
記住我








A 44-years-old female went to hospital mainly because of "upper abdominal pain for 17 days". In the early morning of Feb. 12th 2023, she had a sudden severe and persistent epigastric pain without obvious inducement, accompanied by vomiting. She went to local hospital and took the blood routine with a result of leukocyte is 7.77 × 109/L, in which neutrophil% (Neut) is 74%, hemoglobin (Hb) is 71g/L, platelet (Plt) is 393 × 109/L. Liver and kidney function, myocardial enzyme, amylase were normal. Within 4 h, the Hb decreased to 45g/L rapidly, with abnormal coagulation function including prothrombin time (PT) 45s, partial thromboplastin time (APTT) 38s, fibrinogen (Fbg) 1.09 → 0.73g/L. Arterial blood gas (ABG) showed a PH of 7.25 with a lactate level of 5.2mmol/L. Enhanced abdominal CT showed a huge retroperitoneal hematoma, abdominal effusion (Fig. 1). On the same day, a right femoral arteriography was performed, no clear contrast medium leakage was found during the operation, so no interventional embolization was performed. She was transferred to the ICU for endotracheal intubation assisted mechanical ventilation, blood transfusion, pain relief on Feb. 13th. With a monitoring level of Hb 80-90g/L. Fever occurred during hospitalization with a Tmax 38.5℃, accompanied by jaundice in skin and sclera. Further more examinations were done, including leukocyte 16–20 × 109/L, Neut% 80%. Liver function included aspartate aminotransferase (AST) 13 → 90u/L, alanine aminotransferase (ALT) 11 → 81u/L, total bilirubin/direct bilirubin (Tbil/Dbil) normal → 156/149μmol/L. Blood culture of aerobic and anaerobic with two sets were both negative. Qualified sputum culture showed Stenotrophomonas maltophilia positive. Enhanced CT was re-examined on Feb. 18th, roughly the same as before (Fig. 2). When the infection state was almost controlled with cephalosporins, she was transferred to a general ward after deventilation and extubation on Feb. 25th. The gastric tube drainage was dark green at the beginning, but with a intermittent bright red—reddish-brown fluid on Feb. 27th. She arrived at the emergency department of our hospital on Feb. 28th. CT scan showed double lower lung cord shadow, bilateral pleural effusion, and huge retroperitoneal hematoma (about 15cm in length), which was roughly the same as before. She was treated with antibiotics, acid inhibition and fluid rehydration, then she was admitted to the emergency generalized ward on Mar. 1st.
Fig. 1
Abdominal enhanced CT scan on Feb. 12.th 2023
Fig. 2
Abdominal enhanced CT scan on Feb. 18.th 2023
Past history: Adenomyosis with anemia was diagnosed in 2021 with a Hb of 70g/L. Total laparoscopic hysterectomy was performed in Sep. 2022, and Hb recovered to 80g/L after surgery. Novel corona virus infection history in Dec. 2022. Hypertension for six years, SBPmax 160mmHg, irregular medication.
Condition of hospitalizationPhysical examination showed that irritability, anemic in appearance, part cooperation, inquiries roughly to the point. Yellow in sclera and skin of the whole body. The upper abdomen was full and tender with a suspicious rebound pain. Improved examination included blood routine with leukocyte 14 × 109/L, Neut% 77.8%, Hb 82g/L, Plt 803 × 109/L. Reticulocyte% 7.39%, with 219 × 109/L. Biochemical function included albumin (Alb) 36g/L, Alt 60U/L, Ast 58U/L, Tbil/Dbil 93.5/75.2μmol/L. Coagulation showed PT 29.8s, APTT 39.1s, Fbg 0.90g/L, D-dimer 1.65mg/L, international normalized ratio 2.67, fibrinogen degradation products 5.5μg/ml. Inflammatory markers, tumor index and immune index had no significant abnormality. Blood smear showed neutrophilrophil 78%, lymphocytes 13%, increased number of platelets, roughly normal shape. A 1:1 mixing test showed both APTT and PT can be completely corrected immediately and t hours later. Blood coagulation factor activities included FVIII 153.4%↑, FXII 49.4%↓, FIX 58.4%↓, FX 6.0%↓. Factor II,V,VII,XI factors were normal. were almost normal.
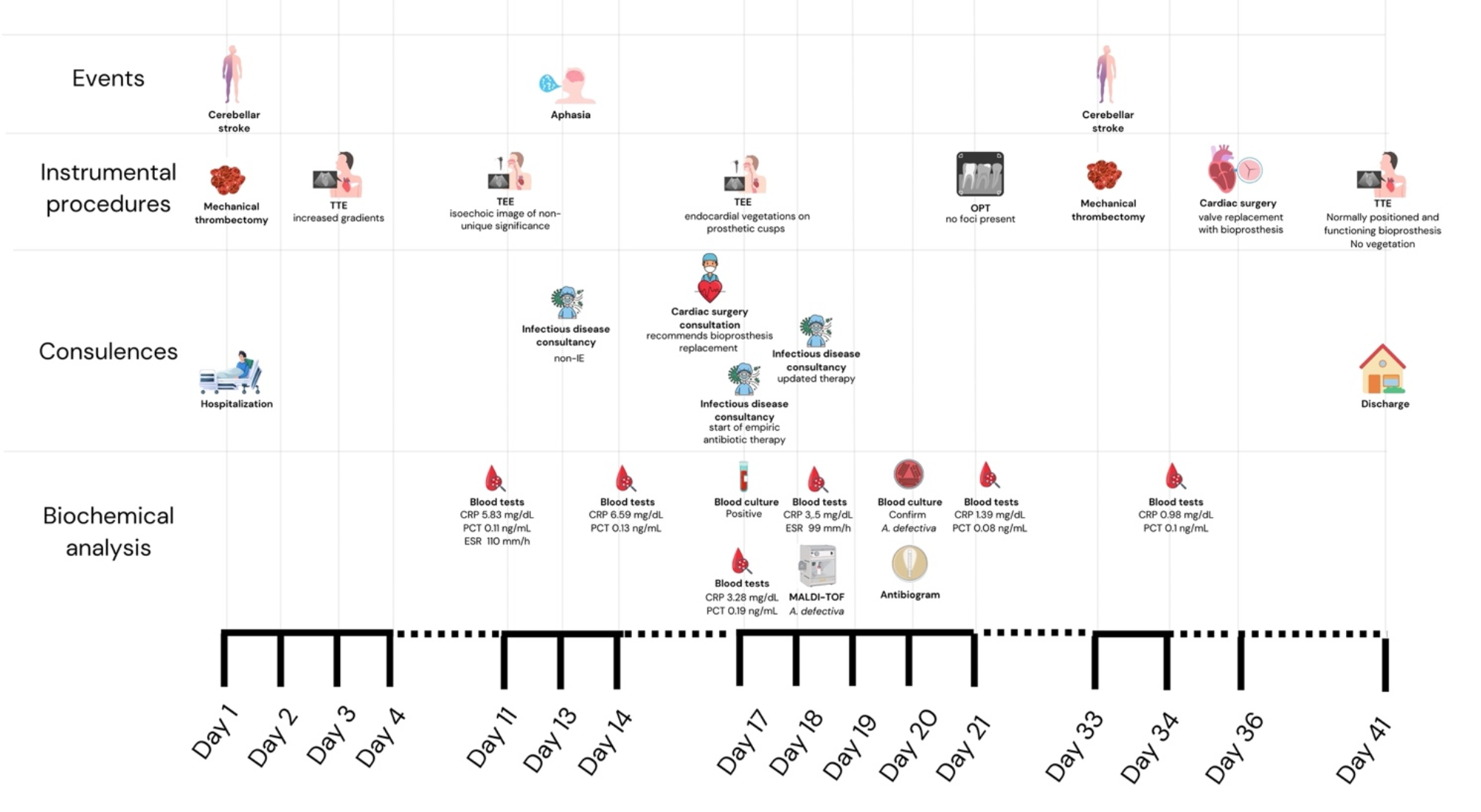
Process of diagnosis and treatmentThe patient had a fever with Tmax of 37.9℃ and intermittent complaints of abdominal pain after admission. She was given plasma infusion to correct coagulation function, piperacillin / tazobactam for anti-infection, cooling, pain relief, and rehydration. Dark green fluid was drained at the beginning of the gastric tube, which turned to reddish brown in the morning of Mar. 2nd. She was treated with strictly fasting for solids and liquids, rehydration, continuously pumping nexium and citrine. At noon, dyspnea and hypoxia occurred with oxyhemoglobin saturation 87–90%@room air → 100%@nasal catheter 5L/min, checking ABG with PH 7.46, pCO2 34, pO2 50, total Hb 72g/L. She was transferred to EICU on Mar. 2nd. Then enhanced CT was taken which showed retroperitoneal hematoma (about 16.9*8.3mm), compression of the superior arteries of duodenum, inferior vena cava, pancreas and mesentery, multiple peripheral exudation and effusion, and no obvious contrast agent extravasation (Fig. 3). Assisted of endotracheal intubation with ventilator, vasoactive drugs and active fluid rehydration were given. Red blood cells, plasma, human fibrinogen, prothrombin complex concentrates (PCCs), vitamin K1 were infused. The etiological examination was gradually improved including urine immunofixation electrophoresis (IFE) showed free λ M protein positive. Blood IFE showed λ positive, the serum free light chain (sFLC) -κ 20.4 mg/L, sFLC—λ 1252.5 mg/L, sFLC κ/λ 0.016. No M protein was found in serum protein electrophoresis (SPE). Cardiac ultrasound showed possible myocardial amyloidosis, bilateral atrium enlargement, moderate tricuspid valve insufficiency. Bone marrow smear showed active hyperplasia, normal morphology, and increased thrombocytosis. The proportion of hematopoietic and adipose tissue is roughly normal in bone marrow biopsy. Special dyeing results showed congo red and potassium permanganate congo red both negative. Under effective treatment the tracheal intubation was removed, and she was transferred back to the general ward. Gradually discontinued nesin and stanine pumps, and continued infusion of vitamin K1, PCCs, plasma infusion and corresponding anti-infection therapy. Subsequently, the patient's symptoms were improved, the gastric drainage was dark green fluid, about 200ml per day, still intermittent night upper abdominal pain, accompanied by acid reflux and heartburn, body temperature was normal since Mar. 4th. The level of Hb was stable (61 → 80 → 99 → 102g/L), and coagulation was slightly improved including PT 25s, APTT 40s, Fbg 1.3g/L. Myocardial biopsy was scheduled. Upper gastrointestinal contrast showed gastric wall peristalsis decreased, contrast agent passed slowly through pylorus, duodenal curvature expanded, and the possibility of duodenal compression stenosis (Fig. 4). The patient was allowed to transit to liquid diet without discomfort gradually. Pathology of myocardium showed some cardiomyocytes were deformed, individual blood vessel walls in the interstroma were thickened, and a little powdery stain deposition was seen around the blood vessel walls. Combined with special staining, it was considered amyloidosis. Immunohistochemical results were κ partial positive, λ positive. Special staining results were congo red focal, potassium permanganate congo red focal, alcoholized congo red all positive, but masson staining negative. Delivered myocardium pathology showed κ negative, λ positive under gold immunoelectron microscopy, consistent with amyloidosis (AL-λ type). Report of abdominal wall biopsy included congo red staining with polarizing lens showed focal apple green double refraction, indicating amyloid deposition. Special staining were fused congo red, congo red focal, and potassium permanganate fused congo red focal all positive. PET-CT showed bilateral ventricles and atria positive, SUVmax 8.2. The metabolism of tongue, spleen, abdominal and pelvic subcutaneous fat and peripheral bone marrow were increased. For further diagnosis and treatment, she was transferred to the hematology department on Mar. 24th. At the same time, the patient developed fever again with a Tmax 38℃considered of infection. After comprehensive discussion by the professional team, it was concluded that the diagnosis of systemic amyloidosis was clear and the primary disease treatment should be started as soon as possible to reduce amyloid deposition and improve the function of affected organs. DBD programs were started on Mar. 29th, specifically including daretumab 800mg every week*8 times (then every 2 weeks *8 times, once every 4 weeks thereafter); bortezomib 2mg, d1, d8, d15, d22; dexamethasone 40mg, d1,d8,d15,d22. The infusion process was successful and her coagulation function were improved obviously. The patient discharged to the local hospital for follow-up treatment. All the disease changes and treatment procedures were showed in Table 1.
Fig. 3
Enhanced CT + CTA of the thoracic and abdominal pelvis on Mar 2.nd 2023
Fig. 4
Upper gastrointestinal contrast using meglumine diatrizoate on Mar 8.th 2023
Table 1 Disease changes and treatment procedures
留言 (0)