
記住我
In 1958, the American Medical Association, the American Dental Association, and several other health professional organizations created the Joint Council to Improve the Health Care of the Aged, which was dedicated to opposing the creation of the program that would eventually become Medicare. In the years since the council’s defeat, Medicare has proved transformative, with enrollment in the program at 65 years of age resulting in improved access to care and reductions in health-related racial inequities.1 Yet organized medicine and dentistry’s historical opposition to Medicare has at least one present-day legacy: with the exception of some Medicare Advantage plans, Medicare still lacks dental coverage.
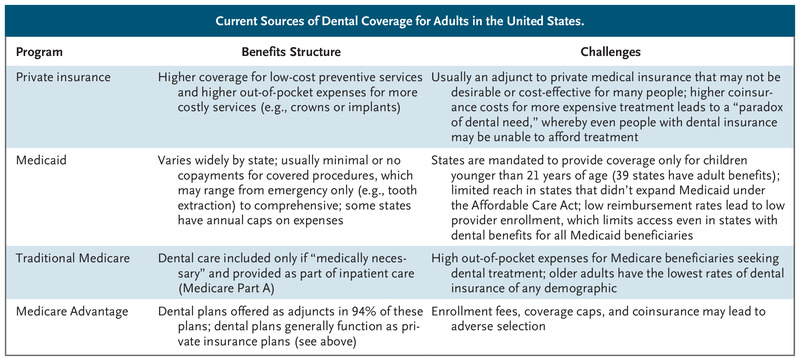
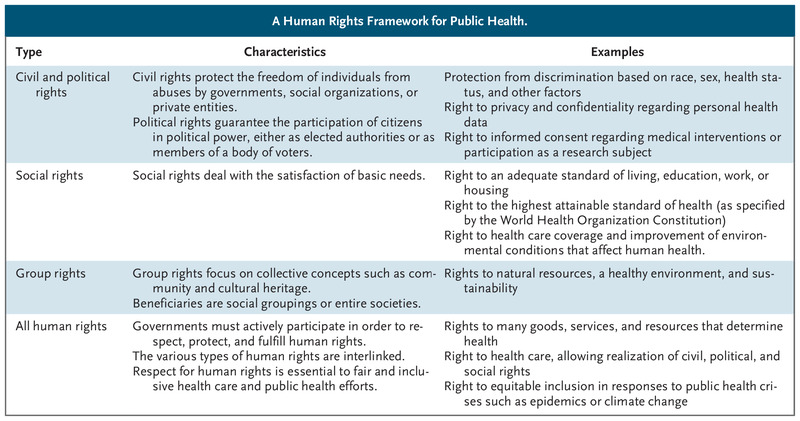
 Current Sources of Dental Coverage for Adults in the United States.
Current Sources of Dental Coverage for Adults in the United States. In 1965, nearly every older adult could expect to eventually lose all their teeth. Today, edentulism is no longer a consequence of age but is one of structural injustice. Dentistry continues to operate under a fee-for-service payment model, with higher proportions of costs that are out of pocket and higher financial barriers to access than other forms of health care. Moreover, most practice models focus on reconstructive care rather than on preventive measures to maintain dental health.2 These factors contribute to inequities in pain, edentulism, and unmet need affecting lower-income people, people of color, and older adults. Black and Latinx Americans are two to three times as likely to have untreated dental decay as White Americans, and low-income older adults are more than three times as likely to have lost all their natural teeth as older adults with incomes at or above 200% of the federal poverty level (FPL).3 The primary sources of dental coverage in the United States and their limitations are shown in the table.
After decades of unsuccessful attempts to enact a Medicare dental benefit, the federal government is closer than ever to doing so. In 2019, the House of Representatives passed the Elijah E. Cummings Lower Drug Costs Now Act (H.R. 3), which included proposed Medicare coverage for dental, vision, and hearing services, but the bill didn’t succeed in the Senate. The dental benefit was predicted to cost $238 billion over the first 10 years. A bill with similar provisions restricted to dental care (H.R. 502 and S. 97) was introduced in Congress in 2021. President Joe Biden’s budget-reconciliation package includes funding for a Medicare dental benefit, and in August 2021, the Centers for Medicare and Medicaid Services (CMS) appointed its first-ever chief dental officer, whose role is to “guide CMS in advancing oral health” in various federal health programs, including Medicare.
The American Dental Association has offered support for a Medicare dental benefit only if it includes so-called means testing to restrict coverage to people with incomes (from assets, pensions, and earnings) below 300% of the FPL and only if dental coverage would be separate from Medicare Parts A, B, and D (i.e., if Congress established a Medicare “Part T”). Beyond excluding many middle- and higher-income older adults who currently lack dental coverage, we believe a means-tested policy that is distinct from other Medicare benefits would restrict advances in oral health for two reasons.
First, limiting a Medicare dental benefit to low-income beneficiaries would make it financially straightforward for most dentists to refuse to accept Medicare. Lack of acceptance by dentists has plagued Medicaid dental programs throughout the country. Nationally, only 43% of dentists accept Medicaid or Children’s Health Insurance Program (CHIP) insurance,4 which has resulted in low access rates and poor oral health outcomes even in states whose Medicaid programs offer comprehensive adult dental benefits. Federally qualified health centers and other safety-net providers that accept public insurance are already at capacity and, without substantial private-sector participation, would struggle to accommodate increased demand among newly covered Medicare beneficiaries.
Second, a means-tested, stand-alone Part T benefit would perpetuate dentistry’s separation from the rest of the health care system. Although means testing has previously been proposed as an option to curb Medicare costs and determines some premium costs for beneficiaries in Medicare Part D, no other Medicare benefits are determined by income. Establishing a separately administered, means-tested Medicare dental program would maintain the financial and structural separation of dentistry and medicine, thereby precluding any innovation that could be achieved in the course of integrating medical and dental care.
A fully integrated dental benefit could lead to capitated-payment mechanisms that include both oral health and other health care services, as well as oral health quality metrics akin to those mandated for other forms of Medicare-reimbursed care. This type of centralization could help Medicare drive the incorporation of oral health into accountable care organizations and other health care delivery organizations, the development of quality-focused payment mechanisms, and multidisciplinary care coordination (e.g., vaccination in dental offices or delivery of preventive dental care during primary care visits). Medicare’s scope provides an opportunity for change that could improve the quality and cost-effectiveness of health care. The scale of disruptive innovation in dental practice would be lost if benefits were restricted to only a portion of Medicare beneficiaries and if benefit administration remained siloed.
The need for a Medicare dental benefit and the form that such a benefit would take are not concerns limited to dentists. The medical system already assumes the burdens associated with unmet dental need. Each year, millions of patients, including many older adults, present to emergency departments, hospitals, and primary care offices for the palliation of dental pain — visits that generally conclude with a directive to visit a dentist, which many patients are unable to do. Untreated dental disease can lead to endocarditis, brain abscesses, and mediastinitis. The local and systemic inflammation driven by common periodontal infections has been associated with worsening diabetes and increased cardiovascular disease risk. Older adults with untreated dental problems have less nutritious diets and higher rates of depression and isolation than those with good dental health. But the key reason that access to dental care is crucial is that, even in the absence of other medical complications, dental problems are a preventable and far-too-common source of disabling disease.5
Especially in the face of opposition from organized dentistry, current proposals for a Medicare dental benefit may be unsuccessful. Nonetheless, Democrats in Congress have expressed a commitment to establishing Medicare dental, vision, and hearing benefits as necessary steps on the path to “Medicare for All.” Even if a Medicare dental benefit is signed into law, numerous challenges will remain. Congress and CMS would need to develop a system for administering dental coverage, establish a fee schedule, and begin enrolling dental providers. Health systems would require time to scale up dental infrastructure to meet pent-up demand and develop and refine integrated care systems. With Medicare’s cost curve already a national concern, policymakers would need to determine which dental treatments would be covered and what forms of copayment or coinsurance would be required for beneficiaries. Even universal coverage of dental services would not ensure oral health for people in rural areas or low-income communities without accessible dental care. But we believe that none of these challenges should impede the adoption of a Medicare dental benefit.
Medicare’s evolution has had profound effects on not only the health of Medicare beneficiaries, but of all Americans. A Medicare dental benefit could transform dental care delivery to be more equitable, outcomes-driven, and integrated with the rest of the health care system, but only if dentists are compelled to take part. We believe that the implementation of a universal Medicare dental benefit is a health and health equity imperative.
留言 (0)