the EuroQol Group to provide a simple, generic measure of health for both clinical and economic appraisal. It can be applied over a wide range of health conditions and treatments. The EuroQol Group provides two versions of the EQ-5D with either three or five dimensions; for this study, we used the latter (EQ-5D-5L), which comprises five categories with five questions in each category. Depending on the pattern of answers, an individual's health status is given either as a single index value, ranging from zero to one, or death to perfect health. This study used only a single index value for statistical analysis. 7)The PASE,20 which is easy to administer and score, measures the level of physical activity in people aged 65 years and above. The instrument consists of self-reported occupational, household and leisure activity items over a period of 1 week. The present study used the total PASE score. We measured grip strength of the dominant hand of the participant in kilograms by using a Smedley-type handheld dynamometer (GRIP-D; Takei Scientific Instruments Co., Ltd., Japan). Ethical considerationOur study protocol was approved by the ethics review committee of Kobe Gakuin University and the WHO ethics committee (ERC.0002899). The study was carried out in accordance with the provisions of the Declaration of Helsinki and Japan's ‘Ethical Guidelines for Medical and Health Research Involving Human Subjects.’
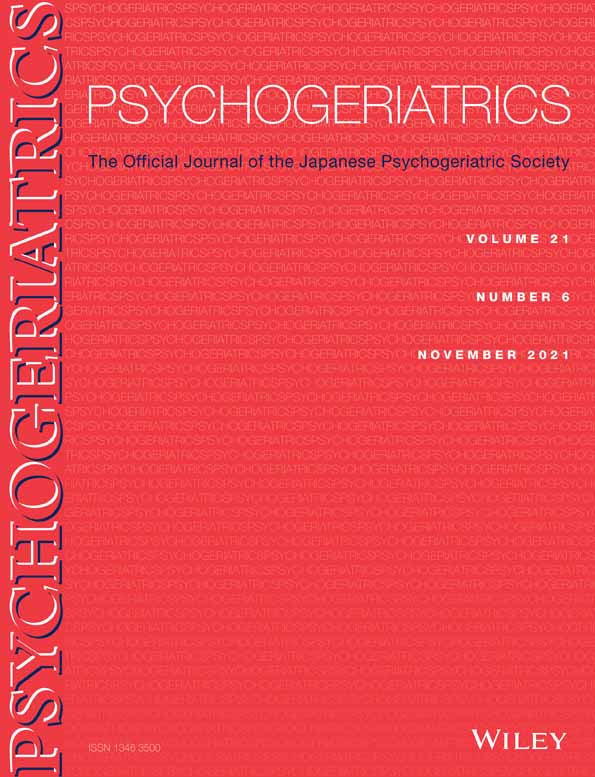
RESULTSThis study involved 57 participants (21 male, 36 female) who underwent 10 sessions of intensive training. The mean (SD) age of the participants was 76.4 (2.7) years, and the mean years of education were 12.0 (2.3) years. We excluded from the project subjects who missed the intensive training three or more times. Forty-nine participants received PIT assessment. We randomly assigned 25 participants to the BTG and 24 to the NonBTG. Sixteen participants dropped out during the follow-up period, and the eventual number of participants at the FU-4 assessment was 16 (6 male, 10 female) in the BTG and 17 (6 male, 11 female) in the NonBTG. The chief causes of the dropouts were personal matters and hospitalisation due to poor physical conditions (Fig. 1). The mean ages of the BTG and the NonBTG participants were 75.8 (3.2) years and 76.6 (2.4) years, respectively. There were no significant differences between the two groups in age (P = 0.39) and measurement results (Table 1).

Study overview, showing the change in the number of participants in this study. BTG, booster training group; NonBTG, non-booster training group; PIT, post-intensive training; FU-1, follow up 1; FU-2, follow up 2; FU-3, follow up 3; FU-4, follow up 4.
Table 1. Assessment result of the post-intensive training in the BTG and the NonBTG BTG (n = 16) NonBTG (n = 17) Z score P-value MMSE 28 (26.3–29.0) 28 (27.0–30.0) −1.03 0.30 Five Cog Attention 29 (24.3–33.0) 29 (23.5–30.0) −0.33 0.75 Memory 14.5 (11.0–20.5) 17 0.0 (11.5–22.5) −0.51 0.61 Visuospatial 7.0 (7.0–7.0) 7.0 (7.0–7.0) 0.00 1.0 Language 17.5 (15.0–21.8) 16.0 (13.5–20.0) −1.24 0.26 Reasoning 12.0 (9.3–14.0) 11.0 (9.5–13.0) −0.54 0.59 CFI 4.8 (2.6–6.9) 3.5 (2.5–4.8) −1.45 0.15 TUG, seconds 6.5 (5.9–7.7) 5.7 (5.2–6.8) −1.8 0.066 Grip strength, kg 23.7 (22.4–29.1) 27.6 (21.1–32.6) −0.45 0.65 GDS 3.0 (2.3–5.5) 3.0 (1.5–5.5) −0.31 0.76 EQ-5D 0.895 (0.774–0.938) 0.895 (0.847–0.938) −0.37 0.71 PASE 115.7 (83.3–175.6) 104.8 (64.7–158.8) −0.65 0.52 Data are presented as median (25th—75th percentile). P-values are calculated using the Mann–Whitney U-test. BTG, booster training group; NonBTG, non-booster training group; MMSE, Mini-Mental State Examination; Five Cog, Five Cognitive Functions Test; CFI, Cognitive Function Instrument; TUG, Timed Up & Go Test; GDS, Geriatric Depression Scale; PASE, Physical Activity Scale for the Elderly. Effects of the intensive training and the booster trainingRegarding the tests for cognitive function, the MMSE (P = 0.047) and the subtests of the Five Cog (attention (P < 0.0001), memory (P < 0.0001), language (P = 0.035) and reasoning (P = 0.025)) showed significant improvement after intensive training. The TUG test time for evaluating physical performance also improved significantly (P < 0.0001). We did not find any improvement in CFI, grip strength, GDS, EQ-5D and PASE (Table 2).
Table 2. The effects of the intensive training Baseline PIT Z score P-value MMSE 27 (25—28) 28(26—29) −1.99 0.047 Five Cog Attention 22(19—25.5) 28(23—30) −5.49 <0.0001 Memory 12(9—15.5) 15(11—20.5) −5.31 <0.0001 Visuospatial 7(7—7) 7(7—7) −0.425 0.67 Language 15(13—17) 16(13—19) −2.11 0.035 Reasoning 11(8—12) 11(8—13) −2.24 0.025 CFI 4.5(3—6.5) 4.0(2.5—6.5) −1.63 0.10 TUG, seconds 7.2(6.4—8.1) 6.0(5.5—7.2) −5.41 <0.0001 Grip strength, kg 23.6(20.1—31.8) 23.7(20.9—30.4) −0.464 0.64 GDS 4(2—6) 3(2—6) −0.132 0.90 EQ-5D 0.895(0.8075—0.895) 0.895(0.815—0.9384) −0.639 0.52 PASE 127.7(68.3—157.0) 113.9(79.8—168.0) −0.84 0.40 Data are presented as median (25th—75th percentile). P-values are calculated using the Mann–Whitney U-test. PIT, post-intensive training; MMSE, Mini-Mental State Examination; Five Cog, Five Cognitive Functions Test; CFI, Cognitive Function Instrument; TUG, Timed Up & Go Test; GDS, Geriatric Depression Scale; PASE, Physical Activity Scale for the Elderly.Our analysis of the effects of the booster training revealed no additional significant differences in most of the outcome measures. Although there was a significant interaction in the CFI (P = 0.006) and the TUG (P < 0.0001) (Table 3), the pairwise comparison did not reveal any significant differences.
Table 3. The effects of the booster training Mixed effect model Baseline PIT FU-1 FU-2 FU-3 FU-4 Group Time Interaction MMSE BTG 27.2 (1.9) 27.5 (1.9) 28.3 (1.3) 28.3 (1.5) 28.2 (1.5) 27.6 (1.6) 0.71 (0.17) 0.97 (0.0055)0.92
(0.020)
NonBTG 27.4 (1.7) 28.2 (1.7) 28.2 (1.6) 28.4 (1.7) 27.8 (2.3) 28.5 (1.8) Five Cog Attention BTG 24.2 (5.9) 27.9 (5.2) 25.8 (7.1) 24.8 (7.2) 24.6 (5.9) 24.6 (7.9) 0.62 (−1.0) 0.001 (−0.73)0.86
(−0.05)
NonBTG 20.4 (7.7) 27.1 (5.1) 23.8 (6.2) 25.2 (6.6) 23.8 (6.0) 23.3 (5.8) Memory BTG 13.3 (4.5) 15.9 (6.1) 16.1 (5.9) 17.2 (7.1) 17.1 (7.1) 17.7 (7.4) 0.83 (0.52) 0.010 (0.44)0.20
(−3.0)
NonBTG 13.1 (5.2) 16.5 (6.8) 16.7 (7.1) 16.7 (6.9) 16.6 (7.4) 17.3 (6.9) Visuospatial BTG 6.9 (0.34) 6.9 (0.25) 6.9 (0.25) 6.9 (0.25) 6.9 (0.25) 6.9 (0.25) 0.084 (−0.18) 1.0 (<0.001)0.087
(0.070)
NonBTG 6.7 (0.59) 6.6 (1.7) 6.8 (0.44) 6.9 (0.24) 7 (0) 7 (0) Language BTG 16.8 (2.4) 18.4 (4.2) 16.8 (3.2) 18.0 (3.7) 18.6 (4.1) 18.3 (3.5) 0.51 (−0.96) 0.45 (0.14)0.93
(0.023)
NonBTG 16.5 (4.2) 16.6 (4.0) 16.8 (4.2) 17.7 (5.3) 18.1 (5.8) 17.2 (5.7) Reasoning BTG 10.2 (3.2) 11.6 (2.5) 10.9 (2.5) 11.1 (3.1) 10.9 (3.0) 10.9 (3.1) 0.81 (0.22) 0.24 (−0.13)0.79
(−0.04)
NonBTG 11.4 (2.7) 11.3 (2.5) 11.8 (2.6) 11.5 (2.4) 10.9 (2.8) 10.8 (2.9) CFI BTG 5.1 (2.9) 5.2 (2.6) 4.2 (2.4) 4.3 (2.3) 4.3 (2.7) 4.2 (2.2) 0.22 (−0.89) 0.085 (−0.17)0.006
(0.39)
NonBTG 4.9 (2.2) 3.8 (2.2) 4.1 (2.0) 4.4 (1.9) 4.4 (2.1) 4.7 (2.0) TUG, seconds BTG 7.8 (1.4) 7.0 (1.6) 7.4 (1.3) 7.0 (1.4) 6.8 (1.5) 6.5 (1.3) 0.034 (−0.98) 0.005 (−0.15)0.000
(0.30)
NonBTG 7.1 (1.4) 6.0 (1.3) 6.9 (1.7) 6.6 (1.5) 6.8 (1.7) 6.8 (1.7) Grip strength, kg BTG 25.0 (6.3) 25.4 (5.3) 24.4 (6.1) 24.1 (5.9) 24.2 (5.5) 24.7 (5.5) 0.29 (2.3) 0.17 (−0.16)0.15
(−0.24)
NonBTG 27.3 (7.7) 27.6 (7.6) 26.9 (7.5) 27.2 (7.3) 26.0 (7.5) 26.1 (7.6) GDS BTG 4.7 (3.7) 4.2 (3.0) 4.9 (2.6) 3.1 (2.6) 4.4 (3.3) 3.6 (3.6) 0.36 (−0.77) 0.032 (−0.25)0.089
留言 (0)