
記住我






A 19-yr-old man with a medical history of obesity presented to the emergency department with a 6-mo history of low back pain. The pain began as an intermittent pain localized over the spinous processes in the lower thoracic and upper lumbar spine without radiation. It was described as a dull ache with 3–4/10 intensity and was aggravated by lying down and with movement in all planes. The patient denied alleviating factors and took acetaminophen without relief. Over the past 2 wks, the patient had developed worsening of the pain, now described as a constant, “stabbing” pain rated as an 8/10. The patient now had radiation of the pain into his left leg down to his foot consistent with a L3 and L4 distribution. He also had weakness throughout his bilateral lower limbs, worse in his ankle dorsiflexors resulting in a foot drop, leading to frequent falls. The patient denied symptoms related to bowel, bladder, or saddle anesthesia. He was eventually unable to ambulate and required a wheelchair for mobility, which caused the patient to come to the hospital for evaluation.
Physical examination revealed an obese man in no acute distress. Cranial nerve examination was unremarkable. Inspection of the back revealed no deformities, skin changes, or muscle atrophy. The patient experienced severe point tenderness over the spinous processes of T11, T12, and L1. Manual muscle testing revealed 5/5 strength throughout the upper limbs. He had 2/5 strength in the bilateral hip flexors, knee flexors, knee extensors, and ankle plantar flexors with 0/5 strength bilaterally with ankle dorsiflexion and toe extension. Sensation was intact to light touch, pinprick, and temperature in the bilateral lower limbs. The pain was exacerbated with straight leg raise in the left lower limb. Patellar and Achilles reflexes were 1–2+ bilaterally with absent clonus. Patient had a negative Babinski sign.
DIFFERENTIAL DIAGNOSISThe differential diagnosis is concerning for an injury to the spinal cord or spinal nerve roots because of the presence of both bilateral strength deficits in the lower limbs and bilateral pain. Most importantly, surgical emergencies, such as spinal cord infarction, spinal cord compression, cauda equina syndrome, and conus medullaris syndrome, must be ruled out. Certain “red flag” questions must be asked to promptly rule these conditions out, such as the presence of profound weakness or sensory disturbances, saddle anesthesia, and bowel or bladder dysfunction (Table 1). It is important to assess for the presence of multiple “red flags” in these instances as a systematic review has shown that in isolation, the diagnostic accuracy of these questions is low, but the combination of multiple “red flags” should raise suspicion for serious pathology.1
TABLE 1 - Red flags as diagnostic clues Myelopathy/cauda equina syndrome • Bowel/bladder incontinence • Loss of anal sphincter tone • Sexual dysfunction • Saddle anesthesia • Progressive/severe motor weakness Cancer • History of cancer • Fever • Unexplained weight loss • Night pain • Failure to improve with conservative management Infection • Fever • Intravenous drug use • Recent infection • Immunosuppression • Steroid use • Failure to improve with conservative management Fracture • History of trauma • Steroid use • History of osteoporosisImaging is rarely indicated in the evaluation of acute low back pain. In patients with low risk for a serious underlying condition, such as cauda equina syndrome, fracture, cancer, or spinal infection, imaging can be deferred in favor of a 6-wk trial of conservative management.2 Unnecessary imaging can lead to radiation exposure, invasive procedures, and increased cost to the patient and healthcare system. In this patient who presents with acute on chronic axial low back pain, however, imaging is warranted. The choice of imaging modality is dependent on the possible diagnosis, the acuteness of the diagnosis, and any comorbidities that may affect the ideal imaging modality, such as renal failure limiting the use of contrast or retained metal preventing the use of magnetic resonance imaging (MRI).2 In the presence of “red flag” symptoms, MRI of the spine with and without intravenuos contrast is likely the best radiologic procedure depending on the specific indication.2 Superior imaging of the bony structures to assess for fractures, spondylosis, and stenosis can be obtained with computed tomography; however, computed tomography is less useful for detailing soft tissue pathology.2,3 Computed tomography with myelography can be useful if MRI is unable to be obtained as it can assess the patency of the spinal canal through injection of contrast into the subarachnoid space.2
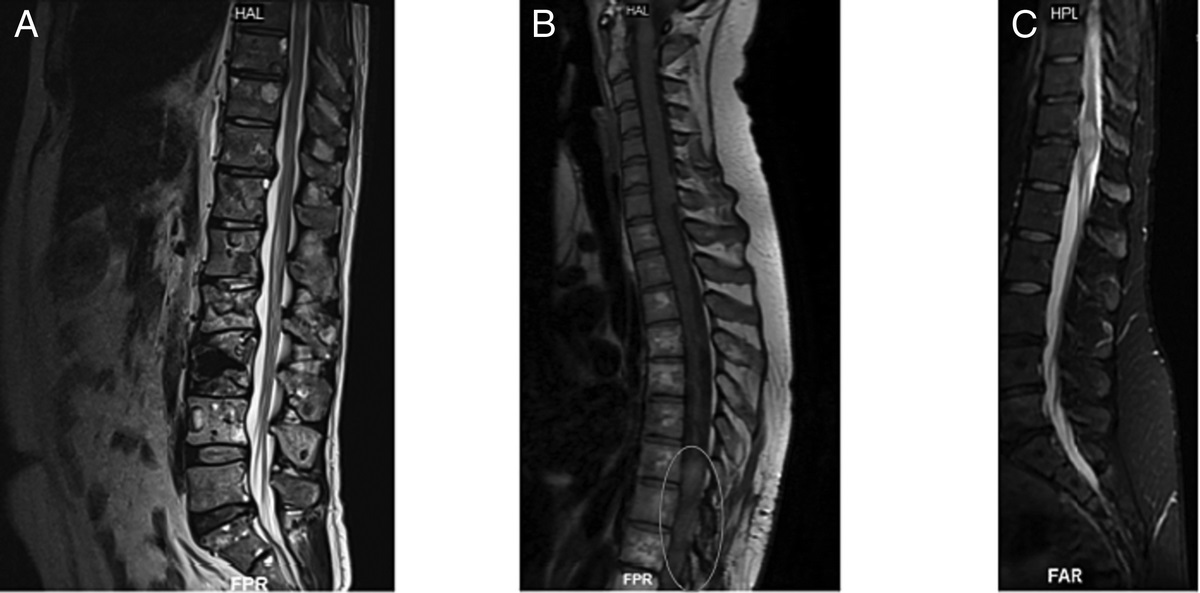
DIAGNOSTIC STUDIESIn the emergency department, x-ray of the thoracolumbar spine with anterior-posterior and lateral views showed no acute fractures, normal vertebral alignment, and no degenerative changes (Fig. 1). Magnetic resonance imaging with and without intravenuos contrast of the cervical, thoracic, and lumbar spine revealed a large, heterogeneous, multicystic mass arising at T11 (Fig. 2A) compressing the spinal canal (Fig. 2B). There was also enhancing tissue around the cystic foci that seemed to displace but not invade the dural sac. There was no disc bulge, herniation canal narrowing, or foraminal narrowing. The vertebral bodies all had normal alignment and height. The differential diagnosis for a spinal mass varies based on the epidemiology, location, and imaging findings of the mass (Table 2). The radiologic differential diagnosis for a heterogeneous multicystic mass includes an aneurysmal bone cyst, giant cell tumor, osteoblastoma, and osteosarcoma.3
 FIGURE 1:
FIGURE 1: Thoracolumbar spine x-ray showing no acute fractures, normal vertebral alignment, and no degenerative changes.
 FIGURE 2:
FIGURE 2: Sagittal (A) and axial (B) views of a T2-weighted MRI of the thoracolumbar spine. A large, heterogeneous, multicystic mass arising at lateral T11 and T12 (A) extends into the vertebral bodies and the spinal canal displacing and compressing the dural sac and its contents centrally and to the right (B) with enhancing tissue around a cystic foci that displaces the dural sac measuring approximately 57 × 38 × 74 mm (AP, LR, CC).
TABLE 2 - Typical presentations of common spinal cord tumors Population Tumor Location MRI Findings Ependymoma Adult Intradural Intramedullary T1: Isointense or hypointenseaMost common tumor overall.
Neurosurgery was emergently consulted given the compression of the mass on the spinal canal and the progressive weakness. The patient underwent T10, T11, and T12 laminectomies, resection of the epidural spinal tumor, and pedicle screw fixation with posterolateral arthrodesis with both locally harvested and cancellous chip allograft. A biopsy of the mass was sent to pathology, which was found to be a highly cellular neoplasm containing a mixture of cells with spindled cytology as well as multinucleated giant cells. It also contained blood-filled cystic spaces and dilated venous structures with multifocal regions of osteoid formation. While the pathologic differential included a giant cell tumor variant or an osteosarcoma variant, it was ultimately determined that this was a solid variant of an aneurysmal bone cyst.
PATIENT OUTCOMEThe patient was subsequently admitted to our acute inpatient rehabilitation hospital and found to be an L1 ASIA Impairment Scale grade D on the American Spinal Injury Association Impairment Scale. His pain was largely improved by the operative resection of the mass. Some nociceptive pain persisted but was controlled with acetaminophen, ibuprofen, and oxycodone. Over the next 2 wks, the patient progressed in his mobility from requiring maximum assistance with ambulation to ambulating 200 ft with modified independence with a rolling walker. His motor strength progressed in the right lower limb to a 5/5 throughout and in the left lower limb to a 4/5 in the hip flexors and 5/5 in the knee and ankle flexors and extensors. Parents and friends of the patient were involved early and throughout the process to help the patient cope with his injury as well as training in providing functional support. The patient has been followed in the outpatient setting for 5 mos with continued improvement of his functional deficits and no recurrence of his weakness.
DISCUSSIONThe solid variant of an aneurysmal bone cyst was first reported in 1983 as a lesion with a combination of “fibroblastic, osteoclastic, osteoblastic, aneurysmal, and fibromyxoid elements” and was coined as a “solid” variant of aneurysmal bone cyst.4 These cysts are rare, with a prevalence of 0.14 per 100,000 individuals, and seem to be equally common in male and female individuals.5 The solid variant is even less common, accounting for 3.4%–7.5% of all aneurysmal bone cysts.6 Aneurysmal bone cysts develop most commonly in adolescents during periods of skeletal growth; the median age of discovery is 13 yrs with 90% found before the age of 30 yrs.5 It is a benign lesion that presents with pain and swelling in the affected area, most commonly occurring in the metaphyses of long bones.7 When it occurs in the spinal canal, pain is the most common presenting symptom with weakness and numbness in a spinal nerve distribution often accompanying it.6
Radiologic diagnosis of solid aneurysmal bone cysts can be difficult as it can appear similarly to a malignant bone tumor.3,6 X-ray can be unrevealing and MRI may reveal what is generally described as “fluid-fluid levels,” which results from the layering of blood as well as septations on gadolinium-enhanced T1- or T2-weighted images; however, these septations are less commonly present in the solid variant.6,8 Biopsy with histopathology confirms the disease and is important to differentiate it from a malignant lesion.3,6 For this patient, the radiologic imaging was more consistent with the aneurysmal bone cyst, but the differential also included a telangiectasia osteogenic sarcoma and an osteosarcoma. Histopathological diagnosis was more difficult because of a variety of elements found in pathology (cells with spindled cytology, multinucleated giant cells, less-prominent blood-filled cystic spaces, and multifocal regions of osteoid formation) consistent with not only a solid variant of an aneurysmal bone cyst but also an osteosarcoma variant or a giant cell tumor variant. The management of these cases would drastically differ without pathologic confirmation.
Current recommended treatments for the solid variant of the aneurysmal bone cyst vary but preoperative arterial embolization, followed by total operative resection, and spinal fusion seems to be most successful with the lowest rate of recurrence.6,7 Recurrence is rare, and patients can be surveilled with repeat imaging to monitor, although there are no formal guidelines on this matter.6,7
Patients with weakness from nerve compression from these large masses likely would benefit from rehabilitation.9 The goal of rehabilitation is to improve patients’ functional independence, symptoms, and focus on quality-of-life measures.9,10 Patients benefit from strength and transfer training as well as range-of-motion exercises with both physical and occupational therapies.9 Pain has been shown to be a significant barrier to functional improvement in patients with spinal masses and can be due to the tumor or postsurgical.10 Treatment options include medications, modalities, and further surgery depending on the etiology of the pain.9,10 In the case of this patient, surgical resection of the mass, followed by a 2-wk acute inpatient rehabilitation admission, focused on lower limb strengthening, gait training, and balance re-education, resulted in an improved functional outcome with the patient discharging at modified independence of ambulation.
CONCLUSIONSThe solid variant of an aneurysmal bone cyst is a rare variant that can be mistaken for malignancy radiologically.3,6 It should be included in the differential for adolescent patients with imaging findings suspicious for a malignant bone tumor.3,6 Prompt screening for pathology of the spine with imaging, especially MRI, should be undertaken in patients with a constellation of “red flag” symptoms to determine the presence of any conditions requiring urgent intervention.1–3 Treatment with surgical resection results in the best outcomes with reduced rates of recurrence.6,7 In this condition, biopsy is important to distinguish from any malignant lesion to help guide future treatment.3,6 Patients should be monitored functionally and radiographically periodically for recurrence.6,7 Rehabilitation after surgery likely can improve functional outcomes in these patients.9
This study conforms to all American Journal of Physical Medicine and Rehabilitation Resident and Fellow Section CARE guidelines and reports the required information accordingly (see Supplemental Checklist, Supplemental Digital Content 1, http://links.lww.com/PHM/B202).
REFERENCES 1. Maselli F, Palladino M, Barbari V, et al.: The diagnostic value of red flags in thoracolumbar pain: a systematic review. Disabil Rehabil 2020;19:1–17 2. Patel ND, Broderick DF, Burns J, et al.: ACR appropriateness criteria low back pain. J Am Coll Radiol 2016;13:1069–78 3. Rodallec MH, Feydy A, Larousserie F, et al.: Diagnostic imaging of solitary tumors of the spine: what to do and say. Radiographics 2008;28:1019–41 4. Sanerkin NG, Mott MG, Roylance J: An unusual intraosseous lesion with fibroblastic, osteoclastic, osteoblastic, aneurysmal and fibromyxoid elements. “Solid” variant of aneurysmal bone cyst. Cancer 1983;51:2278–86 5. Leithner A, Windhager R, Lang S, et al.: Aneurysmal bone cyst: a population based epidemiologic study and literature review. Clin Orthop Relat Res 1999;363:176–9 6. Suzuki M, Satoh T, Nishida J, et al.: Solid variant of aneurysmal bone cyst of the cervical spine. Spine (Phila Pa 1976) 2004;29:E376–81 7. Park HY, Yang SK, Sheppard WL, et al.: Current management of aneurysmal bone cysts. Curr Rev Musculoskelet Med 2016;9:435–44 8. Mahnken AH, Nolte-Ernsting CCA, Wildberger JE, et al.: Aneurysmal bone cyst: value of MR imaging and conventional radiography. Eur Radiol 2003;13:1118–24 9. Kirshblum S, O’Dell MW, Ho C, et al.: Rehabilitation of persons with central nervous system tumors. Cancer 2001;92(4 Suppl):1029–38 10. Stubblefield MD, Bilsky MH: Barriers to rehabilitation of the neurosurgical spine cancer patient. J Surg Oncol 2007;95:419–26
留言 (0)