
記住我

The fact that generic drugs are typically not required to contain the same inactive ingredients as the branded product raises the possibility of differences in the safety and efficacy profiles of the branded and generic drugs related to differences in the formulations.19 This issue has been addressed in multiple large-scale claims and meta-analyses, the results of which indicated similar clinical outcomes for branded and generic agents across a wide range of disease states.11, 12, 20-23
Despite the large body of evidence demonstrating equivalent efficacy and safety for branded drugs and their generic counterparts, some patients and providers have the perception that generics may be less safe and effective than branded agents.24 Negative expectations regarding generic products may lead to negative clinical outcomes due to a complex neurobiological phenomenon often described as the nocebo effect.11, 24-26 A remarkable demonstration of this phenomenon was provided by Faasse and colleagues.27 In their study, 62 university students were recruited to purportedly test the effectiveness of fast-acting β-blocker medications for reducing pre-examination anxiety. All tablets were placebos and were the same size. In session 1, all participants received a yellow tablet (‘‘Betaprol’’). In session 2, participants were randomly allocated to receive Betaprol (no change) or a white tablet labelled either as ‘‘Novaprol’’ (branded change) or ‘‘generic metoprolol’’ (generic change). Blood pressure and state anxiety were measured before and after tablet ingestion. Patients experienced reduced effectiveness and increased medication-related side effects when changed from a branded medication to a drug labelled as a generic.27
Patient and provider concerns regarding the efficacy and safety of generic medications may arise, at least in part, from results of generally small-scale studies that have demonstrated differences in the efficacy and safety of branded and generic agents, most often for agents with a narrow therapeutic index (NTI), such as antiepileptic drugs.28, 29 In addition, for some higher-risk patients with complex needs, generic substitution may lead to decreased compliance, poorer treatment outcomes, increased resource utilization and higher overall cost of care.30
Patient perceptions about generic agents have the potential to adversely affect adherence to therapy and treatment outcomes. For example, 73% of 106 patients taking atypical antipsychotics questioned in a hypothetical pharmacy setting stated they would probably not take their medication if it had been substituted with a generic by their pharmacist.31 Results from analysis of a large claims database indicated that patients with hypertension, switched from branded valsartan to another generic angiotensin receptor blocker, had significantly decreased adherence.32 It is important to note that decreased adherence to therapy after switching treatment may also occur after switching among branded medications. A retrospective observational analysis of 38,866 new statin users who switched from one branded statin to another was less adherent to treatment by 19% and less persistent by 21%–48%.33
The following sections discuss the nine publications identified in the literature search that focus on AGs with respect to medical and health outcomes of therapy as well as switching between brands and generics. The first section is specific to comparative outcomes with 3 subsections on effectiveness and clinical outcomes, usage patterns and outcomes and safety. The second section highlights the available information related to switchbacks from AGs and other generics to branded medications.
3.2 Comparative outcomes 3.2.1 Effectiveness and clinical outcomesAssessment of clinical responses and persistence with generic medications may be negatively impacted by patient perceptions regarding these products.34 AGs can be used in order to control for negative perception bias in studies comparing generic vs branded drugs. For example, this approach was employed by Desai and colleagues, who directly compared the effectiveness of branded and generic versions of eight different drugs using two large population-based sources and a comparison of branded vs AG versions of the drugs as the negative control.11 Data were included from more than 3.5 million patients in two large US commercial insurance databases who were prescribed either alendronate tablets (osteoporosis), amlodipine tablets (hypertension), amlodipine-benazepril capsules (hypertension), calcitonin salmon nasal spray (osteoporosis), escitalopram tablets (depression and anxiety), glipizide extended-release tablets (diabetes), quinapril tablets (hypertension) or sertraline tablets (depression and anxiety). Drugs included (1) products for which generics entered the market after 2003 (the start of data availability from the sources used); or (2) products for which generics and AGs entered the market concurrently; or (3) a combination product (amlodipine-benazepril capsules).11 The effectiveness end points for the different agents included in the study were a composite cardiovascular outcome (hospitalization with myocardial infarction or ischaemic stroke or coronary revascularization) for amlodipine, amlodipine-benazepril and quinapril; non-vertebral fracture for alendronate and calcitonin; psychiatric hospitalization rate for sertraline and escitalopram; and insulin initiation for glipizide.11 Results from this investigation suggested that clinical outcomes with the use of generics and brand products for serious chronic conditions were broadly equivalent, with observed differences that might potentially be due to perception bias.11 However, this very large-scale study was not without limitations, which included potential residual confounding due to the unavailability of certain clinical parameters in administrative claims data and the inability to evaluate surrogate outcomes, such as immediate changes in blood pressure, upon switching from branded products to generics. In addition, although potential problems with efficacy and/or safety have been of concern for NTI drugs, no such agents met the study inclusion criteria.11
3.2.2 Evaluation of usage patterns and health resource utilizationHansen et al carried out a retrospective cohort study that compared brand-to-generic switching patterns and outcomes for AGs and generic drugs to determine whether there were differences in drug utilization patterns and indicators of health resource utilization that could be attributed to differences in therapeutic equivalence between drug products.12 A comparison between AG and generic users indirectly represents a brand vs generic comparison after controlling for drug perception bias. Alendronate, amlodipine, citalopram, gabapentin, paroxetine, sertraline and simvastatin were included in the analysis; and across these seven drugs, 5,234 unique individuals and 5,544 unique person-drug combinations were identified. Across all drugs pooled, results from patients using AGs were similar to those for patients taking generics with respect to outpatient visits, urgent care visits, hospitalizations and medication discontinuation, but the likelihood and number of emergency department (ED) visits were slightly higher for AGs vs generics.12 It is possible that inactive ingredients used in the generic agents might have had a better safety profile than those employed in the AG formulations. It is also possible that there may have been differences in the characteristics of patients who received AGs vs generics despite the fact the study design controlled for patient-related factors and pre-index health services use.12 An exploration of results for individual drugs indicated that the higher probability and number of ED visits for AGs vs generic drugs was driven by alendronate and sertraline. In contrast, ED visits for the AG of simvastatin were lower than those for patients who received the generic. Although these results indirectly support similar outcomes for generics compared with brand drugs, they emphasize the importance of cautious interpretation of pooled data and suggest that future evaluations should consider products individually and that the observed differences between AGs and generics are worth continued exploration.12
3.2.3 Safety considerationsDifferences in adverse events between brand and generic medications have been specifically evaluated in several studies. An analysis of adverse events reported to the FDA for branded agents, generics and AGs for amlodipine, losartan, metoprolol extended-release and simvastatin during the period from 2004 to 2015 indicated higher rates of adverse event reports for generics vs branded agents. An interrupted time series analysis indicated that only losartan showed a significant increase in the reporting trend in the post-generic period (p = 0.0001). There were fewer statistically significant differences when AGs were used as controls, although this approach may be explained by the smaller number of AG reports. In this analysis, only the reporting odds ratio (ROR) for AG vs generic amlodipine with peripheral oedema was statistically significant (p = 0.004). It should be noted that this study included only cardiovascular drugs. In addition, the FDA Adverse Event Reporting System (FAERS) has multiple limitations. Adverse event reporting is voluntary for patients and healthcare providers, and it may be prone to reporting biases.35 This system is also limited by substantial underreporting of events and uncertainty regarding whether patients used branded or generic versions of drugs.11
The safety of branded vs generic antiepileptic drugs has been a focus of concern and a comparison among branded, AG, and generic products has also been carried out for this class. Events reported to FAERS for the period of January 2004 to March 2015 with lamotrigine, carbamazepine and oxcarbazepine classified as brand, generic or AG were compared using ROR. A total of 27,150 events with lamotrigine, 13,950 events with carbamazepine and 5,077 events with oxcarbazepine were reported, and the RORs for the majority of known adverse events were significantly higher for the generic vs branded agents (p < 0.001). In contrast, when controlling for perception bias, RORs were generally similar for AG and generic comparisons. Generic lamotrigine and carbamazepine were more commonly cited in reports of suicide or suicidal ideation compared with the respective AGs (p < 0.01).36
The results summarized in this section suggest that, in general, AGs and generics have similar safety profiles, with observed differences potentially due to perception bias. When differences in perceptions or socioeconomic status are controlled by using an AG, the performance of brand-name and generic products may be similar with respect to claims-based clinical and health service use outcomes.25 In considering the results reviewed and this conclusion, it is important to note that a limited range of medications has been evaluated and that all studies were retrospective, employing either claims or the FAERS database. In addition, the studies reviewed were not specifically designed to determine safety differences between AGs and generics.
Of note, ongoing work by Peissig and colleagues is using a novel process for evaluating brand vs generic safety and effectiveness.37 This approach is based on drug-specific, new-user, retrospective cohort studies of insurance claims and medical records. AGs are included in these analyses as brand proxies to control for perception bias. This modular approach permits drug- and event-specific adjustments in measurements and analyses and extends beyond the FAERs database to larger insurance claims databases in order to gain more extensive safety data.37, 38
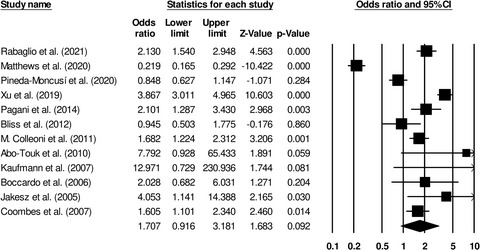
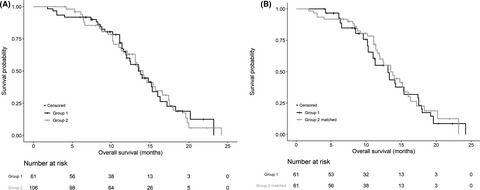
3.3 SwitchbacksSwitchbacks are an important consideration for patients who have undergone conversion from a branded medication to a generic. The impact of AGs on switchbacks was evaluated in a claims-based study that included 94,909 patients switched from branded to AG drug products and 116,017 patients that switched from branded to generic products. Switchback rates were lower, 28% and 25% in the primary and replication study cohorts, respectively, for patients switched from branded to AGs vs generics (Figure 3) (pooled hazard ratio [HR] = 0.72, 95% CI 0.64 to 0.81; HR = 0.75, 95% CI 0.62 to 0.91).39 Although it is not possible to disentangle the extent to which these results are attributable to concerns about having received the wrong medication, real pharmacological differences or other patient perceptions, these findings suggest that individuals exposed to a brand-name product experience or perceive differences between generics and AGs (brand proxy).
 Switchback analysis for the primary cohort39
Switchback analysis for the primary cohort39
Results from another somewhat smaller scale study indicated no significant difference in switchback rates to branded agents after switching to generics or AGs. This retrospective cohort study used claims and electronic health record data for the period 1999 through 2004 from a regional US healthcare system for 5,542 patients who received select branded drugs during the 6 months before their generic drug market availability and were switched to a generic (n = 5,062) or AG (n = 867) within 30 months of generic drug entry. There was no significant difference in switchback rate for AGs (8.0%) vs generics (4.2%; HR = 0.86, 95% CI 0.65 to 1.15).40 Although this study did not include as many patient-claims compared to the study by Desai and colleagues (2018), the estimates of association in the two analyses were fairly similar.
A third study specifically assessed switchback rates among patients switched from branded methylphenidate (Concerta) to either one of two generics or an AG. There were no differences among any of the products other than the external packaging. The data for this retrospective analysis came from the Truven MarketScan Commercial Claims and Encounters database from 2012. The analysis included 732 patients, of whom 124 switched from the branded agent to a generic and 608 switched to the AG. Study results indicated that 19.7% of patients in the AG arm vs 24.6% of those who switched to generics switched back (adjusted odds ratio [OR] = 1.22, 95% CI, 0.88 to 1.68). The respective rates for the combined end point of switching back to the branded drug, changing the use of immediate-release methylphenidate, stopping all long-acting methylphenidate or starting a new medication were 32.9% and 39.5%, respectively (adjusted OR = 1.23, 95% CI, 0.90 to 1.70).41
A fourth study used a retrospective cohort design to evaluate switching among patients taking eye drops used for lowering intraocular pressure. Among 7,431 patients dispensed branded latanoprost and included in the analysis, 5,969 switched to generic latanoprost, 1,514 to the original manufacturer’s generic and 4,455 to another manufacturer’s generic. Among patients who switched to the original manufacturer’s generic (ie AG), 76 switched back to brand (5%). Among patients who switched to another manufacturer’s generic product, 329 (7%) then switched back to the branded drug and 599 (13%) to the original manufacturer’s generic product. There was no statistical analysis of these results, and the reason(s) for switching back was not determined.42 The authors concluded that the substantial proportion of subjects who switched to generic latanoprost but then switched back to either the AG or branded product implies that further studies of generic substitution must address the nonpharmacological effects of this change.
The analyses summarized in this section did not distinguish between differences in actual clinical experiences with AGs or generics and differences in perceptions regarding these products. In addition, the analyses did not include any NTI agents and there have been significant concerns regarding the efficacy and safety of generic versions of such drugs.39 Nevertheless, the observed differences in switchback rates between AGs and generic products are unlikely to be fully explained by differences in quality, safety or efficacy; they may be related to negative perceptions of generic drugs.39 Thus, a potential reason for lower switchbacks to branded drugs for patients taking AGs may be due to similarity in appearance. Interventions to improve patient-provider communication aimed at increasing patient awareness regarding similarity between branded and generic drugs may be crucial for preventing switchbacks to branded drugs for these agents.39 Consistency in appearance between branded and generic drug products may also help in preventing switchbacks.39
The literature on AGs is limited, but available data clearly highlight the importance of patient perception of generics as well as medication appearance. The economic benefit of generic medications is well documented. It has been estimated that use of generic drugs resulted in a savings of $293 billion in the United States in 2018.7 Yet, although generic drug use decreases drug acquisition costs, it may not always decrease total healthcare utilization and costs.15, 30, 32, 43, 44 In some cases, there may be a misconception among patients that a less expensive medication is associated with lower quality,24 even so, some studies have demonstrated improved adherence with generic drugs compared to brand-name drugs, most probably due to lower cost.11, 25 Cost may not be the only factor that influences adherence. It is also possible that changes in the appearance of generic agents can confuse patients and adversely affect adherence to therapy.25, 45 The adverse effect of change in drug appearance on persistence has been documented in multiple studies46, 47 and drug appearance-associated reductions in adherence have also been shown to adversely affect clinical outcomes.48
AGs are typically priced only slightly higher than the lowest-priced generic. Although these lower prices may improve adherence, AGs may further have the potential to positively impact adherence due to the similarities to the brand in inactive ingredients and appearance.39 As it is plausible that there could be some differences between branded and AGs compared with generics due to such differences as inactive ingredients used by the other generic manufacturers, it is difficult to fully tease this out in the analyses which have been conducted to date. In addition to the considerations regarding adherence, AGs may provide an additional choice for patients switching to a generic treatment for a disease in which the prescribed therapy has a NTI.
In weighing prescription choices for individual patients, availability and access are important factors. AGs may not be available for all products, and although the FDA publishes a listing of reported AGs, it may not be practical for provider use, in part, because the manufacturer is listed as the NDA holder and not necessarily the associated subsidiary of the authorized generic.11 Further, product availability issues (eg marketing periods and patient access at the pharmacy) may contribute to the highly variable uptake of AGs vs generics drugs. In the past, some AGs have only been on the market for limited periods of time by the manufacturer. At the pharmacy, it is common that only a single generic manufacturer of each medication will be stocked based highly on wholesaler cost as pharmacies must balance keeping adequate inventory that can fulfil patient needs although excess inventory is returned to minimize overall stock. In addition, AGs may be reimbursed from payers the same as lower-priced generics (Maximum Allowable Cost, Federal Upper Limit, etc.).12 This lowers pharmacy gross margins and may be a disincentive to dispensing of AGs when other generics are also available. Future payer tiering of AGs may increase access to these products, possibly at a higher cost.
In addition to the factors above that lend to the complexity of access to AGs, there is also need for more information and research regarding the use of AGs in clinical practice. There is a lack of awareness about potential differences between AGs and generic drugs.9 Particularly important broad targets for educational interventions include increasing the knowledge of interchangeability criteria between generic and brand-name drugs, as well as addressing physicians’ and patients’ negative perceptions of generics. Additionally, gaps that should be filled by new studies include analyses aimed at understanding reasons for different switchback rates for AGs vs generics, including switching from generics to branded agents among patients having no prior experience with the branded drug; and the impact of switchbacks on patients and the healthcare system (ie cost of switchbacks). Laroche and colleagues evaluated the economic impact of switchbacks from generic to brand name allopurinol in France, and their results prompted the conclusion that they had only a weak economic impact on reimbursement cost for the French health insurance system.49 It would be useful to have corresponding information for the United States that includes AGs. There is also a need for research focussed on patients’ perspectives and outcomes (clinical end points or surrogates) and analyses of individual product differences among brands, AGs, and generics for outcomes, such as adherence to therapy. Some additional insights regarding AGs might be gained via active surveillance with the recently developed FDA Sentinel System.25, 50
It is important to acknowledge potential limitations of a narrative vs a systematic review for addressing the issues considered in this paper. It is often noted that narrative reviews lack explicit criteria for article selection and that this creates a risk for bias. We have addressed this by clearly stating literature search criteria and the citations recovered. All of the papers included in the Results section were recovered from the searches described. References cited in other sections were selected to provide context for the results described. We believe that adhering strictly to the criteria for a systematic review would not have permitted provision of this framework for the studies described.
The current US healthcare environment is complex, and prescription medications continue to be a key topic in the conversation about reducing healthcare costs, while recognizing the importance of drug quality, and ensuring consistent supply.51
留言 (0)