
記住我


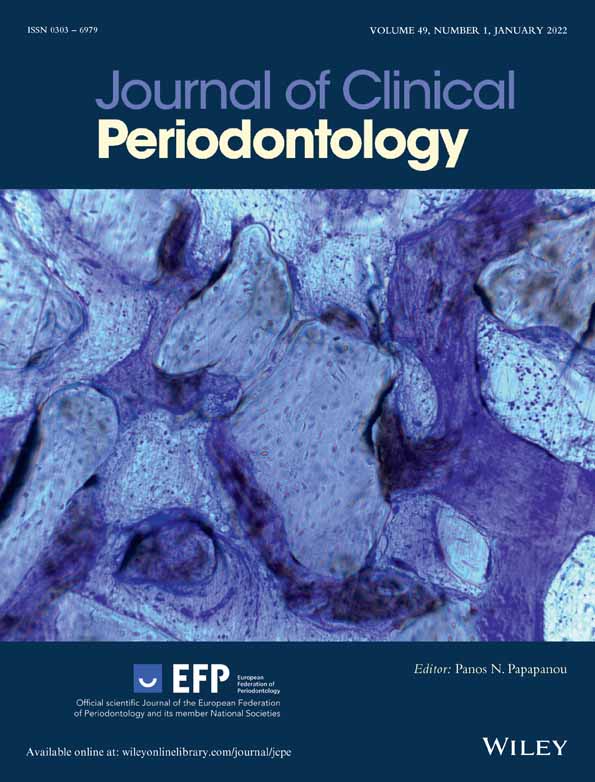
A total of 1515 records were identified through searching electronic databases after duplicates were removed (Figure 1). No additional records could be identified through other sources, including hand search. After structured screening of titles and abstracts, 1464 articles were excluded, and the examiners reached an accordance of 95% with kappa score 0.89 (Landis & Koch, 1977).
 Selection process for the studies included. Procedure applied in the study: *s-splinting, ¤o-occlusal adjustment, ‡so-splinting and occlusal adjustment [Colour figure can be viewed at wileyonlinelibrary.com]
Selection process for the studies included. Procedure applied in the study: *s-splinting, ¤o-occlusal adjustment, ‡so-splinting and occlusal adjustment [Colour figure can be viewed at wileyonlinelibrary.com]
Fifty-one articles were retrieved for full-text reading, and 46 articles were then excluded from further analysis. Reasons for exclusion are outlined in Appendix S2. Among the five studies included, two were retrospective case series on TS (Sonnenschein et al., 2017; Graetz et al., 2019), while for OA, two prospective studies (Fleszar et al., 1980; Kerry et al., 1982), and one RCT were identified (Burgett et al., 1992). In the study by Sonnenschein et al. (2017), only the period of up to 7 years of observation was initially considered due to the high drop-out rate of 59% after 10 years and 90% after 15 years (Sonnenschein et al., 2017). The limited number and heterogeneity of included articles hampered performance of a meta-analysis.
4.2 Quality assessment 4.2.1 Tooth splintingQuality assessment for studies on TS was based on the Newcastle–Ottawa Scale, and both publications were rated 5 (out of possible 5 stars), indicating a low risk of bias (Table 1a). The items in the Selection category (representativeness of study cohort, ascertainment of exposure) and those in the Outcome category (assessment of outcome, follow-up time, and adequacy of follow-up) were graded as secure for both single-centre analyses (Sonnenschein et al., 2017; Graetz et al., 2019).
TABLE 1. Quality assessment of included studies using the Newcastle–Ottawa Scale (a) and the Cochrane Collaboration's tool for assessing risk of bias including domain-level judgements for each result (b) and weighted bar plots of the distribution of risk-of-bias judgements within each bias domain (c) (a) First author (year) Selection Comparability Outcome Total of stars Representativeness of the exposed cohort Selection of non-exposed cohort Ascertainment of exposure Demonstration that outcome of interest was not present at start of study Comparability of cohorts on the basis of the design or analysis Assessment of outcome Was follow-up long enough for outcomes to occur? Adequacy of follow-up of cohorts Sonnenschein et al. (2017) ★ n.a. ★ n.a. n.a. ★ ★ ★ 5 Graetz et al. (2019) ★ n.a. ★ n.a. n.a. ★ ★ ★ 5 (b) (c)
(c)
 Abbreviation: n.a., not applicable.
4.2.2 Occlusal adjustment
Abbreviation: n.a., not applicable.
4.2.2 Occlusal adjustment
Quality assessment of the three studies included was based on the Cochrane Collaboration's tool for assessing risk of bias resulting in an unclear risk of bias (Table 1b,c). All three studies were performed by the same research group, thus indicating a research-centre bias.
4.3 Population 4.3.1 Tooth splintingRegarding the two retrospective case series related to TS, data from a total of 81 patients were further analysed, and 321 splinted teeth were followed over a time period of 3–15 years (Sonnenschein et al., 2017) and of 2–32.4 years (Graetz et al., 2019). At baseline TM grades, TL, PPD, and BL were reported in both studies (Sonnenschein et al., 2017; Graetz et al., 2019), whereas the clinical parameters CAL, PI, and bleeding index (BI) were presented in the article by Sonnenschein et al. (2017) (Table 2). Prior to TS, at least one tooth with mobility grade 1–3 was present (Sonnenschein et al., 2017; Graetz et al., 2019). Further, Sonnenschein et al. excluded patients exhibiting cross-bites in the frontal region and/or oral parafunctions. Among the 24 included patients, 12 patients with Eichner class A, 3 patients with Eichner class B1, 5 patients with class B2, B3, and B4 with one patient each, and 2 patients with class C2 were identified, and functional loading of the splinted teeth by natural antagonists was given (Sonnenschein et al., 2017). In the study by Graetz et al., bruxism was determined as a potential cofactor at baseline, and the 57 included patients presented with various Eichner Classes including Class A, Class B1, B2, and B2, as well as Class C (no antagonistic contacts) (Graetz et al., 2019).
TABLE 2. Characteristics of included studies related to splinting First author (year) country funding Study type study design settinga examiner calibration n patients (n female) Mean age ± SD (range) n smokers Periodontal diagnosis Patient-related inclusion criteria tooth-related inclusion criteria Test control Splinting indication type and number of teeth time point material Periodontal treatment Follow-up (years) mean ± SD (range) time points n dropouts reasonSonnenschein et al. (2017)
Germany
None
Case series
Retrospective
University
n.r.
Calibratedb
24 patients (15 female)c
55.3 (37–76)c
1 S, 1 FS, 22 NSc
22 ChP, 2 AgPc
Patient-related inclusion criteria:
Tooth-related inclusion criteria: Splint of 2–6 anterior mandibular teeth and X-ray at splinting time ± 18 months ≥1 tooth with increased mobility, CAL ≥5 mm and ≥50% RBL Dental and periodontal status (PPD, CAL at 6 sites/tooth) before splinting/APT and after 3 years ± 6 months No known oral parafunctions No cross-bites in the frontTest: splinted teeth
Control:
remaining dentition
Increased mobility combined with CAL ≥5 mm at ≥1 site of the affected tooth and ≥50% RBL
mandibular incisors and canines
Four patients with composite adhered pontic
2 teeth (4 patients), 3 teeth (5 patients), 4 teeth (6 patients), 5 teeth (2 patients), 6 teeth (7 patients) splinted
17 splints before APT, 7 splints between FMD and completion of APTd
composite (20 splints) or fibre glass reinforced composite splint (4 splints)e
APT:
oral hygiene assessment, motivation and instruction, professional tooth cleaning with hand instruments, polishing, fluoride application, subgingival debridement under local anaesthesia (FMD), periodontal surgery after 3–6 months if required
SPT:
≥ 1/year, oral hygiene assessment, re-motivation and re-instruction, professional tooth cleaning with hand instruments, subgingival reinstrumentation if PPD = 4 mm with BOP and/or ≥ 5 mm (PPD and CAL ≥1/year), polishing, fluoride application
n.r. (3–15f ± 0.5 months)
5, 7, 10, 12, 15
9 after 5 years, 6 after 7 years, 8 after 10 years, 8 after 12 years, 4 after 15 years
SPT interval < 1 visit/year
Graetz et al. (2019)
Germany
None
Case series
Retrospective
University
n.r.
n.r.
57 patients (38 female)
48.9 ± 13.1 (23–72)
18 S, 1 FS, 38 NS
49 ChP, 8 AgP
Patient-related inclusion criteria:
18–80 years finished APT SPT for ≥2 years with ≥1 visit/year Tooth-related inclusion criteria: Splint of ≥2 teeth; Annual PPD and X-ray at splint insertion or 1 year after and at last SPT visitTest: splinted teeth
Control:
non-splinted teeth
High mobility, usually combined with extensive bone loss
Type of teeth: n.r.
≥ 2 teeth (to 1 tooth or to both sides)
10 teeth (9 patients) had amputation of 1–2 roots prior to splinting
mean n of splinted teeth/patient: 4.1 ± 2.4 (1–11)
mean splints/patient: 1.7 ± 1.0 (1–5)
Splinting during or after APT
Composite or glass-fibre/metal-reinforced composite splint
APT:
subgingival debridement with, if indicated, additional access flap and/or adjunctive systemic antibiotic therapy, re-evaluation after 3–6 months
SPT:
oral hygiene re-motivation and re-instruction, professional tooth cleaning with subgingival reinstrumentation of residual pockets and polishing by a dental auxiliary; individualized intervals of 3–12 months; if necessary surgery with or without systemic adjunct antibiotic therapy
11.0 ± 7.2
(2.0–32.4)
Prior to APT (control group); prior to splinting (test group); end of investigation (test and control group)
n.a. Abbreviations: AgP, aggressive periodontitis; APT, active periodontal therapy; BL, bone loss; BOP, bleeding on probing; CAL, clinical attachment loss; ChP, chronic periodontitis; FS, former smoker; GBR, gingival bleeding index; FMD, full mouth disinfection;; n.r., not reported; NS, non-smoker; PCR, plaque control record; PPD, probing pocket depth; RBL, relative bone loss; S, smoker; SPT, supportive periodontal therapy. a University/practice. b Calibrated for study re-examination. c Recalculation by the reviewers based on the provided original data from Sonnenschein et al., 2017. d Time period from first oral hygiene training until successful completion of APT, that is, no site with PPD ≥6 mm. e Isolation of treated teeth. f After splint insertion.At the 7-year re-examination, Sonnenschein et al. (2017) evaluated 93 splinted lower anterior teeth and 294 teeth of the remaining dentition without further stratification into tooth type, position, or TM in 24 patients with 22.38 (±6.3) teeth on average. In the study by Graetz et al. (2019), splinted teeth were compared to 1069 non-splinted teeth at the time of re-examination (2–32.4 years) in 57 patients with 22.3 (±3.9) teeth on average. The analysis was then stratified into groups of upper anterior, lower anterior, and posterior teeth (Graetz et al., 2019).
4.3.2 Occlusal adjustmentThe studies related to OA included 82 patients with 1974 teeth (Fleszar et al., 1980), 93 patients with 2421 teeth (Kerry et al., 1982), and 50 patients with a mean number of 27 teeth (range 20–32) (Burgett et al., 1992). Burgett et al. reported CAL, PPD, and TM; Fleszar et al. reported TM and CAL in respect to initial PPD; and Kerry et al. reported TM (Table 3. In all three studies, patients were diagnosed with moderate to severe periodontal disease with PPD >4 mm (Table 4.
TABLE 3. Outcome parameters of included studies related to occlusal adjustment First author (year) Group Time point n teeth (maxilla/mandible) n (%) teeth with mobility grade 0, I, II, III n tooth loss (%) PPD (mm) BL (%) (range; median) CAL (mm) PI (%) BI (%) Fleszar et al. (1980) Test Baseline 1974 (n.r) n.r. (pooled data on patient level of tooth mobility from 0 to III) n.r. n.r. n.r. n.r. n.r. n.r. After 8 years 1083 (n.r.) n.r. (pooled data on patient level of tooth mobility from 0 to III) n.r. n.r. n.r.Pooled data on patient level after 1–8 years
initial pocket depth of 1–3 mm and mobility
0: −0.27 to −0.61
I: −0.38 to −0.83
II: −0.59 to −1.05
III: −0.76 to −1.08
initial pocket depth of 4–6 mm and mobility
0: 0.69 to 0.49
I: 0.61 to 0.25
II: 0.31 to 0.01
III: −0.11 to 0.21
initial pocket depth of 7–12 mm and mobility
0: 2.57 to 2.31
I: 1.90 to 1.89
II: 1.64 to 1.20
III: 0.95 to n.a.
n.r. n.r. Control n.a. Kerry et al. (1982) Test Baseline 2421 (n.r.)979a (40.4a), 1226a (50.6a), 216a (9a), n.r.
n.r. n.r. n.r. n.r. n.r. n.r. After 2 years 2421 (n.r.) 1304a (53.9a), 1035a (42.8a), 82a (3.3a), n.r. n.r. n.r. n.r. n.r. n.r. n.r. Control n.a. Burgett et al. (1992) Test Baseline n.r. n.r. n.r.Data on patient level:
3.66 ± 0.75 (srp)
3.64 ± 0.61 (mW)
n.r.Mean data on patient level:
−3.52 ± 0.81 (srp)
−3.48 ± 0.76 (mW)
n.r. n.r. After 2 years n.r. n.r. n.r.3.08 ± 0.41 (srp)
2.90 ± 0.33 (mW)
n.r.0.46 ± 0.66 (srp)
0.37 ± 0.68 (mW)
n.r. n.r. Control Baseline n.r. n.r. n.r.Data on patient level:
3.58 ± 0.58 (srp)
3.62 ± 0.68 (mW)
n.r.Mean data on patient level:
−3.44 ± 1.20 (srp)
−3.50 ± 1.19 (mW)
n.r. n.r. After 2 years n.r. n.r. n.r.3.04 ± 0.43 (srp)
2.89 ± 0.41 (mW)
n.r.0.08 ± 0.53 (srp)
−0.03 ± 0.54 (mW)
n.r. n.r. Note: If not otherwise indicated, parameters are presented as means ± SD. Abbreviations: BI, gingival bleeding index; BL, bone loss; CAL, clinical attachment loss (+ = gain; − = loss); mW, modified Widman flap; n, number; n.a., not applicable; n.r., not reported; PI, plaque index; PPD, probing pocket depth; srp, scaling and root planning. a Calculated by the authors. TABLE 4. Characteristics of included studies related to occlusal adjustment First author (year) country funding Study type study design settinga examiner calibrationb n patients (n female) mean age ± SD (range) n smokers periodontal diagnosis patient-related inclusion criteria tooth-related inclusion criteria Test control Occlusal adjustment indication type and number of teeth time point Periodontal treatment Follow-up (years) mean ± SD (range) time points n drop-outs (reason)Fleszar et al. (1980)
USA
None
Case series
Prospectivec
University
n.r.
n.r.
82 patients (n.r.)
n.r.
n.r.
moderate to severe periodontitis
Patient-related inclusion criteria:
Completion at least the first 1-year recall and scoring One or more periodontal pockets >4 mm Tooth-related inclusion criteria with three severity groups: Group1—initial pocket/sulcus depth 1–3 mm Group 2—initial pocket/sulcus depth 4–6 mm Group 3—initial pocket/sulcus depth 7–12 mmTest: occlusal adjustment
control:
n.a.
OA of entire dentitions during initial treatment phaseInitial therapy:
scaling, root planning, oral hygiene instruction, occlusal adjustment
APT:
all patients on randomized basis had each half of their mouth treated with one of the following surgical procedures: subgingival curettage, modified Widman flap surgery, pocket elimination surgery
SPT:
recall every 3 months for prophylaxis
8
n.r.
annually 1–8 years
10 after 5 years,
29 after 8 years
(n.r.)
Kerry et al. (1982)
USA
Grant No.
DE 02731
Case series
Prospective
University
n.r.
n.r.
93 patients (n.r.)
n.r.
n.r.
Moderate to severe periodontitis
Patient-related inclusion criteria:
n.r.
Tooth-related inclusion criteria:
n.r.
Test: occlusal adjustment
control:
n.a.
OA of entire dentitions during initial treatment phaseInitial therapy:
scaling, root planning, oral hygiene instruction, occlusal adjustment
APT:
all patients had each quadrant treated with one of the following surgical procedures randomly assigned: pocket elimination, subgingival curettage, modified Widman flap surgery, scaling & root planning by a periodontist
SPT:
recall every 3 months
2
n.r.
baseline; after initial therapy; 1 month, 1 and 2 years after APT
n.r.Burgett et al. (1992)
USA
None
RCT
University
n.r.
n.r.
50 patients (29 female)
44.2 ± 11.2 (25–69)
n.r.
Moderate to advanced periodontitis
Patient-related inclusion criteria:
Adults diagnosed with moderate or advanced periodontitisTooth-related inclusion criteria:
n.r.
Test: occlusal adjustment
(n = 22)
Control:
no occlusal adjustment
(n = 28)
Random allocation of patients to OA (entire dentitions) and no OA during initial treatment phaseInitial therapy:
scaling, root planning, smoothing of restorations, polishing of the teeth, oral hygiene instruction, fluoride treatment, occlusal adjustment (test group)
APT 2 months after initial therapy:
Split-mouth design with random allocation to Widman flap on one side and scaling and root planning on the other side
SPT:
recall every 3 months
2
n.r.
baseline; 1 and 2 years after APT
n.r. Abbreviations: APT, active periodontal therapy; OA, occlusal adjustment; n.a., not applicable; n.r., not reported; RCT, randomized clinical trial; SPT, supportive periodontal therapy. a University/practice. b Calibrated for study re-examination. c Data from Ramfjord et al. (1973). 4.4 Indications and intervention 4.4.1 Tooth splintingIn the included TS studies, the periodontal treatment regimens consisted of non-surgical periodontal therapy in combination with open-flap debridement and adjunctive antibiotic treatment (Graetz et al., 2019), resective surgery in four cases, and regenerative periodontal surgery in three cases (Sonnenschein et al., 2017). The non-surgical periodontal therapy included motivation and instruction for optimal individual plaque control (Sonnenschein et al., 2017; Graetz et al., 2019). Sonnenschein et al. performed subgingival debridement following the adapted protocol proposed by Quirynen et al. (1995).
TS was indicated in teeth with increased mobility and performed before, during, or after completion of the phase of active periodontal therapy (APT) (Sonnenschein et al., 2017; Graetz et al., 2019). In addition, the study by Sonnenschein et al. (2017) defined a CAL ≥5 mm at ≥1 site of the affected tooth and
留言 (0)