
記住我

Enkephalins are endogenous opioid peptides that exert cardiodepressive effects, such as reducing heart rate and inhibiting norepinephrine release, as well as improving renal function by increasing renal blood flow and urinary output.1-5 Proenkephalin (PENK) is a stable surrogate for enkephalins.3 In subjects from the general population, higher concentrations of PENK were associated with a higher risk of development of chronic kidney disease (CKD).6, 7 In patients with an acute myocardial infarction, higher plasma PENK concentrations have been associated with an increased risk of development of heart failure (HF).8 In patients with established HF, PENK concentrations were elevated and higher concentrations have been associated with HF severity, worse(ning) of renal function (reflected by both glomerular and tubular renal markers), and adverse clinical events.9-12 It remains to be established whether higher concentrations of PENK are also associated with an increased risk of new-onset HF. We, therefore, investigated the association between higher PENK concentrations and new-onset HF in the general population.
2 METHODS 2.1 Patient populationThe prevention of renal and vascular end-stage disease (PREVEND) study was designed to prospectively investigate the natural course of urinary albumin excretion (UAE) and its association with the development of cardiorenal disease in the general population.13 From 1997 to 1998, all inhabitants of Groningen (The Netherlands) aged 28–75 years were asked to complete a questionnaire and send a vial containing early morning urine. Among respondents, 6000 subjects with a morning UAE ≥10 mg/L and 2592 randomly chosen subjects with UAE <10 mg/L were included. These 8592 subjects (4291 men, 4301 women) comprised the cohort that participated in the baseline screening assessment (1997–1998). From 2001 to 2003, the second screening followed (n = 6894), which was the starting point of the present study. Among these subjects, those who had already developed HF before the second screening assessment or were classified as having HF with midrange ejection fraction (left ventricular ejection fraction [LVEF] 41%–49%) were excluded (n = 53 and n = 8, respectively), as well as subjects with missing PENK values (n = 156), resulting in a study population of 6677 subjects (Figure 1).

Flow diagram of in- and exclusion of patients. PENK, proenkephalin
The PREVEND study was approved by the medical ethics committee of the University Medical Center Groningen and was conducted in accordance with the Declaration of Helsinki. Written informed consent was obtained from all participants.
2.2 Data collection and measurementsAll participants completed a self-administered questionnaire regarding demographics, cardiovascular and renal disease history, smoking habits, alcohol consumption, and medication use prior to the baseline screening assessment. Medication use was verified with community pharmacies. Blood pressure was measured on the right arm, every minute for 10 and 8 minutes, respectively during two examination visits of the second screening visit. The mean of the last two recordings from each of the two examinations was used. Fasting blood samples were obtained in the morning and stored at −80°C. All participants collected two consecutive 24-hour urinary specimens, subsequently stored at −20°C.
PENK was measured in plasma using a sandwich immunoassay targeting PENK amino acids 119–159 (SphingoTec GmbH, Hennigsdorf, Germany) as described previously.14 The lower detection limit of the assay was 7 pmol/L and mean interassay coefficients of variation was 5.7% in the measuring range 10.9–686.3 pmol/L. Total cholesterol, high-density lipoprotein cholesterol, and low-density cholesterol were determined as previously described.15 Serum creatinine measurement was performed by an isotope dilution mass spectrometry traceable enzymatic method (Roche Diagnostics, Mannheim, Germany). UAE was measured by nephelometry with a threshold of 2.3 mg/L and intra- and interassay coefficients of variation of 2.2% and 2.6%, respectively (Dade Behring Diagnostic, Marburg, Germany). N-terminal pro brain natriuretic peptide (NT-proBNP) and high-sensitivity C-reactive protein were measured as previously described.16, 17
2.3 DefinitionsEstimated glomerular filtration rate (eGFR) was calculated using the CKD-EPI creatinine formula.18 PENK was investigated according to varying degrees of glomerular function and glomerular damage defined by Kidney Disease: Improving Global Outcomes (KDIGO) GFR and albuminuria categories.19 KDIGO GFR and albuminuria categories “high risk” and “very high risk” versus “low risk,” or “moderately increased risk” were used to investigate interactions between presence/severity of kidney disease and PENK concentrations with regards to outcomes. Type 2 diabetes was defined as a fasting glucose of ≥7.0 mmol/L, a non-fasting glucose of ≥11.1 mmol/L, or the use of antidiabetic medication. Left ventricular hypertrophy was defined according to the Cornell criteria on electrocardiography: a value of >2440 mm/ms as resulting from RaVL+SV3 (with 6 mm added in women) multiplied by QRS duration.
2.4 New-onset heart failureDetails on the methodology for identifying new-onset HF in PREVEND have been published previously.20 In brief, hospital records from both hospitals in Groningen, the University Medical Center Groningen and Martini Hospital, were checked for the presence of HF at baseline and for new-onset HF. This was done by recording signs, symptoms, and objective evidence of HF. Permission to access hospital records was granted by the local Ethics Committees. Criteria were used in accordance with the European Society of Cardiology Heart Failure Guidelines applicable at the time.21 Each case was validated anonymously by two different HF experts including clinical charts, hospitalization, and physician office records of suspected cases. LVEF at time of diagnosis was used to define HF with reduced ejection fraction (HFrEF) and HF with preserved ejection fraction (HFpEF; LVEF ≤40% or ≥50%, respectively).
2.5 Cardiac and cardiovascular events and mortalityCardiovascular endpoints were obtained through the Dutch national registry of hospital discharge diagnoses (PRISMANT), and adjusted according to detection in hospital records. Cardiac events (which were classified as being fatal or nonfatal) included acute myocardial infarction (ICD-10 code 410), acute and subacute ischaemic heart disease (411), coronary artery bypass grafting, and percutaneous coronary angioplasty. Cardiovascular events (also classified as being fatal or non-fatal) included cardiac events with the addition of stroke (subarachnoid hemorrhage [430], intracerebral hemorrhage [431], other intracranial hemorrhage [432], or occlusion or stenosis of the pre-cerebral [433], or cerebral arteries [434]), and vascular interventions. Data on mortality was obtained from Statistics Netherlands to allow for competing risks analysis.22
2.6 Follow-upTime to events was defined from the date of the subject's second screening visit until the date of first new-onset HF, cardiovascular events, death, or January 1, 2011. If a person had moved to an unknown destination, the date of last contact served as the censor date.
2.7 Statistical analysisBased on the population size and range of PENK, PENK was divided into quintiles. Data are presented as mean ± SD when normally distributed, as median (Q1–Q3) for skewed variables, and as frequency (percentage) for categorical variables. Trends over PENK quintiles were statistically tested with the Cochran–Armitage trend test, Jonckheere–Terpstra test, or a linear regression model for categorical, skewed, or normally distributed variables, respectively. Otherwise, continuous normally distributed variables were tested with the student independent t-test or analysis of variance (ANOVA), skewed variables with the Mann–Whitney U or Kruskal–Wallis test, and categorical variables with χ2 tests.
Determinants of PENK concentrations were analyzed using univariable and multivariable regression analyses, in which all variables with p < .1 in univariable analysis were included in the multivariable analysis and subjected to the backward elimination method. For all linear regression analyses, the assumption of linearity and normal distribution of residuals was checked, as well as checks for outliers. If necessary, variables were transformed using natural logarithm, including PENK. Variables in multivariable regression models were checked for multicollinearity, which led to exclusion of age from the model due to multicollinearity with eGFR, with weak contributory value from age. Variables with p < .05 were retained in the final multivariable regression model. Competing-risk regression analysis was used to assess whether PENK concentrations were associated with new-onset HF, HFrEF, and HFpEF, where death was considered a competing risk in all analyses. In analyses pertaining HFrEF and HFpEF specifically, the other HF entity was additionally considered a competing risk. Competing-risk regression analysis was executed using the cmprsk package, which uses Fine–Gray regression. Competing-risk regression models were adjusted for sex, eGFR, and body mass index (BMI), and results are expressed as hazard ratios (HRs) per doubling of PENK with their corresponding 95% confidence intervals (CIs). The assumption of proportionality of hazards and linearity were checked in all analyses. In addition, interactions were evaluated in cox proportional hazard models between PENK concentrations and sex, KDIGO risk categories, and presence of eGFR <60 ml/min/1.73 m2. Cox proportional hazard models were also constructed for cardiovascular events to evaluate the prognostic predictability of log doubling of PENK concentrations, adjusted for sex and eGFR. Additional packages that were used in the analysis included the packages clinfun, DescTools, foreign, Hmisc, ggplot2, ggpmisc, lm.beta, nephro, psych, survival, and survminer. A two-tailed p-value <.05 was considered statistically significant. All statistical analyses were executed using R (version 3.4.3, R Foundation for Statistical Computing, Vienna, Austria).
3 RESULTS 3.1 Baseline characteristics according to plasma PENK concentrationsIn the current study cohort, the mean age was 54 ± 12 years, and 3360 (50.3%) of subjects were female. Median plasma PENK concentrations were 52.7 (45.1–61.9) pmol/L in the overall study cohort, and 54.9 (47.2–64.0) pmol/L and 50.7 (43.3–59.3) pmol/L in women and men, respectively (p < .001). Subjects with higher PENK concentrations were, among others, older, more often female, had a lower BMI, were more often on antihypertensive treatment, had a lower eGFR, and had higher concentrations of NT-proBNP, serum creatinine, and urea (Table 1; all p for trend <.001). UAE approximated a U-shape over quintiles of PENK (p < .001). In Table S1, PENK concentrations are represented over KDIGO GFR and albuminuria categories, showing increasing PENK concentrations over GFR categories in all albuminuria categories (all p < .001), and also an increase of PENK concentrations over albuminuria categories in all GFR categories except G3b (all p < .05).
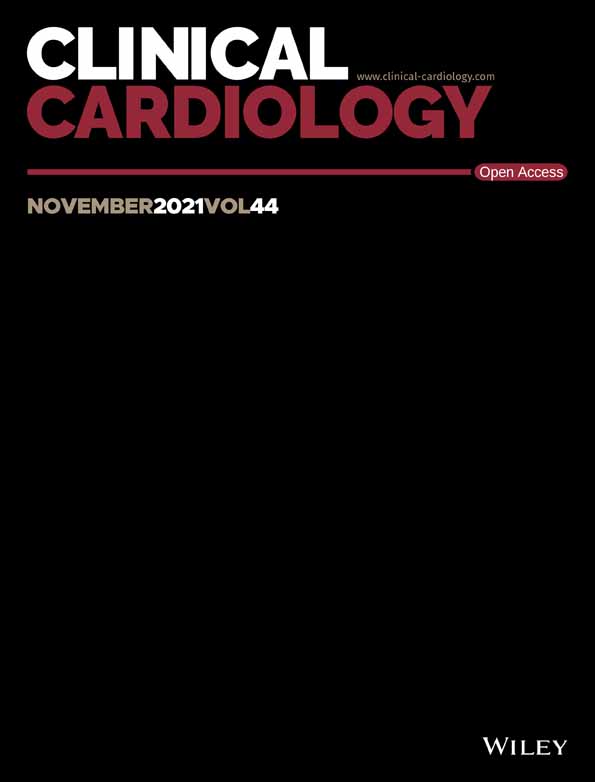
TABLE 1. Baseline characteristics of the PREVEND study in relation to quintiles of PENK concentrations Variables PENK (pmol/L) p for trend Q1, n = 1336 39.2 (35.9–41.6) Min 19.1, max 43.4 Q2, n = 1335 46.7 (45.1–48.2) Min 43.4, max 49.7 Q3, n = 1335 52.7 (51.2–54.4) Min 49.8, max 56.0 Q4, n = 1335 59.7 (57.8–61.8) Min 56.0, max 64.4 Q5, n = 1336 71.7 (67.7–78.9) Min 64.4, max 532.3 Clinical characteristics Age (years) 52 ± 11 53 ± 11 53 ± 12 53 ± 12 57 ± 14 <.001 Sex (female), n (%) 498 (37) 623 (47) 671 (50) 755 (56) 813 (61) <.001 Race (Caucasian), n (%) 1278 (96) 1267 (95) 1278 (96) 1276 (96) 1258 (94) .172 BMI (kg/m2) 28.0 ± 4.6 27.0 ± 4.2 26.5 ± 4.1 26.1 ± 4.2 26.0 ± 4.3 <.001 Systolic blood pressure (mm Hg) 128 ± 17 127 ± 18 125 ± 18 124 ± 20 128 ± 21 <.001 Diastolic blood pressure (mm Hg) 75 ± 9 74 ± 9 73 ± 9 72 ± 9 73 ± 9 <.001 Heart rate (bpm) 69 ± 10 69 ± 10 68 ± 10 68 ± 10 69 ± 10 .097 LVH according to Cornell, n (%) 26 (2) 22 (2) 29 (2) 26 (2) 33 (2) .270 Medical history, n (%) Coronary heart disease 45 (3) 27 (2) 37 (3) 44 (3) 79 (6) <.001 Diabetes mellitus 129 (10) 69 (5) 58 (4) 63 (5) 68 (5) <.001 Smoking or quit ≤1 year 472 (35) 512 (38) 515 (39) 506 (38) 518 (39) .075 Medication, n (%) Lipid-lowering treatment 124 (9) 110 (8) 105 (8) 138 (10) 166 (12) <.001 Antidiabetic treatment 59 (4) 42 (3) 40 (3) 35 (3) 42 (3) .047 Antihypertensive treatment 271 (20) 257 (19) 226 (17) 262 (20) 414 (31) <.001 Laboratory values Hemoglobin (g/dl) 8.6 ± 0.8 8.6 ± 0.8 8.5 ± 0.7 8.4 ± 0.8 8.4 ± 0.8 <.001 Sodium (mmol/L) 141 (139–142) 141 (140–142) 141 (140–142) 141 (140–142) 141 (140–142) <.001 Potassium (mmol/L) 4.2 (4.0–4.4) 4.2 (4.1–4.4) 4.2 (4.0–4.4) 4.2 (4.1–4.4) 4.2 (4.1–4.4) <.001 NT-proBNP (pg/ml) 31 (16–62) 36 (17–70) 41 (22–73) 45 (22–85) 58 (30–115) <.001 Glucose (mmol/L) 5.0 (4.5–5.5) 4.8 (4.5–5.3) 4.7 (4.4–5.2) 4.7 (4.4–5.2) 4.8 (4.4–5.3) <.001 ASAT (U/L) 23 (20–28) 22 (19–26) 22 (19–26) 22 (19–26) 22 (19–26) <.001 ALAT (U/L) 19 (14–28) 18 (13–25) 17 (13–24) 16 (12–22) 16 (12–21) <.001 Total cholesterol (mmol/L) 5.4 (4.7–6.1) 5.4 (4.8–6.1) 5.4 (4.7–6.1) 5.4 (4.7–6.1) 5.4 (4.7–6.2) .956 HDL cholesterol (mmol/L) 1.1 (1.0–1.4) 1.2 (1.0–1.4) 1.2 (1.0–1.4) 1.2 (1.1–1.5) 1.3 (1.1–1.5) <.001 LDL cholesterol (mmol/L) 3.3 (2.7–4.1) 3.5 (2.7–4.2) 3.6 (2.9–4.2) 3.3 (2.7–4.0) 3.4 (3.0–4.2) .843 CRP (mg/L) 1.5 (0.6–3.3) 1.4 (0.7–3.1) 1.3 (0.6–3.1) 1.3 (0.6–2.9) 1.4 (0.7–3.1) .095 Kidney function Creatinine (μmol/L) 70 (61–78) 69 (61–78) 71 (62–80) 71 (63–81) 75 (66–87) <.001 eGFR (ml/min/1.73 m2) 98 ± 12 96 ± 13 94 ± 13 92 ± 15 84 ± 19 <.001 Urea (mmol/L) 5.0 (4.2–5.8) 5.0 (4.2–5.9) 5.0 (4.3–5.9) 5.1 (4.3–6.0) 5.4 (4.5–6.4) <.001 Urinary albumin excretion (mg/24 h) 9.4 (6.7–17.0) 9.1 (6.3–16.6) 8.4 (6.0–14.9) 7.9 (5.9–14.1) 8.9 (5.8–20.4) <.001 Urinary creatinine excretion (mg/24 h) 1541 (1279–1825) 1408 (1171–1703) 1352 (1142–1665) 1298 (1084–1553) 1206 (1009–1460) <.001 Urinary urea excretion (mmol/24u) 246 (182–333) 230 (172–302) 226 (169–301) 222 (167–293) 208 (156–270) <.001 Abbreviations: ALAT, alanine transaminase; ASAT, aspartate aminotransferase; BMI, body mass index; CKD, chronic kidney disease; CRP, C-reactive protein; eGFR, estimated glomerular filtration rate; HDL, high-density lipoprotein; LDL, low-density lipoprotein; LVH, left ventricular hypertrophy; NT-proBNP, N terminal pro brain natriuretic peptide; PENK, proenkephalin. 3.2 Main correlates of PENK concentrationsCorrelation plots showing the association between PENK concentrations and eGFR and NT-proBNP, respectively, are displayed in Figure 2. The strongest independent correlates of higher log-transformed PENK were lower eGFR, lower log urinary creatinine excretion, and lower BMI (all p < .001; Table 2). The adjusted R2 of the model was 0.276.

Correlation plots of PENK with eGFR and NT-proBNP. Spearman correlation coefficients: eGFR, −0.276 (p < .001); NT-proBNP, 0.192 (p < .001). eGFR, estimated glomerular filtration rate; NT-proBNP, N-terminal pro brain natriuretic peptide; PENK, proenkephalin
TABLE 2. Multivariable linear regression analysis for PENK Variable Standardized beta T p-value eGFR −0.379 −22.922 <.001 Urinary creatininea −0.173 −11.186 <.001 BMI −0.130 −8.795 <.001 Smoking or quit ≤1 year 0.091 6.511 <.001 Glucosea −0.093 −6.416 <.001 Potassiuma 0.058 4.204 <.001 Sodiuma 0.056 4.119 <.001 Diastolic blood pressure −0.054 −3.505 <.001 Ureaa 0.052 3.380 <.001 Hemoglobin −0.051 −3.308 <.001 Urinary albumin excretiona 0.045 3.012 .003 NT-proBNPa 0.047 3.007 .003 Antihypertensive treatment 0.038 2.434 .015 Note: Adjusted R2 of model: 0.276. Abbreviations: BMI, body mass index; eGFR, estimated glomerular filtration rate; NT-proBNP, N terminal pro brain natriuretic peptide; PENK, proenkephalin. a log-transformed. 3.3 Plasma PENK concentrations are only univariably associated with new-onset heart failureIn the current study cohort, a total of 221 subjects developed HF after a median follow-up time (from the second screening visit) of 8.3 (7.8–8.8 years). The median time to HF diagnosis was 5.1 (2.9–6.7) years. In subjects who developed HF, median PENK concentrations were 56.2 (45.2–67.6) pmol/L and 52.7 (45.1–61.6) pmol/L in subjects who did not develop HF (p = .003). Among new-onset HF cases, 127 subjects developed HFrEF, and 94 subjects HFpEF. In univariable competing-risk regression analysis (Table 3), PENK concentrations were significantly associated with a higher risk of new-onset HF (HR = 2.09 [95% CI 1.47–2.97] per doubling of PENK, p < .001), new-onset HFrEF (HR = 2.31 [95% CI 1.48–3.61] per doubling of PENK, p < .001), and new-onset HFpEF (HR = 1.74 [95% CI 1.02–2.96] per doubling of PENK, p = .042). After adjustment for sex and its main determinant eGFR, PENK concentrations were no longer associated with new-onset HF and HFrEF. After additional adjustment for BMI, PENK concentrations were also no longer associated with new-onset HFpEF. There was no interaction between plasma PENK concentrations and sex, KDIGO risk category, nor with presence of eGFR <60 ml/min/1.73 m2 at baseline with respect to all three outcomes.
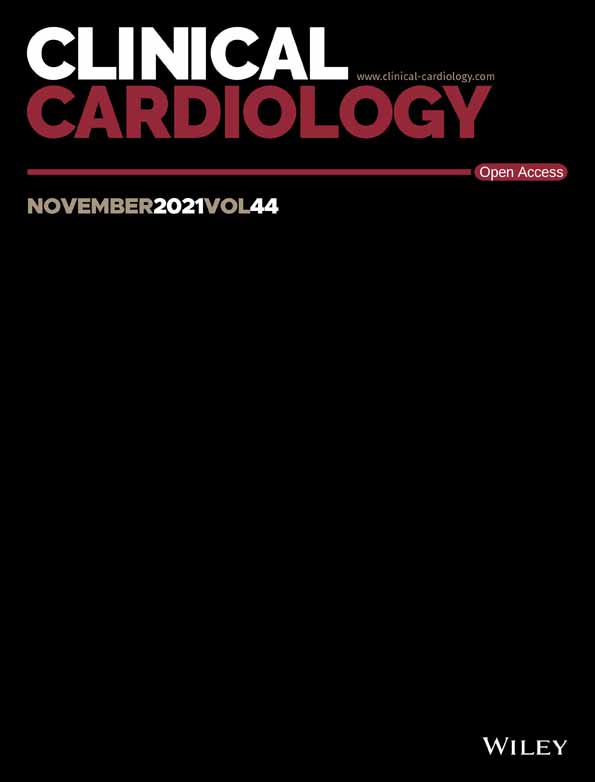
TABLE 3. Competing-risk regression analysis for PENK predicting new-onset heart failure, also stratified per HFrEF and HFpEF Outcomes Univariable Adjusted for sex and eGFR Additionally adjusted for BMI HR (95% CI) p-value HR (95% CI) p-value HR (95% CI) p-value HF (n = 221) 2.09 (1.47–2.97) <.001 0.85 (0.60–1.20) .360 1.07 (0.75–1.53) .720 HFrEF (n = 127)b 2.31 (1.48–3.61) <.001 1.09 (0.71–1.68) .690 1.26 (0.80–1.96) .320 HFpEF (n = 94)c 1.74 (1.02–2.96) .042 0.59 (0.35–0.99) .044 0.80 (0.47–1.36) .400 Abbreviations: BMI, body mass index; CI, confidence interval; HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; HR, hazard ratio; PENK, proenkephalin. a log base 2 transformed. b In addition to death, HFpEF development was also considered a competing risk. c In addition to death, HFrEF development was also considered a competing risk.Competing risks cumulative incidence curves for new-onset HF, HFrEF, and HFpEF respectively over quintiles of PENK concentrations illustrate an increasing risk with higher quintiles of PENK concentrations (Figure 3; p < .001 for HF; p = .003 for HFrEF; p = .039 for HFpEF).

Competing risks cumulative incidence curves for new-onset heart failure for quintiles of PENK concentrations. Cumulative incidence curves for new-onset heart failure, heart failure with reduced ejection fraction, and heart failure with preserved ejection fraction stratified over quintiles of PENK concentrations. The indicators Q1 to Q5 represent the first quintile of PENK concentrations to the fifth quintile of PENK concentrations, respectively. HF, heart failure; HFpEF, heart failure with preserved ejection fraction; HFrEF, heart failure with reduced ejection fraction; PENK, proenkephalin
In Table S2 the association of PENK with new-onset HF, HFrEF, and HFpEF was analyzed per quintile of PENK concentrations. The frequency of new-onset HF and HFrEF increased over ascending PENK quintiles (p = .003 and p = .019 respectively). The fifth and highest PENK quintile was univariably associated with new-onset HF (HR = 1.92 [95% CI 1.29–2.84], p = .001) and new-onset HFrEF (HR = 2.06 [95% CI 1.20–3.52], p = .009), but not after adjustment for sex and eGFR.
3.4 Plasma PENK concentrations and cardiac and cardiovascular eventsNon-fatal cardiac events, non-fatal cardiovascular events, and fatal cardiovascular events occurred in 359, 434, and 38 subjects respectively. Plasma PENK concentrations were univariably associated with all three events (Table S3; HR = 1.50 [95% CI 1.14–1.98] per doubling of PENK, p = .004 for non-fatal cardiac events; HR = 1.55 [95% CI 1.20–2.00] per doubling of PENK, p < .001 for non-fatal cardiovascular events; and HR = 4.07 [95% CI 2.22–7.49] per doubling of PENK, p < .001 for fatal cardiovascular evens), but not after adjustment for sex and eGFR. There was no interaction present between plasma PENK concentrations and sex, KDIGO risk category, or presence of eGFR <60 ml/min/1.73 m2 at baseline.
4 DISCUSSIONIn this study, we show data from the novel renal marker PENK in subjects from the general population. Those with higher plasma PENK concentrations were older, more often female, had lower eGFR, and higher concentrations of NT-proBNP. The main independent correlates of higher PENK concentrations were lower eGFR, lower urinary creatinine excretion, and lower BMI. Higher PENK concentrations were univariably associated with new-onset HF, HFrEF, and HFpEF in competing-risk regression analysis, but this association was mainly confounded by low eGFR. The association of PENK concentrations was similarly attenuated by low eGFR with regards to other cardiovascular outcomes.
留言 (0)