This study is the first to describe a cohort of recurrent MOGCE cases. We discuss clinical presentations, laboratory test results, and imaging features, and compare initial and recurrent episodes. This study improves our understanding of this unique MOGAD phenotype and will help clinicians identify MOGCE in practice. MOGCE still presents some challenges, including misdiagnosis, identification of recurrence factors, and necessity of long-term immunotherapy.
The clinical manifestations of MOGCE are not well-defined, and the initial diagnosis in many cases reported in the literature was delayed or incorrect. Headache is the most common presentation; 100% of MOGCE patients reviewed in this study had headache at first attack, and 44.4% had headache at relapse. MOGCE typically involves severe headache, progressive disease course, and rapid alleviation with immunotherapy [9]. Fever is the second most common clinical symptom, which contributes to the common misdiagnosis of infectious encephalitis. Yuqing et al. reported that 66.7% of MOGCE patients presented with fever [10], which is lower than the 88.9% observed in the present study. It is possible that patients with fever are more likely to relapse; however, additional studies with larger sample sizes are needed to confirm this.The third most common clinical presentation was seizures. They are typically focal-onset, most often present as motor seizures, ictal aphasia, or somatosensory symptoms [11], and have been reported to progress to bilateral tonic–clonic seizures in as many as 77% of MOGCE patients [3, 12].Although the most common clinical symptoms at the time of the first attack were headache, fever, and seizure, these were not the predominant symptoms at the time of recurrence. At relapse, symptoms were more varied and included neurological symptoms such as visual impairment and limb paralysis.
MOG antibody positivity is key to the diagnosis of MOGCE. Valencia-Sanchez et al. reported that initial misdiagnosis occurred in 47% of cases, as isolated CE did not always prompt consideration of central nervous system demyelination and MOG-IgG testing [11].Of the nine patients included in our study, five were initially misdiagnosed because they were not tested for MOG antibodies at the time of the first attack; MOGCE diagnosis was confirmed only at the time of relapse. It has been reported that serum MOG-IgG titer is correlated with disease activity, and that titer is higher in the acute stage than in the remission stage [13]. A high antibody titer [14] and persistent antibody positivity [15] have been proposed to be correlated with the likelihood of recurrence. However, the present cohort of patients with recurrent MOGCE did not display unusually high MOG titers (range 1:10 to 1:100). Additional, multi-center, large-sample studies will be needed to further explore the relationship between MOG antibody titer and likelihood of recurrence.
MOGCE often presents with clinical meningoencephalitis symptoms and abnormal CSF findings mimicking central nervous system infection [16]. Elevated CSF WBC count is common in MOGCE, but rare in other cerebral demyelinating diseases [17]. It has been reported that CSF WBC count increased in 92% of MOGCE cases [18]. In the present review, CSF WBC count was found to be elevated in 7/9 patients (77.8%). CSF inflammation is easily confused with infectious diseases of the nervous system, making early diagnosis difficult. Adequate etiological examination is needed to exclude infection [19]. There was insufficient data to conclude whether CSF WBC count is associated with recurrence; 4/9 cases did not have this information available.
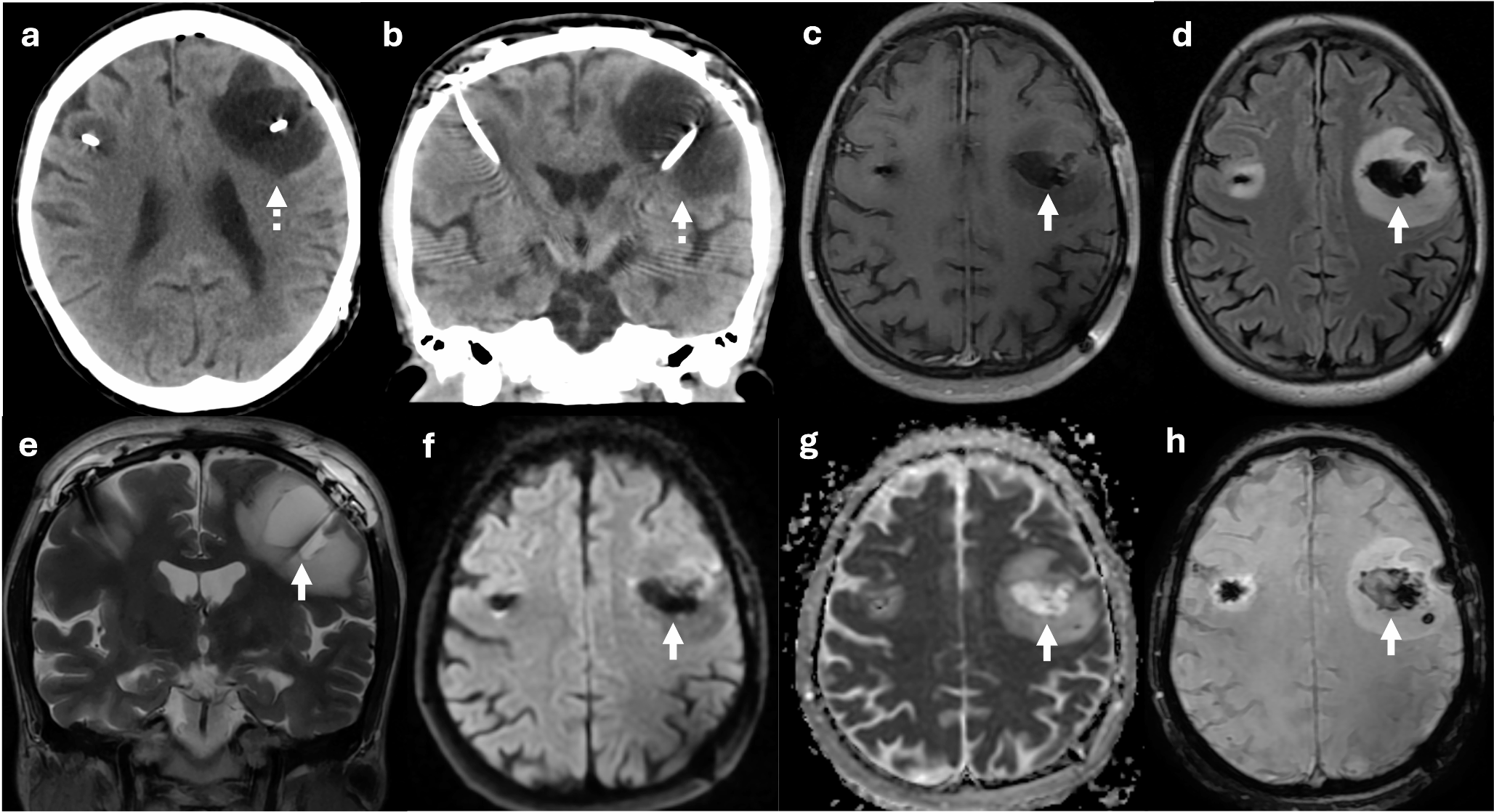
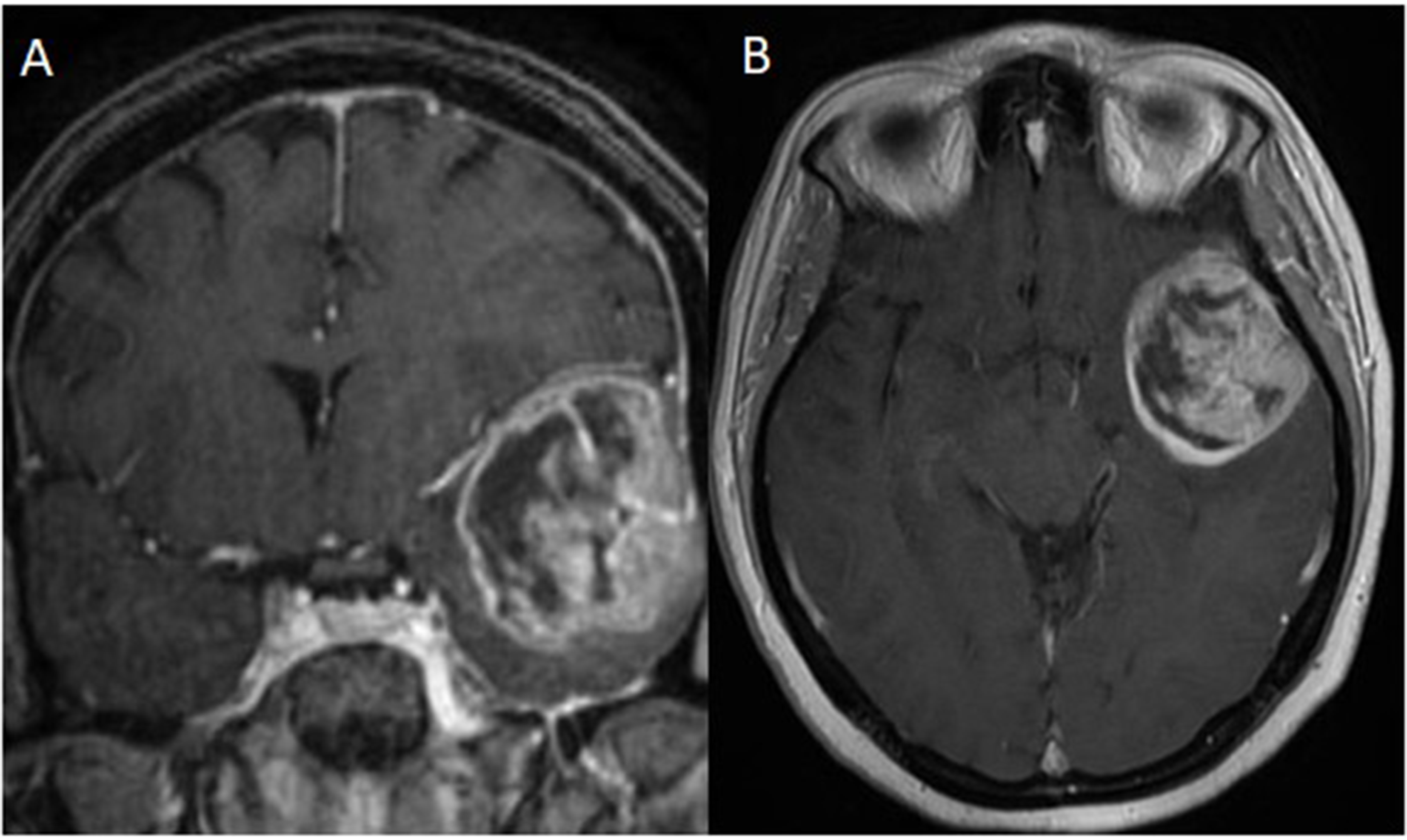
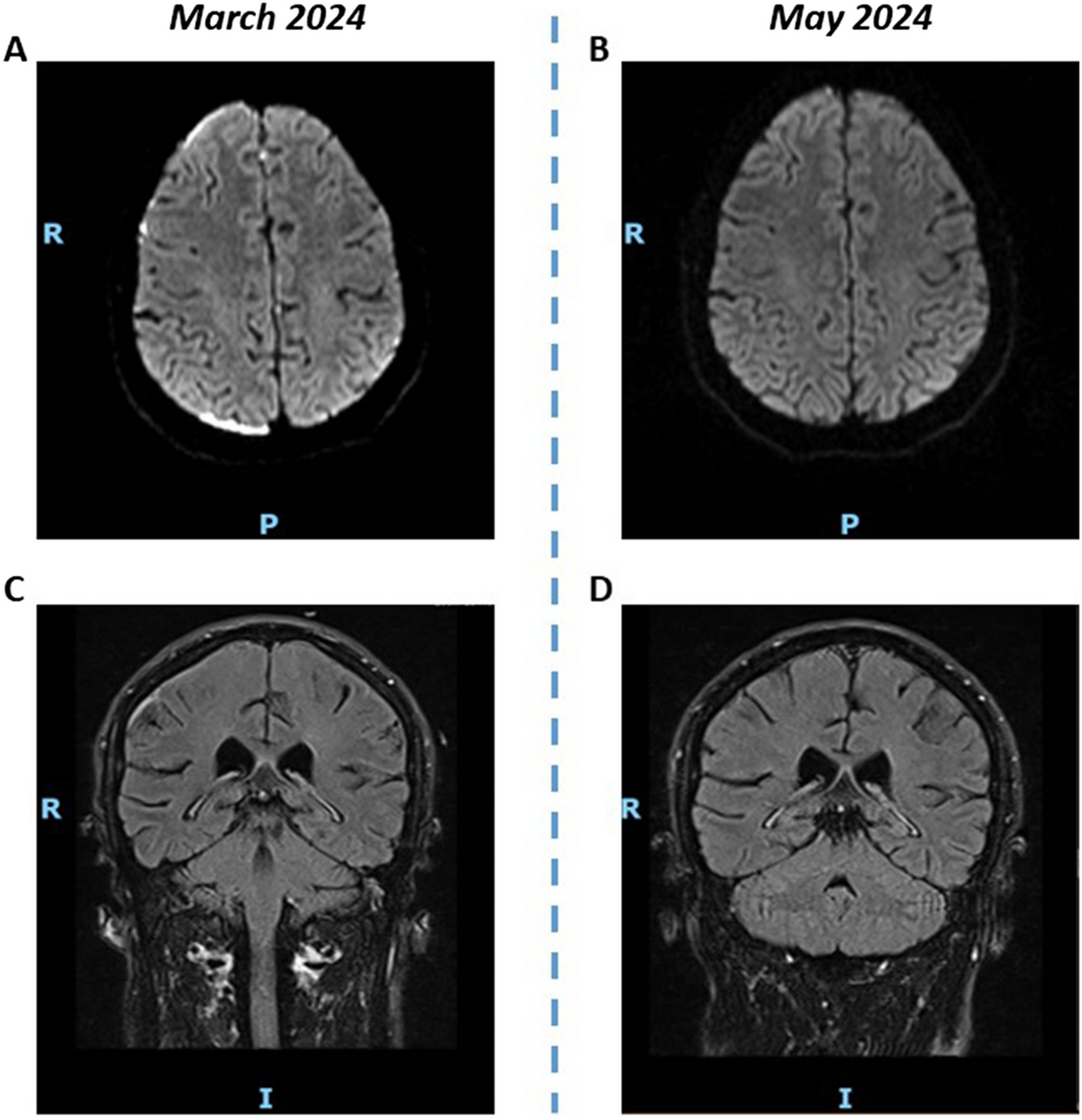
Lesions in MOGCE are typically distributed in the peripheral territories of the anterior cerebral arteries (bilateral) and the peripheral territories of the middle cerebral arteries (unilateral) [20, 21].In the present study, four presenting with bilateral cortical lesions and five with unilateral cortical lesions at the first attack. At relapse, four patients presented with lesions in spinal, brainstem, grey matter, and basal ganglia regions and the other five patients presented with cortical lesions. Similarly, Horita et al. reported that MOGCE can manifest with a variety of phenotypes over time in the same patient [22]. An Austrian case report also showed extensive, predominantly cortical demyelinating lesions with extension into subcortical white matter [23].Together these observations demonstrate that MOGCE is a disease that can affect multiple locations within the central nervous system over time, and is not limited to the cortex.
Treatment responses vary widely in MOGCE. Intravenous high-dose methylprednisolone and immunoglobulins comprise the standard first-line treatment to combat MOGCE in the acute phase, and usually result in significant improvements in clinical symptoms and imaging. In some patients, however, recurrence occurred after withdrawal from therapy, indicating a high state of disease activity [24].In our study, none of the patients with recurrent MOGCE were taking long-term immunosuppressive drugs after their first onset. Currently, there is no consensus on the necessity of long-term maintenance therapy for MOGCE patients at first attack [25, 26]. When recurred, 8 out of 9 patients had a good prognosis after immunotherapy in our study. Therefore, considering the low recurrence rate of MOGCE and the obvious effect of immunotherapy after recurrence, patients with MOGCE may not need long-term immune maintenance therapy at the first episode.But this conclusion needs further confirmation. It is clear that recurrent MOGCE requires long-term use of steroids or immunosuppressive therapy, such as mycophenolate mofetil, rituximab, and tacrolimus, to prevent relapse again.
This study has some limitations. First, it is a retrospective literature review in which no comparison was made between relapsed and non-relapsed MOGCE. Second, the sample size was relatively small. Finally, it was unable to identify a factor that can predict whether or not a patient with initial MOGCE will experience relapse. Further prospective studies with larger sample sizes and longer follow up are warranted to estimate the likelihood of MOGCE relapse.
In conclusion, recurrent MOGCE is a disease that can affect multiple locations within the central nervous system over time, and is not limited to the cortex. Factors contributing to the likelihood of disease recurrence remain unclear. Patients with recurrent MOGCE do not require unusually high MOG titers. Whether long-term treatment is needed during the first episode is uncertain, but long-term immunotherapy is required after recurrence. Currently, research on recurrent MOGCE is limited and requires further exploration.




留言 (0)