
記住我








This retrospective study utilized hospital discharge records from the National Inpatient Sample (NIS) for the years 2020 and 2021. The NIS is a component of the Healthcare Cost and Utilization Project (HCUP), funded by the Agency for Healthcare Research and Quality (AHRQ) [20]. The NIS sampling frame encompasses data from 48 statewide data organizations, including 47 states plus the District of Columbia, representing approximately 98% of the U.S. population. It includes a stratified 20% sample of discharges from U.S. community hospitals, excluding long-term acute care hospitals and rehabilitation facilities. The NIS ensures patient confidentiality because of the de-identified nature of data. A detailed description of the database is available on the HCUP website [20].
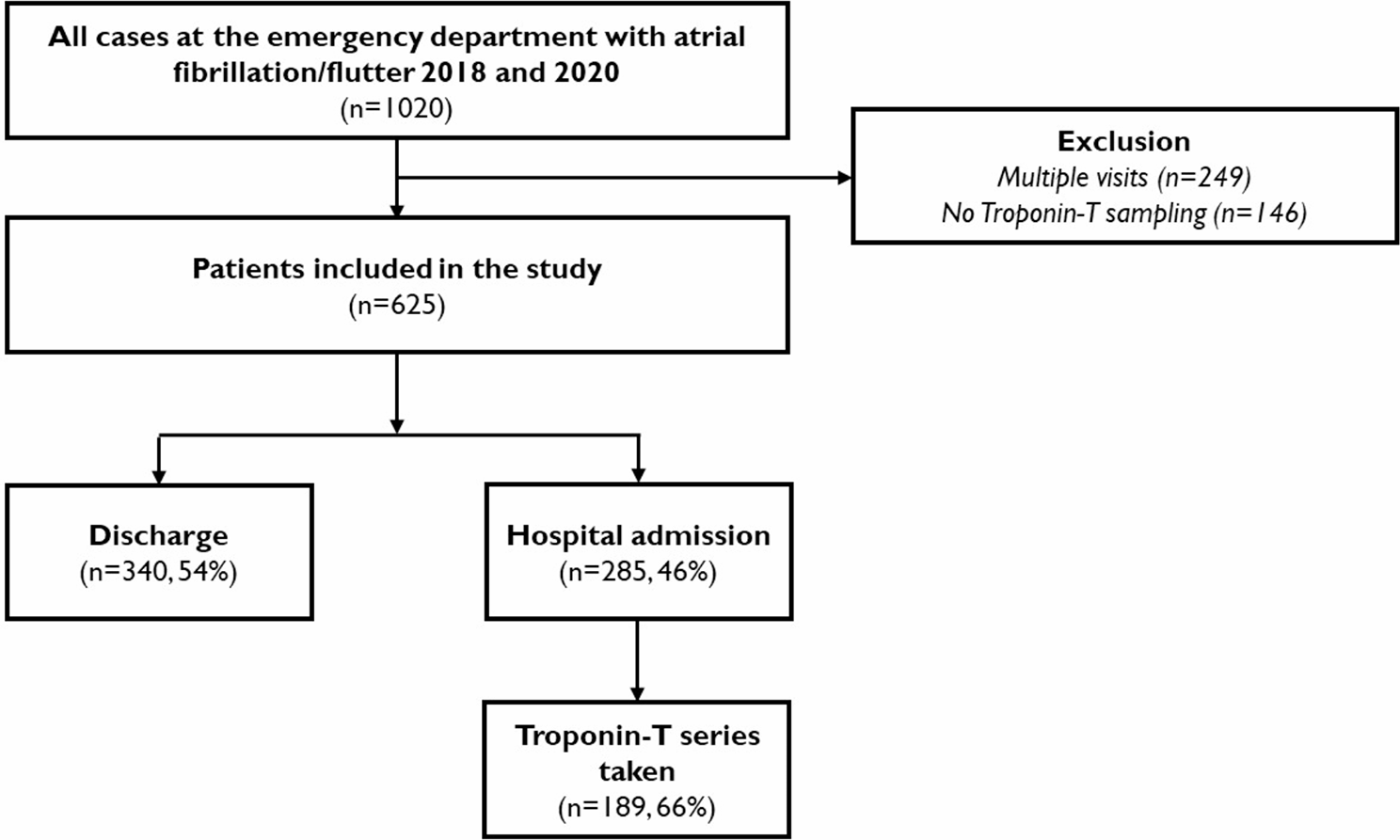
Our study focused on individuals aged 20 years or younger who were hospitalized with a diagnosis of COVID-19, influenza, or respiratory syncytial virus (RSV). The International Classification of Diseases, Tenth Revision, Clinical Modification (ICD-10-CM), was utilized to identify hospitalized children diagnosed with COVID-19, influenza, RSV, and other variables studied. To minimize confounding effects, we excluded individuals with co-respiratory infections (i.e., those diagnosed with more than one of the studied viral infections: COVID-19, influenza, or RSV) and those who were transferred between hospitals to prevent double counting (Fig. 1).
Fig. 1
Flow diagram for in-hospital admission for COVID-19, influenza and RSV infection
To identify COVID-19 cases within the database, we utilized the ICD-10-CM code B97.29 for records from January 1 to March 31, 2020, and U07.1 for records from April 1, 2020, onward [21]. For RSV infection, the following ICD-10-CM codes were employed: B97.4, J12.1, J20.5, and J21.0. We excluded cases of bronchiolitis that did not have a corresponding RSV diagnosis. We excluded admissions that did not have complete data for analysis.
Severity, used as a variable in the analysis, denotes the severity of illness and has four categories: 1) minor loss of function, which includes cases with no comorbidity or complications; 2) moderate loss of function; 3) major loss of function; and 4) extreme loss of function [22].
Outcome variablesThe primary outcomes were in-hospital mortality and major cardiovascular complications associated with COVID-19, influenza, or RSV infection. For the purpose of analysis, major cardiovascular complications were myocarditis, tachyarrhythmia, bradyarrhythmias/heart block, sudden cardiac arrest, and the need for extracorporeal membrane oxygenation (ECMO). Additionally, we compared disease severity and length of hospital stay across the study groups. The ICD-10 codes corresponding to the diagnoses and procedures analyzed in this study are presented in supplementary Table 1.
Statistical analysisWe conducted both descriptive and inferential analyses, followed by logistic regression modeling, to evaluate the data. Given that the NIS is a complex survey dataset, we incorporated clusters, strata, and weighting as recommended by the Healthcare Cost and Utilization Project (HCUP) to generate national estimates and ensure the accuracy of the statistical analyses. Continuous variables, such as age, length of stay, and disease severity, were reported as medians with interquartile ranges. Categorical variables were analyzed using weight-adjusted chi-square tests.
For multivariable analysis, we selected variables with reliable and consistent ICD-10 codes. Initially, univariable regression analysis was performed for variables of interest, followed by multivariable regression analysis that accounted for additional covariates, including age group, sex, asthma/reactive airway disease, prematurity, obesity, diabetes, congenital heart disease, chromosomal anomalies, ZIP code of household neighborhood, and disease severity. These covariates were identified through a comprehensive literature review and clinical expertise and were finalized prior to conducting the analyses.
The patient’s ZIP code was categorized into quartiles based on the estimated median household income of residents within that ZIP code, with quartiles representing the range from the lowest to highest income, indicating the poorest to wealthiest populations. All statistical analyses were conducted using Stata statistical software (version 15.1) and R (version 4.3) with RStudio (version 1.2). Figures were generated using the ggplot2 package in R [23].
留言 (0)