
記住我









During the study period the HSAR bases completed 18,710 missions. A total of 10,400 (56%) were categorized as primary HEMS missions, 6531 (35%) as HSAR missions, and 1699 (9%) as secondary HEMS missions/interhospital transfers. Eighty missions (0.4%) lacked mission categorization (Fig. 2).
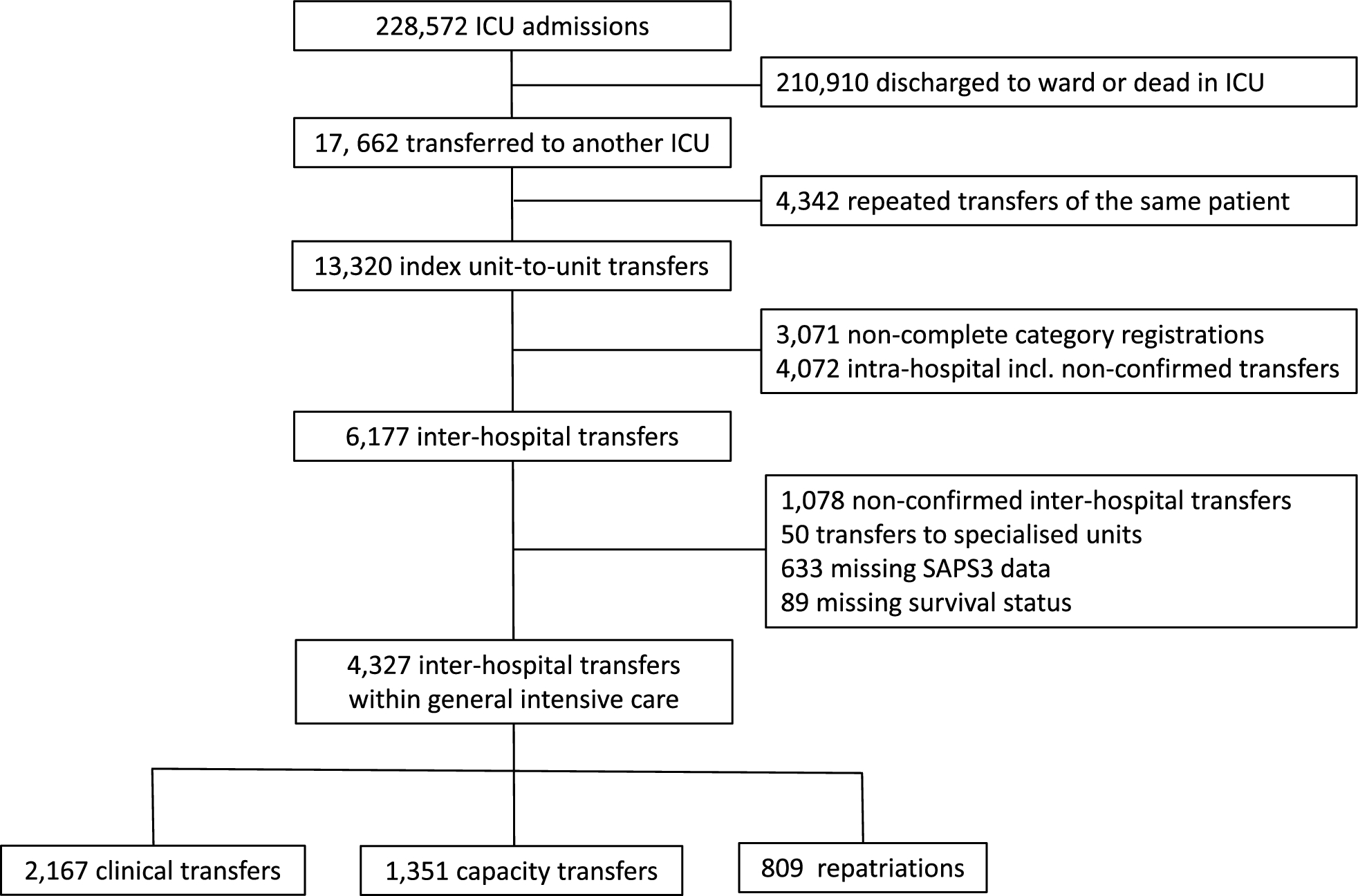
Fig. 2
Study diagram for all helicopter missions 2011—April 2024. Of the HHOs, 2,423 mission resulted in HEC. The diagram illustrates from which environment the patients were hoisted: Terrestrial = Land/mountain/forest, Maritime = Boats and ships, Water = Direct extrication from ocean/lake/river. Of the terrestrial and maritime HEC, 1261 patients were hoisted horizontally in a helicopter rescue bag (RB) or stretcher
Patient characteristics and medical interventions in all missionsThe HSAR crew attended to 16,384 patients of whom 10,171 (62%) were male. Acute medical events were the main cause for dispatch in 8761 missions (54%), followed by 5474 traumatic causes (33%). The median NACA-score was 4 (range 0–7). CPR was performed on 1128 patients (7%), of whom a mechanical chest compression device (mCPR) was used in 430 patients (3%).
The most common intervention was oxygen (n = 6327, 39%), followed by crystalloid infusion (n = 4826, 30%) and analgesia (n = 3345, 20%). Advanced medical interventions included endotracheal intubation (n = 1818, 11%), total intravenous anaesthesia (n = 1248, 8%), automatic ventilation (n = 1106, 7%), invasive arterial blood pressure (IABP, n = 961, 6%) and blood product transfusion (n = 278, 2%).
An overview of patient characteristics and interventions is presented in Table 1.
Table 1 Patient characteristics and medical interventions for all helicopter missions 2011—April 2024 (n = 16,384)Mission characteristics of HHOs with HECHHOs were performed in 3284 (50%) of the missions categorized as HSAR. While the RS was hoisted down in all HHOs, the physician was hoisted down in 1295 (39%). 2423 HHOs (74%) resulted in HEC. Of the HEC patients, 1261 (52%) were hoisted horizontally in a rescue bag or stretcher of which a total of 54 patients (2%) were identified as iHEC (Fig. 2). Among the iHEC missions, 27 (50%) occurred during the summer months (June–August), and 9 (17%) occurred during winter months (December-March). Fourteen missions (26%) were classified as night operations requiring night vision goggles. Thirty-seven patients (69%) were located on land or on a waterfront, and 17 (31%) were located on ships or boats. Twenty-two cases (41%) were categorized as sports related. An overview of mission characteristics is presented in Table 2.
Table 2 Mission characteristics of HHOs with iHEC 2011—April 2024 (n = 54)We observed an increasing frequency of iHEC missions during the study period. While 19 cases occurred during the first half of the study period, 35 cases occurred during the last half. In 2023, 11 cases of HHOs with iHEC were executed (Fig. 3).
Fig. 3
Incidence with trendlines for HHOs with HEC and iHEC in the RNoAF 330 Sqn 2011–2023
Patient characteristics and medical interventions in HHOs with iHECThe median patient age was 50 years (range 17–85), and 44 patients (81%) were male. Traumatic causes (including secondary asphyxia, i.e., avalanche and drowning) were the reason for intubation in 32 patients (59%), whereas 22 intubations (41%) were performed due to acute medical conditions. The median NACA score was 6 (range 5–7) and the median Glasgow coma scale (GCS) score prior to intubation was 3 (range 3–15).
Twenty-four iHEC patients (44%) were intubated before arrival of the RRT by either another HEMS physician or a ship doctor. Drug-assisted rapid sequence intubation (RSI) was performed in 31 patients (57%). Other advanced medical interventions on-scene included thoracostomy (n = 4, 7%), vasoactive drug infusion (n = 3, 6%) and blood product transfusion (n = 2, 4%). CPR was performed on 25 patients (46%), of whom 10 (40%) obtained ROSC before hoisting. Of the 15 patients with persistent cardiac arrest, 13 patients (87%) were hoisted with an ongoing mechanical chest compression device (mCPR). Two patients in cardiac arrest had a period of no-flow during the hoist procedure. Eleven cardiac arrest cases (44%) were presumed to be of primary coronary origin. Although it was registered in a few patients, the occurrence of hypothermic cardiac arrest (or core temperature) was not consistently documented in the written reports. The median on-scene time for the RRT was 23 min (range 1–74).
During hoisting, 34 patients (63%) were ventilated manually with a self-inflating bag, whereas 20 (37%) were connected to an automatic ventilator. While one base only practiced manual ventilations, another base used an automatic ventilator in 83% of the cases. The most frequently used ventilator was a compact battery powered turbine ventilator.
Monitoring of vital parameters during hoisting varied from none (n = 4, 7%), to fully monitored patients with peripheral oxygen saturation (SpO2), electrocardiogram (ECG, capnography and IABP (n = 2, 4%). Thirty-nine patients (72%) were documented to having ≥ 1 vital signs (capnography or SpO2) monitored during hoisting and 25 (46%) had ≥ 2 vital signs monitored. The database registries were nondescriptive for 10 cases (19%).
Table 3 presents an overview of patient characteristics and interventions in HHOs with iHEC.
Table 3 Patient characteristics and medical interventions in HHOs with iHEC 2011—April 2024 (n = 54). Only interventions that could be verified to be delivered on-scene are includedAdverse events in HHOs with iHECFour adverse events related to the hoist procedures were identified. In two of the cases, stretcher rotation resulted in periods of suboptimal manual ventilation. In the third case, the helicopter downwash resulted in disconnection between the manual ventilation bag and the endotracheal tube. The physician was here unable to reconnect the bag before entering the helicopter cabin, at which point the SpO2 had decreased to approximately 80%. In the fourth case, a brief disconnection between the filter and tube occurred during the loading of an iHEC patient into the helicopter cabin. None of these events were deemed by the physician to affect patient outcome.
Patient outcome in HHOs with iHECTwenty-eight patients (52%) survived to hospital discharge. Among the survivors, seven (25%) presented with initial cardiac arrest, of whom six obtained return of spontaneous circulation (ROSC) before hoisting. The last cardiac arrest survivor received continuous mCPR to an extracorporeal life support (ECLS) centre. Twenty-four iHEC patients (44%) did not survive to hospital discharge, and the outcome was unknown for two patients (4%).
留言 (0)