In the present study we described the anatomical and functional characteristics of seven patients 12 eyes with GA and performed a genetic analysis finding two novel pathogenic variants in the OAT analysis. Most of the features in the patients studied are consistent to previous reports such as age of first symptoms (second decade of life), being night blindness the most common reported symptom, also most of the phakic eyes had mild to high myopia and some degree of cataract with the need of intervention in 50% in the third decade of life [19, 22].The study by Peltola K et al. made in 35 finish patients reported the mean age of diagnosis at 18 years old, in our study the mean age was 34.2 years old which can translate to a late diagnosis. Central and peripheral nervous system abnormalities (muscular weakness, cognitive and hearing impairment) have been demonstrated in patients with GA by electrophysiological studies and these findings were also presented in some patients in our study [23, 24].
In the ophthalmological evaluation the mean BCVA of 0.5 logMar (Snellen 20/63) was worse than a similar case series of 7 patients with GA where a mean BCVA of 0.26 logMar was reported, this can be explained by the small number of patients studied in both series and the heterogeneity of disease severity. P2 16 years old was blind in one eye secondary to an untreated RRD, interestingly some cases have been reported related to this finding in pediatric patients with GA, with a novel OAT mutation confirmation in one case [25, 26], as pediatric RRD is uncommon even in myopic patients and GA has a very low prevalence worldwide it is important to evaluate if this complication might be another feature included in the clinical manifestations of GA.
In the fundoscopy all eyes presented patches of chorioretinal atrophy in different amounts which tended to be more coalescent in the older patients except for P1 who was 10 years old and presented an advanced stage of the disease. Another clinical finding which needs a special mention was presented in P6 (54 years old), with a well-defined area of atrophy in the macula separated from the peripheral atrophic patches by an area of preserved retina at the equator in both eyes, this is different to what has been classically described where the atrophy starts in the mid-periphery and spreads to the macula and the ora serrata in the more advanced stages [7], as we don’t have previous images of this patient we can only suggest but not proof a different pattern of atrophic changes in patients with GA that also start at one point of the disease in the posterior pole and not only in the periphery (Fig. 1). We found this pattern with similar characteristics by the fundus image of two patients presented by Sergouniotis et al. [19].
FAF findings were consistent to the atrophic area in all cases, with some degree of hyperautofluorescence in the border of the preserved retina as mentioned before [19]. With the use of ultra-wide field autofluorescence, P2 and P3 (siblings) showed an interesting pattern with an evident hyperautofluorescent ring outside the arcades that separated the retina with normal autofluorescence posteriorly from the mid-periphery retina anteriorly with subtle hypoautofluorescence that did not show the same degree of autofluorescence found in the chorioretinal patches in far-periphery retina (Fig. 1). By this finding in these two patients 3 eyes, we can suggest that an initial RPE damage that is not clinically visible can precede the chorioretinal patches of atrophy which might be evidenced by the FAF. Measuring this hyper-AF ring in patients with initial damage could work as an indicator of progression and to do a more accurate follow-up.
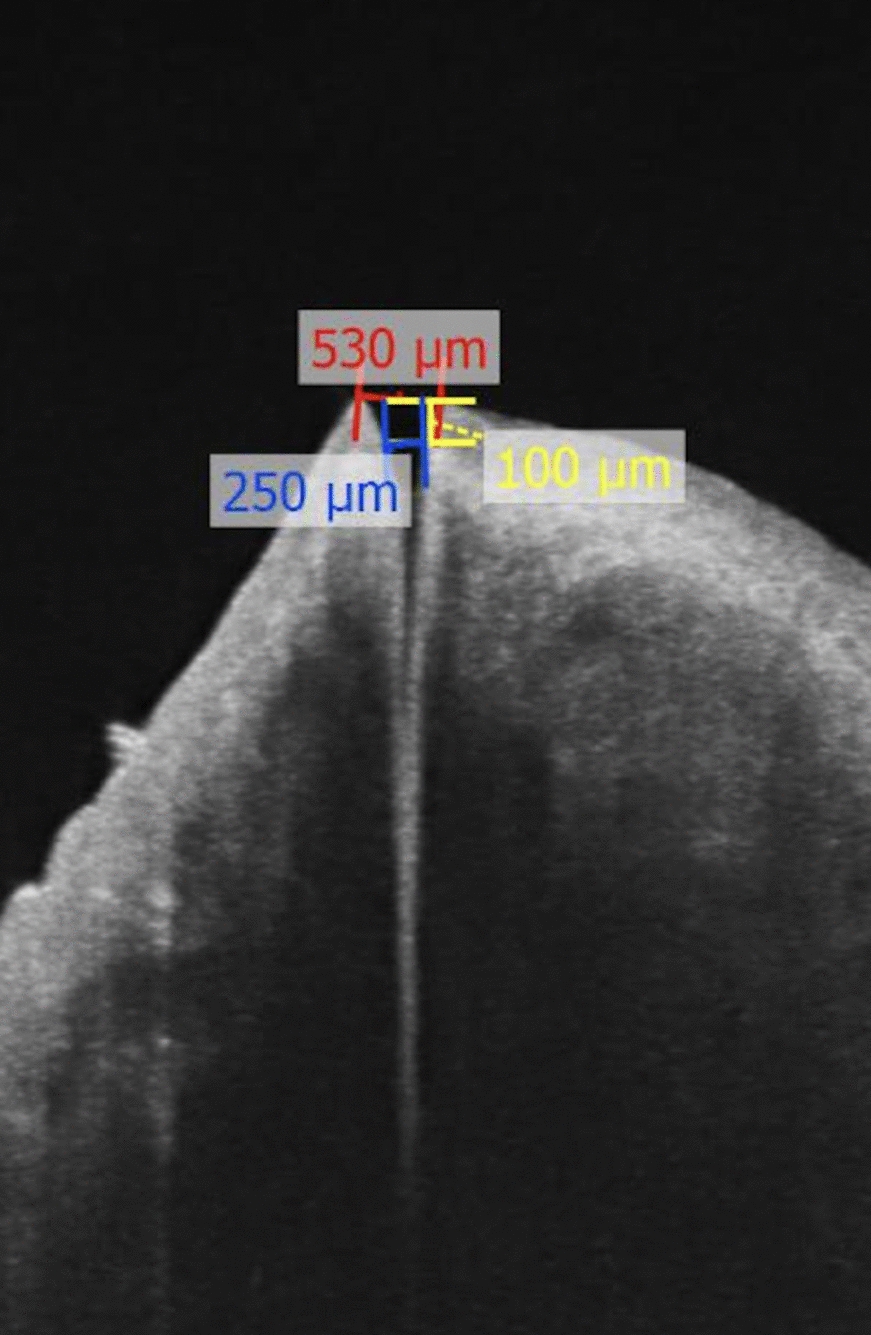
In our study, CME was found in 50% of the eyes studied which differs from the 100% of eyes described in Sergouniotis et al. case series [19]. This specific finding can be explained by a disruption of the outer blood-retinal barrier in the parafoveal area leading to a diffusion of fluid toward intraretinal spaces, maybe a lower incidence of this finding in our study could be attributed to the fact that the patients who did not present intraretinal cyst had a more preserved parafoveal area. CME in this type of retinal dystrophy has been treated with topical and oral carbonic anhydrase inhibitors, topical non-steroidal anti-inflammatory drugs, intravitreal or subtenon steroid injections, restriction of arginine in diet and vitamin B6 supplementation with widely range of response [27, 28]. Half of the patients presented ORT, the youngest patient (P1, 10 years old) with very advanced damage also presented this finding which demonstrates that the ORT can be considered as an indicator of the stage and marker of severity of the disease as mentioned before [29]. The intraretinal hyperreflective deposits found in the ganglion cell layer had been reported previously [19], usually found near the chorioretinal atrophy, in our study found these deposits along all the preserved macula, a gliotic process due to cell death has been hypothesized in a mice model study. In our study we found more accumulation of these deposits in the patients with chronic macular edema, where they seem to coalesce and form a band-shape zone.
Interestingly, the visual field constriction found in the GP mainly in isopter I4e and the generalized decrease in sensitivity response by the topographic functional evaluation of the cones and rods response separately with scotopic and photopic perimetry in all of eyes was more severe than the clinical changes visible on fundoscopy, making these two functional objective studies parts of the follow-up evaluation of patients with GA (Fig. 2).
Although it was not possible to make a correlation between the severity of retinal degeneration and ornithine levels as the measurements were done in a cross-sectional manner, we found a lower mean of elevated plasma ornithine levels of 586 µmol/L (excluding the patient with normal values) than reported in the finnish and japanese case series, 960 and 975 µmol/L respectively [19, 22], nevertheless the variability of the disease’s severity was quite similar. The possible explanation for this finding could be related to the differences in diet between populations, but this must be properly studied. Furthermore, P5 (47 years old) with a homozygous OAT pathogenic variant had normal ornithine plasma levels at the time of the diagnosis, without any diet modification or treatment (Table 1). Previous studies have reported patients with normal ornithine levels and clinical findings corresponding to GA but with no genetic confirmation [30,31,32,33,34] naming these patients “GA-like phenotype”.
To date, this is the first reported case of GA confirmed by genetic testing with normal ornithine levels. It is important to note that we didn’t have the opportunity to repeat the ornithine level measurements in this patient. In such cases, it is recommended to perform the measurements at least three times to confirm the results. This supports the theory proposed by the authors mentioned before that there might be more than one pathophysiological mechanism within the metabolic pathways of ornithine and arginine, leading to an accumulation or a decrease of substrates that eventually produce chorioretinal degeneration. This should be evaluated in more studies in the future.
Pathogenic OAT variants were identified in all GA patients from this cohort. Interestingly, 50% of disease-causing mutations (6/12) corresponded to the novel c.721_722dupCC (p.Asp242ArgfsTer6) variant, which was observed homozygously in two cases and in compound heterozygosity in two additional patients. While additional haplotype studies will be needed, our preliminary data supports that the c.721_722dupCC variant could be a founder OAT mutation in Mexico. A second novel OAT variant, corresponding to c.796C > T (p.Gln266*), was identified in a single allele in this group of patients (Table 2).
Patients included in this study were referred to a specialist in metabolic nutrition to implement an arginine-restricted diet, ensuring careful consideration of nutraceutical components to prevent malnutrition-related disorders. This dietary intervention was meticulously designed to balance the reduction of arginine intake while providing all essential nutrients, thereby safeguarding against the potential risks of dietary insufficiencies. The collaboration with nutritional experts highlights the importance of a multidisciplinary approach in managing complex metabolic conditions.
In conclusion, the present study expands our knowledge of the clinical and genetic features of GA in the Mexican population. This study provides new information regarding functional and structural diagnosis to use in the future and evaluate if these tools can help us make a more accurate diagnosis on staging of the disease and a better follow-up to the patients under treatment. The most frequent mutations as well as the novel molecular findings in the Mexican population have important implications for the future genetic diagnosis of GA, allowing us to identify carriers of the disease and also study the genotype–phenotype correlation in larger studies in the future.
Clinical studies on retinal dystrophies are imperative for a deeper understanding of the disease’s clinical course. Identifying the most precise clinical variables that measure disease progression is crucial, as these indicators are integral to the meticulous planning of gene therapy clinical trials aimed at slowing or halting disease advancement. Such trials depend heavily on accurate, reproducible clinical endpoints that not only reflect the true nature of the disease's progression but also offer measurable targets for therapeutic intervention.









留言 (0)