
記住我





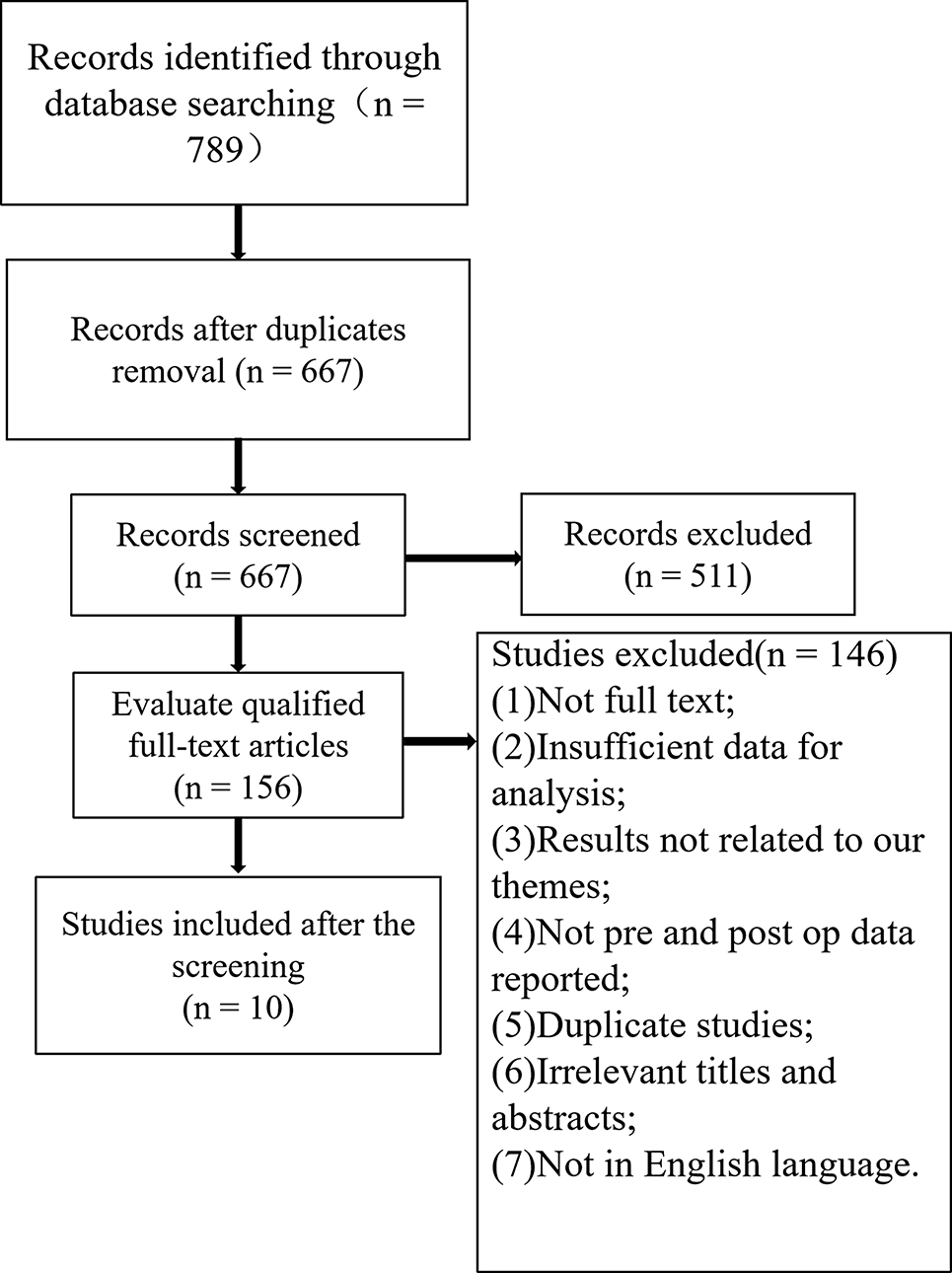
This study included cases from HIV-positive patients diagnosed with osteonecrosis of the femoral head who presented to our orthopedic department between 2011 and 2022.
Inclusion criteria for the study group 1.Confirmed diagnosis of HIV infection, according to the Guidelines for the Diagnosis and Treatment of AIDS [18].
2.Diagnosis of osteonecrosis of the femoral head (ONFH) confirmed by clear radiographs or MRI, categorized as ARCO stage IIIb or IV, with indications for surgery and total hip replacement (THR), as well as perioperative management according to the Enhanced Recovery After Surgery (ERAS) protocol, which includes antiviral therapy, nutritional enhancement, and immune system support.
3.Informed consent obtained from all patients.
Exclusion criteria 1.Patients with severe concurrent primary diseases of the heart, liver, kidneys, or hematopoietic system that precluded surgical intervention.
2.Patients who did not provide informed consent.
3.Patients unable to continue follow-up or who lost contact.
The control group met the same inclusion criteria as the study group; however, perioperative management was conducted according to the Traditional Protocol (TP).
Exclusion criteria for the control group 1.Presence of other hip joint diseases (e.g., primary osteoarthritis, rheumatoid arthritis), skin lesions near the hip joint, lumbar intervertebral disc herniation, diabetes mellitus, tuberculosis, chronic infections, coagulation disorders, anemia, and leukopenia.
2.Sex, age, side of surgery, height, body mass index (BMI), ARCO stage, and follow-up duration were not matched with the study group.
Based on these criteria, a total of 80 patients who underwent THR for ONFH between 2011 and 2022 were included in this study: 40 patients treated before August 2019 formed the control group, while 40 patients comprised the study group. Preoperative data collected included gender, age, vital signs, blood tests, liver and kidney function, BMI, and comorbidities (e.g., tuberculosis, syphilis, hepatitis B, hepatitis C, cardiopulmonary diseases). Imaging assessments (X-ray, CT, MRI) were performed, and ARCO staging was documented.
Perioperative treatment measures were meticulously recorded for both groups, including antiviral regimen and duration, as well as CD4+ and CD8+ T cell counts, CD4+/CD8+ ratios, and viral load. Nutritional status and immunization data were also collected. The ERAS group received standardized treatment measures preoperatively, during the procedure, immediately postoperatively, and one week after surgery. Key metrics such as operation time, blood loss, transfusion volume, postoperative changes in relevant indices, activities of daily living (ADL), and Harris hip scores were documented. Hospitalization duration, follow-up imaging changes, and early postoperative complications were recorded for both groups, along with the occupational exposure of medical personnel during the perioperative period (Table 1).
Table 1 Comparison of preoperative general information between the two groups of patientsAll surgeries were performed by the same surgical team, with the ERAS protocol implemented by a multidisciplinary team comprising orthopedic surgeons, anesthesiologists, nurses, psychologists, and a dietitian. The psychologist and dietitian focused on mental health and nutritional assessments to optimize patient outcomes, guided by evidence-based practices. The TP program for perioperative care was executed by the same team. A comparative analysis of the two programs is presented in Table 2 [19,20,21,22].
Table 2 Programs of ERAS methods and traditional pathwaysThe discharge criteria for both groups were identical, requiring stable vital signs, good mental status, absence of fever, no contamination of dressings, manageable pain, a tolerable diet, independence in defecation, the ability to walk more than 100 m without rest, and mastery of rehabilitation training (Table 2).
Surgical approach and perioperative managementPreoperative treatment and selection of the HAART programHIV infection can lead to the reactivation of dormant pathogenic microorganisms in the body, impairing immune function and increasing susceptibility to opportunistic infections. To address these common complications, it is recommended that patients with CD4+ T lymphocyte counts below 200 cells/μL or a history of oral candidiasis receive prophylaxis against Pneumocystis carinii pneumonia (PCP) using cotrimoxazole. For patients not receiving prophylaxis, heightened vigilance for PCP is necessary, particularly in cases of postoperative pulmonary complications. For those with CD4+ T lymphocyte counts below 50 cells/μL and a history of Mycobacterium avium complex (MAC) infection, prophylactic treatment with clarithromycin or azithromycin may be considered [18, 23, 24]. Opportunistic infections remain a significant cause of mortality among HIV-positive individuals, and the World Health Organization recommends the early initiation of highly active antiretroviral therapy (HAART) within seven days of diagnosis.
We advocate for the early administration of a highly effective HAART regimen to achieve rapid viral load reduction prior to surgery, with long-term maintenance therapy afterward tailored to the patient's financial situation. The rapid and effective HAART regimen can reduce the patient's viral load to undetectable levels (< 20 copies/mL) within 2–4 weeks, thereby significantly lowering the risk of surgical site infections and other complications, as well as reducing the risk of healthcare workers contracting HIV from post-surgical occupational exposure [25,26,27,28,29]. A comprehensive set of perioperative preventive measures against opportunistic infections can further mitigate infection risk [30].
For patients in the Enhanced Recovery After Surgery (ERAS) group, the HAART regimen was based on a newly recommended single-tablet regimen: BIC/FTC/TAF (Bitovir, Bic Enbrel), along with ABT (Abbavitide for injection), which was initiated immediately following HIV diagnosis without significant adverse effects. In contrast, the Traditional Protocol (TP) group received the classical regimen of TDF + 3TC + EFV, also initiated immediately post-diagnosis, without significant adverse effects. Notably, preoperative immunologic indices in the ERAS group, including CD4+ T lymphocyte and CD8+ T lymphocyte counts, were significantly higher than those in the TP group, while the viral load was lower in the TP group, with statistically significant differences (P < 0.05). This suggests that the HAART regimen in the ERAS group is superior in terms of achieving faster viral reduction and enhancing immunity, thereby reducing the incidence of opportunistic infections and occupational exposure risk for healthcare workers (Table 3).
Table 3 Comparison of preoperative immunity indexes between the two groups of patientsIn addition, the ERAS group should conduct a comprehensive assessment of organ function and nutritional status, selecting immunomodulatory treatments such as thymosin and interferon based on individual patient needs. Appropriate management measures should also be implemented for complications such as hepatitis B, hepatitis C, syphilis, tuberculosis, heart disease, and hypertension, which should be addressed symptomatically. Surgical intervention should only be considered after substantial improvement in the patient's immune function and stabilization of complications, in order to minimize the risk of postoperative complications and mortality. Following these perioperative treatments, the nutritional status of patients in the ERAS group was found to be superior to that of patients in the TP group, who exhibited greater surgical tolerance (Table 4).
Table 4 Comparison of preoperative nutritional indicators between the two groups of patientsPeople living with HIV (PLWH) have a significantly higher incidence of postoperative complications, including infections, due to their compromised immune systems. Therefore, special considerations for perioperative prophylaxis are warranted. For patients with severe surgical trauma, prolonged surgical duration, advanced age, and multiple comorbidities, an extended duration of antimicrobial prophylaxis and increased antimicrobial levels should be considered [19]. For patients at high risk for surgical site infections, the prophylactic use of antimicrobial agents is crucial, particularly when CD4+ T lymphocyte counts are below 200 cells/μL. The appropriate use of sulfamethoxazole and antifungal medications is recommended to prevent PCP and other fungal infections [31]. There were no significant differences in inflammatory markers between the two groups (P > 0.05) (Table 5).
Table 5 Comparison of preoperative inflammatory indicators between the two groups of patientsSurgical approach and intraoperative managementAll patients underwent unilateral THR in separate sessions using the posterior-lateral modified Gibson approach. The femoral head prostheses were made of ceramic materials, with 68 cases sourced from the German LINK company and 12 cases from the domestic Beijing Chunli company. To minimize occupational exposure, the surgical team was equipped with protective clothing resembling space suits, complete with a ventilation device (Stryker Company, USA), as well as protective masks, hats, face shields, two pairs of sterilized gloves (or French anti-virus double-layer gloves), and protective boots. The surgical team is relatively stable and comprises an orthopedic surgeon, an anesthesiologist, a nurse, a psychologist, and a nutritionist. Psychologists and dietitians assist with mental health and nutritional assessments to optimize the patient's condition. A perioperative program was developed based on evidence-based practices and principles of the Rapid Recovery Program (Table 2). The control group followed a traditional perioperative care protocol administered by the same team, aiming to shorten surgery duration while ensuring safety.
Before the surgical procedure commenced, the affected limb was washed with soapy water, wiped with alcohol, and covered with iodophor gauze for 15 min, followed by routine sterilization and drying. After each surgical step, the limb was rinsed with 100 ml of iodophor and saline to ensure complete hemostasis. In cases of acetabular abrasion, the approach depended on the patient's specific circumstances, including extensive femoral head necrosis or significant bone defects. If necessary, cancellous bone from the neck of the femoral head was harvested for grafting, as recommended by the surgeon. Prior to the operation, the surgeon conducted a thorough evaluation and preoperative preparation to ensure the safety and feasibility of the procedure. Postoperative rehabilitation and follow-up are equally important for evaluating surgical efficacy; thus, a larger bone graft of 2–4% of the specimen size was selected.
The acetabular prosthesis was sized 2–4 sizes larger than the trial mold, with screws used for enhanced fixation. For patients with significant osteoporosis, a biomimetic prosthesis or an extended shank was utilized to disperse stress. The operation time, total blood loss, and hospitalization duration in the ERAS group were significantly lower than those in the TP group (Table 6).
Table 6 Comparison of operation time, total blood loss, blood transfusion and hospitalization time between the two groups of patientsPostoperative managementRoutine postoperative monitoring included assessments of CD4+ T cell count, CD8+ T cell count, and viral load (VL). For HIV-positive patients undergoing THR, aseptic technique was crucial, and antibiotics were administered postoperatively to prevent infection, with the duration adjusted based on the surgical incision type and patient condition. Discharge criteria were identical for both groups, including stable vital signs, a satisfactory mental state, absence of fever, dry dressings without exudate, tolerable and reducing pain, a normal diet, no discomfort during ambulation, and proficiency in rehabilitation training. The perioperative period adhered to the ERAS principles, resulting in significantly shorter hospitalization compared to the TP group (Table 6).
Postoperative follow-up and functional evaluationCD4+ T-cell counts, CD8+ T-cell counts, and VL tests were conducted regularly at 1, 3, 6, and 12 months postoperatively, followed by annual assessments. The improvement in patients’ ability to perform daily activities was evaluated using the Activity of Daily Living Scale (ADL) at admission and discharge, with all patients demonstrating significant improvements compared to their admission status (Table 7). The Harris Hip Score (HHS) was assessed during follow-up to evaluate hip function improvement (Fig. 1). Recorded complications included surgical site infection, pneumonia, sepsis, cardiovascular events, mortality, lower extremity venous thrombosis, pulmonary embolism, urinary tract infection, cerebrovascular accidents, pressure ulcers, bowel obstruction, and shock. Additionally, perioperative occupational exposure among medical personnel was monitored to compare surgical complication incidence rates between the two groups. Orthopantomograms and frog-leg position X-ray examinations were repeated at each follow-up visit for imaging evaluation.
Table 7 Comparison of ADL scores of patients entering and leaving the hospital in the two groupsFig. 1
Trends in Harris scores (blue: ERAS group red: TP group)
Statistical analysisStatistical analyses were conducted using SPSS 26.0 software. Qualitative data were expressed as case numbers, while continuous variables were presented as mean ± standard deviation (Mean ± SD). Comparisons between groups were performed using independent samples t-tests. For the evaluation of the same indices across three or more time points during the follow-up period, repeated-measures analysis of variance (ANOVA) was utilized. Categorical data were expressed as frequencies, with group comparisons analyzed using the chi-square test or Fisher’s exact probability method. Differences were deemed statistically significant at P < 0.05.
留言 (0)