
記住我
When considering therapeutic interventions for acquired peripheral neuropathies, making a specific diagnosis is essential. A wide spectrum of therapies is now available across a range of acquired neuropathies including the demyelinating immune neuropathies such as chronic inflammatory demyelinating neuropathy (CIDP) and its variants, in addition to multifocal motor neuropathy (MMN) and vasculitic neuropathy. Across these presentations, suspected vasculitis is considered one of the most common indications for nerve biopsy, given that the diagnosis of CIDP and MMN tends to be made by clinical criteria and less invasive investigations.1, 2 However, considerable knowledge about the pathophysiology of these neuropathies has been gained through decades of nerve biopsies, mostly from an era when other diagnostic methods were not yet available. In focal or multifocal neuropathies, malignancy may be a differential diagnosis, including nerve tumors, paraneoplastic phenomenon, and hematological malignancy. These conditions are frequently misdiagnosed, and often nerve biopsy is required to cement a definitive diagnosis and suggest a therapeutic pathway.3
Histopathological processing of peripheral nerve biopsies should be performed in a laboratory that is specialized in neuromuscular diseases. Neuropathological work-up should include tinctorial stains (H&E, Congo red, Turnbull or Pear's), immunohistochemistry (inflammatory cells, neurofilaments, immunoglobulin and light-chain deposition, transthyretin), and semithin resin sections to provide a comprehensive and detailed look at relevant structures. Teased-fiber preparations allow a longitudinal assessment of the nerve fibers including nodes of Ranvier. Electron microscopy of ultrathin sections allows analysis of unmyelinated fibers (however, this has been partly substituted by skin biopsy), changes in myelin structure, macrophage-mediated demyelination, small deposits, or pathological inclusions. In the cases reported in this article, we provide examples of how these different methods and stains can, in combination, lead to the correct diagnosis.
The present review will highlight the insights that nerve biopsy has provided for the auto-immune inflammatory neuropathies, and how this has shaped current views about pathogenesis. Attention is also drawn to less common entities that can easily be mistaken or overlooked, if not included in the differential diagnoses of peripheral nerve manifestations of the disease.
2 CHRONIC INFLAMMATORY DEMYELINATING POLYNEUROPATHY: THE ROLE OF MACROPHAGESAlthough CIDP is usually diagnosed based on clinical manifestations and electrophysiological findings, physicians may encounter difficulties in diagnosing CIDP due to the lack of specific biomarkers. We present the case of a 61-year-old female, with distal-predominant global weakness and sensory disturbance, who was found to have CIDP with pathological evidence of demyelination resulting from phagocytosis of myelin by macrophages. This case demonstrates the ongoing importance of nerve biopsy to confirm the diagnosis and further delineate the underlying pathogenesis of CIDP.
2.1 Patient historyA 61-year-old woman noted numbness in the fingertips and toes at 60 years of age. The numbness gradually extended to the proximal limbs, and she became aware of unsteadiness of gait and weakness in both hands 2 months prior to admission. History included cervical cancer 7 years ago, which was resected. There was no family history.
2.2 Neurological examinationNeurological examination demonstrated symmetrical weakness in the upper and lower limbs. Weakness was more prominent distally. Sensory examination identified a glove and stocking pattern of impairment. Light touch and pain sensation were reduced mildly in the upper limbs and moderately in the lower limbs. Vibration sense was mildly reduced in the upper limbs and severely impaired in the lower limbs. Joint position sense was mildly affected in the toes. Romberg's sign was positive. Deep tendon reflexes were reduced in all four limbs. Plantar responses were flexor bilaterally.
2.3 Laboratory tests, electrophysiological, and imaging studiesCerebrospinal fluid examination revealed an increased protein level (87 mg/dL; normal, 15-45 mg/dL) and a normal cell count. In the right median, ulnar, and tibial nerves, motor nerve conduction velocities (MCV) were decreased to 12.5, 11.7, and 10.4 m/s, and distal motor latencies (DML) were prolonged to 12.6, 8.1, and 22.1 ms, respectively. Compound muscle action potentials (CMAPs) in these nerves were, respectively, 3.4, 1.7, and 0.1 mV. Sensory nerve action potentials (SNAPs) in the median, ulnar, and sural nerves were absent. The neurophysiological findings were consistent with a demyelinating neuropathy. Magnetic resonance imaging revealed thickening of cauda equina. Blood tests revealed normal levels of IgG, IgA, and IgM subclasses. A monoclonal protein was not detected by serum immunoelectrophoresis.
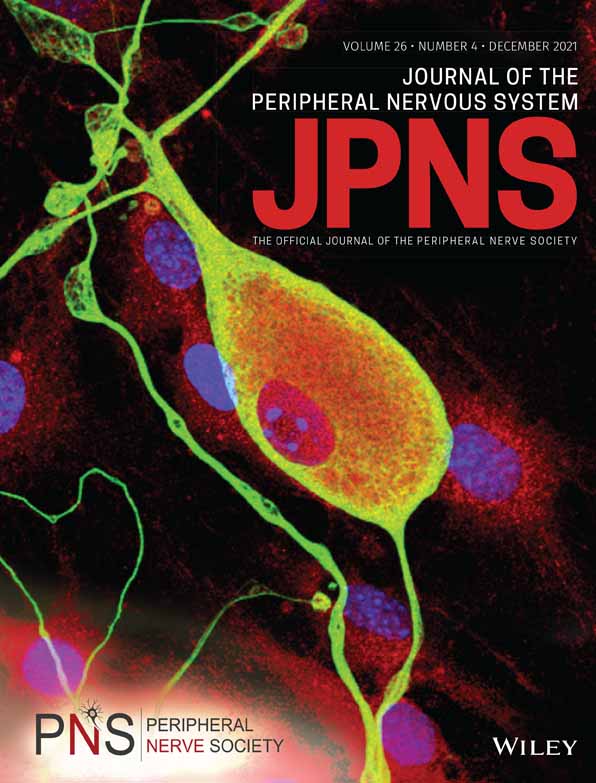
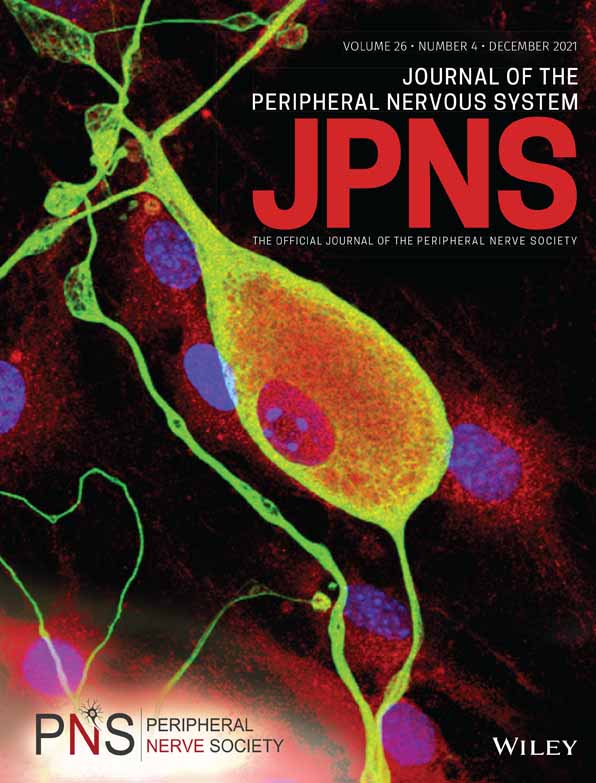
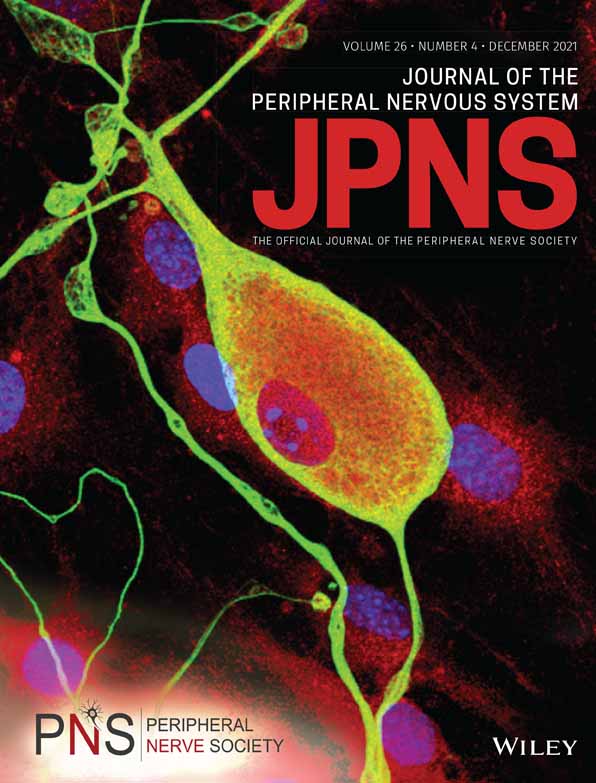
2.4 Nerve biopsy findingsSural nerve biopsy revealed moderate endoneurial edema and mild reduction of myelinated fiber density on transverse sections. Teased-fiber preparations showed segmental demyelination (2.5% of myelinated fibers) without tomaculous appearance. On electron microscopic examination, phagocytosis of myelin by macrophages was observed (Figure 1). Onion bulbs were also infrequently detected. Unmyelinated fibers were well preserved. Thus, macrophage-induced demyelination seems to play a role in the pathogenesis of neuropathy in this patient, which is compatible with the classical concept of chronic inflammatory demyelinating polyneuropathy (CIDP).

Representative electron microscopic photographs of myelin phagocytosis by macrophages in patients with CIDP. Transverse sections of sural nerve biopsy specimens. Uranyl acetate and lead citrate staining. A, A myelinated fiber is surrounded by macrophage cytoplasm that contains a small amount of myelin debris. The thickness of the myelin seems to be normal. Arrows indicate the basement membrane surrounding the myelinated fiber. B, A demyelinated axon is surrounded by macrophage cytoplasm abundant in myelin debris. An asterisk indicates an axon. A macrophage nucleus is indicated by M. Scale bars = 1 μm
2.5 DiscussionCIDP is one of the major immune-mediated demyelinating neuropathies frequently encountered in clinical practice.4 According to a study by Dyck et al., who established an entity of CIDP in 1975, a characteristic feature of this disease is macrophage-induced demyelination.5 Since then, further pathological evidence of demyelination in CIDP patients has been reported.6 The diagnostic criteria proposed by the Ad Hoc Subcommittee of the American Academy of Neurology AIDS Task Force in 1991 regarded the presence of demyelination using either electron microscopy or teased-fiber study mandatory for a definitive diagnosis of CIDP.7 In contrast, in the European Federation of Neurological Societies and Peripheral Nerve Society (EFNS/PNS) guideline, pathological evidence of demyelination is regarded as a supportive criterion.8 At present, CIDP is usually diagnosed based on clinical manifestations and electrophysiological findings in daily practice. However, the diagnosis of CIDP is sometimes difficult. For instance, some patients diagnosed with neuropathy associated with lymphoma or amyloidosis, fulfill the electrophysiological criteria for CIDP.9-11 Hence, demyelination resulting from myelin phagocytosis by macrophages will help to confirm the diagnosis of CIDP; however, lipid laden macrophages may also be evident in the acute inflammatory demyelinating polyneuropathy variant of Guillain-Barré syndrome.6, 12 Consequently, nerve biopsy remains useful when physicians cannot confirm a diagnosis of CIDP.
3 CHRONIC INFLAMMATORY DEMYELINATING POLYNEUROPATHY: A CASE WITH ANTI-NEUROFASCIN 155 ANTIBODIESElectron microscopy, undertaken on longitudinal sections of nerve biopsy specimens, plays an important role in identifying distinct pathologies from typical-CIDP. In this case, evaluation of a sural nerve biopsy specimen with electron microscopy revealed the presence of characteristic paranodal lesions distinct from conventional macrophage-induced demyelination. Thus, demonstrating the importance of nerve biopsy with electron microscopy to elucidate the typical pathogenesis observed in patients with anti-neurofascin 155 antibodies.
3.1 Patient historyA 15-year-old boy presented with a 7-month history of lower limb weakness. Numbness developed in the legs 1 month later. Weakness and numbness in the hands appeared soon afterwards, and he was unable to walk without assistance 2 months prior to admission to the hospital. Autonomic symptoms were absent, and there was no family history of neuropathy.
3.2 Neurological examinationNeurological examination demonstrated mild facial diplegia. Although the other cranial nerves were unremarkable on inspection, a nasal quality of voice was noted. The patient was wheelchair bound. Symmetrical limb weakness, which was predominantly distal, was evident throughout although more conspicuous in the lower upper limbs. His grip strength was 3/2 kg (right/left side). Muscle atrophy was observed distally in all four limbs. A sensory deficit was conspicuous, particularly in the lower limbs. Although light touch and pain sensations were relatively preserved, vibration and joint position sense was severely reduced. Mild postural and action tremor in the hands was observed. The deep tendon reflexes were reduced in four limbs and the plantar responses were flexor bilaterally.
3.3 Laboratory tests, electrophysiological, and imaging studiesCerebrospinal fluid examination revealed an increased protein level (199 mg/dL) and a normal cell count. The findings of nerve conduction studies indicated demyelinating neuropathy. Specifically, MCV, DML, and CMAPs in the median and ulnar nerves were 21.2 and 28.3 m/s, 11.7 and 8.6 ms, and 1.3 and 2.9 mV, respectively (right side). Conduction block was not observed. CMAPs in the tibial nerve and SNAPs in the median, ulnar, and sural nerves were not elicited. Cranial magnetic resonance imaging revealed no abnormalities. Blood tests revealed normal levels of IgG, IgA, and IgM. Monoclonal protein was not detected by serum immunoelectrophoresis. An enzyme-linked immunosorbent assay revealed anti-neurofascin 155 autoantibodies.
3.4 Nerve biopsy findingsSural nerve biopsy revealed mild endoneurial edema and normal myelinated fiber density on transverse sections. Teased-fiber preparations showed no segmental demyelination and very little axonal degeneration (2%). On electron microscopic examination, neither macrophage-induced demyelination nor onion bulb formation was observed. Unmyelinated fibers were well preserved. On longitudinal sections, detachment of myelin terminal loops from the axolemma (ie, paranodal dissection) was observed (Figure 2). These findings suggested that the aberrant nerve conduction in this patient is caused by anti-neurofascin 155 antibody-induced axo-glial detachment, but not by macrophage-induced demyelination.

Representative electron microscopic photograph of paranodal dissection in patients with CIDP with anti-neurofascin 155 antibodies. Longitudinal section of the sural nerve biopsy specimen. Uranyl acetate and lead citrate staining. A clear space is observed between the paranodal myelin terminal loops and the axolemma (arrows). Scale bar = 0.2 μm
3.5 DiscussionRecent studies have revealed that sural nerve biopsy specimens from some CIDP patients show paranodal lesions induced by IgG4 autoantibodies against paranodal junction components, such as neurofascin 155 and contactin 1.13-15 In particular, 5% to10% of CIDP patients have anti-neurofascin 155 antibodies. Patients with these antibodies can manifest characteristic features such as sensory ataxia, tremor, and poor response to intravenous immunoglobulin treatment.6 Studies of longitudinal sural nerve sections reveal IgG4 deposition at paranodes and paranodal myelin terminal loop detachment from the axolemma.14 As these patients lack classical macrophage-induced demyelination, the mechanisms of neuropathy are considered to be distinct from those in conventional CIDP patients. Recognition of this different pathophysiology has altered treatment paradigms in CIDP with paranodal antibodies, with the appreciation that these patients may be more responsive to rituximab.16, 17 Clinical trials are ongoing to prospectively evaluate treatment response to rituximab in CIDP with paranodal antibodies (NCT03864185).
4 NEUROPATHY WITH ANTIBODIES TO MYELIN ASSOCIATED GLYCOPROTEIN (ANTI-MAG-NEUROPATHY)Anti-MAG neuropathy is a distal demyelinating neuropathy, distinct from CIDP, characterized by sensory ataxia and tremor. This case demonstrates the typical pathological finding of widely spaced myelin (WSM) on electron microscopic examination, which helps to confirm the diagnosis of this neuropathy.
4.1 Patient historyA 68-year-old man noticed unsteadiness of gait at 65 years of age. Numbness in the toes appeared 1 year later and gradually spread to the lower legs and hands. He became aware of tremor in his hands at 67 years of age. As the unsteadiness and numbness gradually progressed, he was referred to our hospital for further investigation. Although a mild degree of glucose intolerance was previously noted, he had no other remarkable personal or family history. Autonomic symptoms were not noted.
4.2 Neurological examinationCranial nerves were intact. Distal predominant weakness was present bilaterally in both the upper and lower extremities. His grip strength was 9/7 kg (right/left side). A sensory deficit was noted in a distally accentuated glove and stocking pattern. Light touch and pain were mildly impaired, while vibration was severely reduced in the distal portions of the lower limbs. Joint position sensation was moderately reduced in the toes. Romberg's sign was positive. Deep tendon reflexes were absent in all four limbs. The plantar responses were flexor bilaterally.
4.3 Laboratory tests, electrophysiological, and imaging studiesCerebrospinal fluid examination revealed an increased protein level (157 mg/dL) and a normal cell count. Nerve conduction studies demonstrated severely prolonged DML and a slowing of MCV in the median and ulnar nerves (12.8 and 8.5 ms for DML, 16 and 15 m/s for MCV, respectively). CMAPs in these nerves were also decreased (0.4 and 2.8 mV, respectively). CMAPs in the peroneal and tibial nerves were not elicited. SCV and SNAPs in the ulnar nerve were 11 m/s and 1.1 μV, respectively, whereas SNAPs in the median and sural nerves could not be elicited. Electromyography of the right anterior tibial muscle revealed fibrillation potentials and positive sharp waves, consistent with active denervation. Brain and spinal MRI were normal. Serum investigations identified an increased level of IgM (994 mg/dL, normal 35-220 mg/dL), and serum immunofixation demonstrated the presence of an IgM-kappa type monoclonal protein. Enzyme-linked immunosorbent assays and western blot analysis indicated the presence of antibodies against myelin-associated glycoprotein (MAG).
4.4 Nerve biopsy findingsSural nerve biopsy revealed mild endoneurial edema and a slight reduction of myelinated fiber density on transverse sections. Teased-fiber preparations showed a mixture of segmental demyelination (6%) with a tomaculous appearance and axonal degeneration (7%). On electron microscopic examination, WSM, defined as two or more wraps of myelin with a regularly separated intraperiod line and an intact major dense line was observed (Figure 3A,B). In contrast, neither demyelination caused by macrophages or onion bulbs were detected. Unmyelinated fibers were well preserved. Thus, the diagnosis of neuropathy with IgM monoclonal gammopathy and anti-MAG antibodies was confirmed.

Representative electron microscopic photographs of widely spaced myelin in patients with neuropathy with IgM monoclonal gammopathy and anti-MAG antibodies. Transverse section of the sural nerve biopsy specimen. Uranyl acetate and lead citrate staining. Widely spaced myelin, defined as two or more wraps of myelin with a regularly separated intraperiod line and an intact major dense line, is observed in the outer layers of the myelin lamellae. A high-powered view of the region shown in the box in A, is shown in B. Scale bars = 0.5 μm A and 0.2 μm B
4.5 DiscussionNeuropathy with IgM monoclonal gammopathy and anti-MAG antibodies (ie, anti-MAG neuropathy) is another demyelinating neuropathy characterized by slow progression and predominant sensory symptoms, particularly sensory ataxia.18 Nerve biopsy specimen studies suggest that the occurrence of widely-spaced myelin (WSM) results from the deposition of IgM and complement on myelin, where MAG is localized.18 As WSM is a characteristic feature, and macrophage-induced demyelination is not found in anti-MAG neuropathy, this neuropathy is now considered to be distinct from CIDP.8 Findings from neuropathy caused by IgG4 antibodies to paranodal components and anti-MAG neuropathy indicate the ongoing use of nerve biopsy to understand the pathophysiology of acquired neuropathy.
5 VASCULITIC NEUROPATHYVasculitis remains a typical indication for nerve biopsy with important treatment implications. This case demonstrates an atypical phenotype of vasculitis with a diagnosis confirmed by typical nerve biopsy features. Thus, indicating the need to consider nerve biopsy in seemingly indolent neuropathies.
5.1 Patient historyThe 54-year-old female patient was admitted for diagnostic work-up of a distal symmetric axonal sensorimotor peripheral neuropathy. She reported sensory deficits and dysesthesia that had started in the feet 8 months prior were slowly progressive and now extended to the distal half of the lower legs. She complained of unsteady gait and loss of muscle strength that started 6 months ago. Further symptoms included Raynaud's phenomenon and intermittent lower limb skin rash, both of which were not evident at the time of review. There was no family history of peripheral neuropathy. The patient suffered from Crohn's disease since 1982 (in remission from 1986 onward) and associated spondyloarthritis.
5.2 Neurological examinationAt the first admission, neurological examination revealed reduced upper limb deep tendon reflexes and absent ankle reflexes. In addition, there was bilateral weakness of shoulder abduction and toe extension. Hypoesthesia and dysesthesia were evident in both feet and distal lower limbs.
5.3 Laboratory tests, electrophysiological studiesRoutine laboratory tests were normal except for slightly elevated C reactive protein (2.19 mg/dL). Vasculitis screening revealed elevated ANA and ASMA titers (1:10240) and elevated rheumatoid factor (IgA 87 U/mL, IgM >500 U/mL). Type 2 cryoglobulins were detected. CSF was completely normal.
5.4 Nerve, muscle, and skin biopsy findingsSkin biopsy revealed reduction of intraepidermal nerve fiber density in the sample from the lower leg (lower leg 3.6 fibers/mm, upper leg: 13.1 fibers/mm) and detected perivascular macrophages and T cells (Figure 4A,B). The latter raised the suspicion of vasculitis and nerve and muscle biopsies were performed.

Photomicrographs of the patient's skin and nerve biopsy. A and B show an immunoreacted skin biopsy (of intact skin) with anti-CD3 (T cell marker, A) and anti-CD68 (macrophage marker, B). Numerous T cells A and macrophages B are found around dermal vessels (arrows), also invading the vessel walls. C-G are photomicrographs of the patient's nerve biopsy. Inflammatory cells in the hematoxylin-eosin stain C are further specified as T cells in immunohistochemistry with anti-Leu4 (T cell marker) D and are found around vessels (arrows) infiltrating the vessel wall of smaller vessels. Photomicrograph of hematoxylin-eosin staining E, immunohistochemistry with anti-CD68 (macrophage marker, F) and Elastica van Gieson staining G of the patient's nerve biopsy. A thrombosed epineural vessel (hematoxylin-eosin, E) with macrophages within the vessel wall (anti-CD68, F), but intact internal elastic membrane in the Elastica van Gieson staining G can be seen. Bar = 50 μm
Sural nerve biopsy showed extensive perivascular inflammatory infiltrates around epineural vessels invading the vessel wall (Figure 4C,D). Three thrombosed vessels could be seen (Figure 4E,F), without intramural fibrinoid necrosis. No fragmentation of the internal elastic membrane, endothelial, or media disruption was observed, and there was no edema (Figure 4G). Immunohistochemical staining with anti-Leu4 (pan T cell marker) and anti-CD68 (macrophage marker), disclosed the presence of macrophages and T cells (CD8-positive T cells) within vasculitic infiltrates (Figure 5B,C). Semithin sections revealed axonal loss, some clusters of regenerating fibers, and some fibers undergoing Wallerian degeneration, but no thinly myelinated fibers or onion bulbs, thus demonstrating axonal pathology (Figure 5D).

Photomicrographs of hematoxylin-eosin stain A and immunohistochemistry with anti-Leu4 (T cell marker, B) and anti-CD8 C of the patient's muscle biopsy, showing inflammatory infiltrates around perimysial vessels (A, arrows), also invading the vessel wall B, C and identified as T cells/cytotoxic T cells B, C. Photomicrographs of a semithin section of the patient's nerve biopsy are shown in D, revealing severe axonal loss, few clusters of regenerating fibers (D, arrow, right inlay) and some degenerating fibers (D, arrowhead, left inlay), but no onion bulbs or thinly myelinated fibers. Bar = 50 μm
Muscle biopsy of the gastrocnemius muscle showed some angular atrophic fibers, nuclear clumps, and fiber type grouping, thus presenting a histopathological pattern of neurogenic atrophy. Vasculitic infiltrates, immunohistochemically characterized as macrophages and T cells, were detected around peri- and endomysial vessels (Figure 5A-C). Definite vasculitis was diagnosed due to invasion of vessel walls by inflammatory cells and acute thrombosis.19
5.5 Work-up regarding systemic vasculitisSonography of the abdomen was normal. CT scan of the thorax showed ground-glass opacity, consistent with vasculitis, and a CT scan of the nasal sinuses revealed maxillary sinusitis. Otorhinolaryngeal evaluation resulted in a diagnosis of chronic sinusitis, and ophthalmological assessment led to a diagnosis of keratoconjunctivitis sicca. FDG-PET revealed evidence of pulmonary, pericardial, and pleural vasculitis. Biopsies of the lung could not definitely confirm pulmonary vasculitis, although this was highly suspected.
5.6 Treatment and follow-upIntravenous methylprednisolone (1 g/d for 3 days) was started immediately after biopsy and was continued as a tapering oral treatment (10 mg/d finally). Due to systemic involvement, according to interdisciplinary consensus with the Department of Rheumatology, treatment with rituximab was initiated. Systemic involvement as well as neurological symptoms improved: Muscle strength recovered except for toe flexors (MRC 5-). Hypoesthesia and paresthesia of the feet remained, but gait was no longer impaired. Nerve conduction studies have not improved to date, with the last measurement performed 7 months after treatment.
5.7 DiscussionThis case presents a patient with the common clinical picture of distal-symmetric axonal sensorimotor neuropathy without evident signs or symptoms of systemic vasculitis (except for Raynaud's phenomenon and skin rash, which were not present at the time of review). The patient finally turned out to suffer from systemic vasculitis and was successfully treated with corticosteroids and rituximab. Diagnosis was predominantly made by nerve, muscle, and skin biopsy.
Vasculitic neuropathy is typically characterized by an acute or subacute onset, multifocal or asymmetric involvement and fast, often step-wise, progression.20 Distal symmetric sensorimotor axonal neuropathy is the most common phenotype of peripheral neuropathies of many etiologies and, hence, may not raise suspicion for vasculitis. However, a distal symmetric neuropathy can be found in up to 40% of patients with necrotizing vasculitis.21 In the present case, skin biopsy provided the first evidence of a possible vasculitic neuropathy that could be confirmed by nerve and muscle biopsy, supporting the potential use of skin biopsy as a diagnostic tool in vasculitic neuropathy.22 Inflammatory cells invading vessel walls were found in the nerve and muscle biopsies, as well as acute thrombosis of a vessel, thus fulfilling diagnostic criteria for definite vasculitis. However, we did not detect any vessel wall pathology, particularly there was no evidence of fibrinoid necrosis or fragmentation of the internal elastic lamina, media or endothelium or vascular hemorrhage. This is not uncommon with a recent study identifying fibrinoid necrosis in only 4% and disruption of endothelium or media in 0% of 16 patients with definite vasculitic neuropathy.23 Although systemic involvement of multiple organs could be determined, histopathological confirmation was restricted to the peripheral nervous system, supporting the importance of sural nerve biopsy, not only in non-systemic, but also in systemic vasculitic neuropathy.
6 NEUROLYMPHOMATOSISNeurolymphomatosis, and less commonly neuroleukemiosis, remains a typical and necessary indication for nerve biopsy. We present the case of a 78-year-old male, with a rapidly progressive, painless polyneuropathy, who was found to have neuroleukemiosis due to chronic lymphocytic leukemia (CLL), demonstrating the ongoing requirement of nerve biopsy to make a correct diagnosis.
6.1 Patient historyA 78-year-old male presented with a 4-week history of rapidly progressive, painless asymmetric proximal, and distal weakness with associated wasting of the intrinsic hand muscles, but no objective sensory examination findings. This was associated with a significant deterioration in gait, from independent mobility to the use of crutches, and impaired function due to the development of profound hand weakness. This occurred on a background of CLL diagnosed 1 year prior.
6.2 Laboratory tests, electrophysiological, and imaging studiesNeurophysiology revealed absent or attenuated sensory potentials with motor conduction block and temporal dispersion at sites of non-compression, and prolongation of F-wave latencies. Needle electromyography showed severe ongoing denervation in the first dorsal interosseus and tibialis anterior muscles with reduced recruitment. The findings were consistent with a severe, subacute, asymmetrical, sensorimotor neuropathy with mixed axonal and demyelinating features. A wide differential diagnosis was considered, including vasculitis, paraneoplastic phenomenon, neoplastic infiltration, AMSAN, or POEMS syndrome.
On initial blood testing, a lymphocytosis was noted (78.1 × 109/l, normal range 4-10 × 109/l), with mild anaemia and hypogammaglobulinemia, and elevated free lambda light chains. Biochemistry, vasculitic, viral, and auto-immune blood screening was negative. Bone marrow biopsy showed 93% lymphoid infiltration with reduced hematopoietic reserve. Subsequent cytogenetic and FISH analysis demonstrated trisomy 12. MRI revealed no nerve root impingement, thickening or enhancement, cord lesion, canal stenosis, or cord compression. Incidentally, prominent lymphadenopathy, measuring up to 3.5 cm, was identified in cervical, supraclavicular, axillary, mediastinal, and para-aortic regions, consistent with CLL. CSF was bland with no atypia seen on cytology or flow cytometry, and a normal protein of 0.36 g/L (normal range 0.15-0.45 g/L).
Vasculitis with pseudo-conduction block was felt to be the most likely etiology, and the patient was treated with a 5-day course of intravenous 1 g/kg methylprednisolone, with limited improvement. As a result, a sural nerve biopsy was performed.
6.3 Nerve biopsy findingsSural nerve biopsy revealed a marked reduction in myelinated fiber density with frequently observed actively degenerating axons (Figure 6A). Teased-fiber preparations revealed active axonal degeneration in 5% of fibers. Extensive perivascular, monomorphic inflammatory cell infiltrates surrounding epineurial, subperineurial, and endoneurial vessels were seen, with wall invasion but no fibrinoid necrosis (Figure 6B-D). Immunohistochemistry identified a CD5+, CD23+, mildly CD20+ clonal population consistent with nerve infiltration by CLL (Figure 6E).

Sural nerve biopsy demonstrating features of neuroleukemiosis: A: marked reduction in myelinated fiber density with active degeneration of axons (white arrows), Toluidine Blue, Scale bar = 0.2 mm B-D: perivascular, monomorphic inflammatory cell infiltrate surrounding and invading, endoneurial B, epineurial C and subperineural D blood vessels (black arrow heads), B: Toluidine blue, Scale bar = 0.02 mm C-D: H&E Paraffin, Scale bars = 0.1 mm; E: Immunohistochemical staining for CD markers demonstrates a CD5+, CD23+, mildly CD20+ population, consistent with CLL, with occasional reactive CD3+ T cells Scale bar = 0.2 mm
6.4 Treatment and follow-upThe patient was treated with a CLL specific chemotherapeutic regimen including Obintuzumab, a CD20 monoclonal humanized antibody, chlorambucil, and dexamethasone. Treatment resulted in rapid and significant improvements in functional status with return to independent mobility within a month of treatment, with mild residual hand weakness and persistence of right-predominant, dorsiflexion weakness. Serial neurophysiology demonstrated minor improvements in previously observed conduction blocks. His white cell count improved to a nadir of 2 × 109/l (normal range 4-10 × 109/l). Over the last 4 years, he has continued to improve to near normalization of power, with residual asymmetrical sensory disturbance to the ankles and neuropathic pain.
6.5 DiscussionNeurolymphomatosis, or more rarely neuroleukemiosis, as depicted in this case, is characterized by the direct infiltration of nerve roots, dorsal root ganglia, plexus or peripheral nerves with clonal populations of lymphomatous or leukemic cells, occurring in 5% of cases of lymphoma.24 Neuroleukemiosis is less commonly seen25-28; however, was well described in the pre-chemotherapeutic era. Peripheral nerve infiltration is described in both acute and chronic leukemias.26 CLL is typically thought of as an indolent disease characterized by lymphocytosis, lymphadenopathy, and B-symptoms, with complications resulting from immunodeficiency, deranged immune responses resulting in auto-immune phenomenon, and treatments. Neuropathy is a less recognized complication, occurring in 2.2% of CLL cases in one cohort,29 resulting from viral infection or as a result of treatment, more rarely due to secondary auto-immune processes (GBS, CIDP), or as a result of cryoglobulinemia or vasculitis. Neurolymphomatosis and neuroleukemiosis have similar clinical phenotype, investigational and nerve biopsy findings and are considered here as similar entities, although most data are derived from neurolymphomatosis cohorts.
In both conditions, a multifocal mononeuritis pattern is most commonly identified, however, a symmetric polyneuropathy with proximal and distal weakness can be found.11, 25, 30 Often invasion of monoclonal cells is more pronounced in the proximal nerve trunks resulting in demyelination and secondary axonal degeneration in distal nerve portions.11 Similarly, neurophysiology can demonstrate partial conduction block, as seen in this case, suggesting segmental demyelination.11, 25, 31 It is important to note that, neurophysiological findings can often fulfill the EFNS/PNS criteria for CIDP, in one series 34% of patients with pathologically or radiologically confirmed neurolymphomatosis.11 As such, a lack of response to IVIg in presumed CIDP should prompt repeat evaluation for alternative etiologies including neurolymphomatosis. Conversely, a response to steroids, in this situation, does not rule out neurolymphomatosis. Axonal degeneration does typically ensue and is, either alone or with demyelinating features, the predominant finding on nerve conduction testing in the chronic setting.11, 31
In some, but not all, cases, there is evidence of meningoradicular disease on CSF cytology or magnetic resonance imaging, and FDG-PET/CT can, non-invasively, identify FDG-avid disease in peripheral nerves.11 It is estimated that the diagnostic yield of MRI and PET in neurolymphomatosis is 80% and 88% respectively.32 Despite this, nerve biopsy remains the gold standard for the diagnosis of neurolymphomatosis and is extremely important for diagnosis in primary disease. As the peripheral nervous system is a sequestered site, with intact blood-nerve barrier, neurolymphomatosis is also a common site of secondary disease recurrence.11, 33 In secondary lymphomatosis a biopsy is not definitively required, however, can be useful if there is any diagnostic uncertainty, or if the neuropathy occurs remotely to the primary lymphoma, thought in remission.25
Sural or focal nerve biopsy specimens typically demonstrate a reduction in myelinated and unmyelinated fiber density, with axonal degeneration observed on teased-fiber preparation.11 Lymphomatous cell infiltration can be seen, often most conspicuously in and around the perineurium, thought due to greater lymphatic flow, with secondary extension to the endoneurium.11 Invading cells can display obvious cellular atypia, and a clonal population can be identified further by immunohistochemical studies and PCR of the infiltrate.11, 34 PCR-based clonality testing is reported to have a sensitivity of 87% and specificity of 95% for identifying a clonal rearrangement in nerve biopsy specimens.34 At sites of infiltration, demyelination is frequently observed, however, interestingly lymphomatous or other immune cells are not commonly seen to directly interact with the nerve or Schwann cell at these sites, suggesting an unknown soluble factor may incite demyelination.11, 35 Distal to sites of demyelination active axonal degeneration is identified with florid macrophage infiltration.11 Infiltrating cells are often seen in a patchy distribution, and as such imaging guided localization of nerve biopsies can increase the sensitivity of nerve biopsy to 88%.32, 36 More aggressive blood-nerve and CSF penetrating chemotherapeutic regimens are required for treatment of both neuroleukemiosis and neurolymphomatosis, and due to the rarity of cases are targeted to the individual.11, 30 As such, identification of the monoclonal population, frequently by nerve biopsy, is essential to guide optimal patient management.
7 ACQUIRED AMYLOIDOSISAcquired, light-chain (AL) amyloidosis, remains a frequent and important indication for nerve biopsy. We present the case of a 62-year-old male who presents with a rapidly progressive sensorimotor neuropathy on the background of a presumed toxic neuropathy. This case demonstrates the importance of nerve biopsy, in the context of negative alternate investigations, to make this important diagnosis.
7.1 Patient historyA 62-year-old male gardener presented with a rapid onset of progressive distal and proximal lower limb weakness, distal sensory loss with peri-oral numbness, and painless ulceration of the toes. In addition, he reported postural hypotension, alternating diarrhoea and constipation, erectile dysfunction, and weight loss of 6 kg over 3 months. There was a background history of a sensory axonal neuropathy with neuropathic pain, which developed 1 year prior. At the time, all investigations were normal, including protein electrophoresis and immunofixation, and the sensory neuropathy was presumed toxic in etiology due to remote, but cleared, hepatitis C and prior alcohol excess.
7.2 Neurological examinationAt presentation, the examination revealed global weakness, areflexia, and glove and stocking sensory disturbance to the elbows and knees, with a sensory ataxia.
7.3 Laboratory tests, electrophysiological, and imaging studiesNeurophysiology confirmed a marked deterioration with absent sensory and lower limb motor potentials, along with superimposed median neuropathies at the wrist. Given the rapidity of progression, the patient's care was transferred to a tertiary neuromuscular center for further investigation and management.
Blood testing revealed normal biochemistry, cell counts, viral, auto-immune, and paraneoplastic screens. No paraprotein was observed, however, lambda light-chain excess was identified 130 mg/L; normal range 5.71-26.3 mg/L), with a kappa to lambda ratio of 0.13 (normal range 0.26-1.65). Cerebrospinal fluid (CSF) analysis was acellular with normal protein and glucose, and negative cytology and flow cytometry. Fat pad biopsy was negative for amyloid. A right hilar mass, with an appearance suggestive of a primary lung malignancy and prominent 1 cm pre-tracheal node was demonstrated on CT scanning of the chest, abdomen, and pelvis. FDG-PET CT, however, identified no regions of abnormal metabolism to suggest an underlying high-grade tumor. An endobronchial ultrasound-guided fine-needle aspiration disclosed a moderate number of reactive lymphoid, histiocytic, and multinucleated giant cells, without malignancy, in the hilar lymph node.
7.4 Nerve biopsy findingsSural nerve biopsy revealed severe reduction in myelinated and unmyelinated nerve fiber density (Figure 7A) with active axonal degeneration (Figure 7A,D). Congo red staining with apple green birefringence was positive for amyloid deposits in the endoneurial and epineurial vessel walls (Figure 7B,C) with positive immunofluorescence for lambda light chains (Figure 7E), consistent with AL-amyloidosis.

Sural nerve biopsy demonstrating typical features of AL-amyloidosis: A: Severe reduction in myelinated nerve fiber density with active axonal degeneration (black arrows), Toluidine Blue, Scale bar = 0.05 mm; B-C: Amyloid deposits in the endoneurial blood vessel wall (white arrow), Congo red stained frozen sections; B: Immunofluorescence with Texas Red filter, C: Congo red stained with transmitted light, Scale bars = 0.05 mm; D: Teased fibers demonstrate active axonal degeneration in 50% of fibers (arrow heads); Formalin-fixed nerve is incubated in 1.3% aqueous osmic acid for 48 hours, washed and suspended in a 2:1 glycerol/water solution and individual fibers are randomly teased from the specimen under a dissecting microscope, Scale Bar = 0.1 mm; E: Immunohistochemical lambda light chain staining of endoneurium (white arrow heads) and endoneurial vessel walls (white arrows), Scale bars = 0.05 mm
7.5 Staging, treatment, and follow-upFollow-up investigations revealed a 10% plasma cell clone on bone marrow biopsy, without bony lesions on skeletal survey. Cardiovascular involvement was identified by increased intraventricular septal diameter (19 mm, normal ≤12 mm) and reduced global longitudinal strain (−13%, normal >−15%) on echocardiogram, along with extensive infiltration of ventricular walls with late gadolinium enhancement on cardiac MRI. Furthermore, proteinuria (5.4 g/24 hours, normal <150 mg/24 hours) was identified without renal dysfunction. Transthyretin gene testing was negative. Consequently, systemic AL-amyloidosis with nerve, cardiac, and renal involvement was diagnosed in the context of a low-volume plasma cell myeloma.
The patient was treated with bortezomib, cyclophosphamide, and dexamethasone chemotherapy with
留言 (0)