WHO/INRUD prescribing indicators
In the present study, a total of 600 prescriptions representing 600 patients were assessed in outpatient setting. This study showed the existing prescribing practices of the study hospital compared to WHO/INRUD prescribing indicators. The five prescribing indicators namely: average number of medicines per encounter, percentage of medicines prescribed by generic name, percentage of encounters with antibiotics, percentage of encounters with injection and percentage of medicines prescribed from EML were evaluated against the WHO optimal values.
The results of this study revealed that a total of 1088 medicines were prescribed, giving an average number of 1.8 (SD: ±0.83) medicines per prescription. This is within the upper limit of the WHO optimal value (1.6–1.8), which is encouraged. But, this might not be the case. A study conducted on the impact of war on the health system of Tigrai, Ethiopia, showed that only 27.5% of the hospitals and 17.5% of health centers were functional six months after the onset of Tigrai war [29]. So, low medicines supply chain attributed to the long-lasting effet of war crisis in the study area might have influenced prescribing practice of the clinicians in the hospital. First, clinicians may not prescribe for the medicines unavailable in their hospital. Second, clinicians may hesitate to prescribe drugs for fear of unaffordability of the patients, particularly for the drugs to be obtained from private pharmacies. Our finding on average number of medicines per encounter is comparable to the study finding from Eritrea [30] and slightly higher compared to the study elsewhere from Ethiopia [23] where it was 1.76 and 1.69, respectively. But, studies done in eastern Ethiopia [3], Pakistan [12], Saudi Arabia [2] and Sri Lanka [4] reported higher average number of medicines per prescription than ours, which varied from 2.17 to 3.1. As polypharmacy is a main risk factor for drug interactions [31, 32] and adverse drug reactions [33], prescribers are encouraged to restrict the number of medicines they prescribe as few as possible.
WHO recommends that all medicines should be prescribed by generic name, as generic name is much simpler and cheaper than medicines prescribed with brand names [21]. Besides, generic name prescribing promotes better communication among health care providers, which is good for the safety of the patients [2]. In this study, the percentage of drugs prescribed by generic name was 91.5%, a value below the WHO standard value of 100%. This result is very similar to a systematic review done in Ethiopia, which was 91.6% [34]. But, higher generic prescribing was reported from studies in Jordan (100.0%) [7] and north Ethiopia (97.5%) [23] while lower levels were reported from studies in Pakistan (56.6%) [9] and Sri Lanka (35.5%) [4].
In this study, only 43 (7.2%) prescription encounters included injectable medicine (s), a value much lower than the WHO standard (13.4–24.1%). The finding was also lower compared to studies from various parts of Ethiopia including 13.5% in Dire Dawa [35], 15.9% in Mekelle [23], 26.5% in eastern Ethiopia [3] and 44.77% in Dire Dawa [36]. The current study was conducted in outpatient setting where injections are reasonably expected to be low. This may be one possible reason for low prescribing rate of injection in this study. Inpatient pharmacy of Adigrat general hospital had been either partially or totally out of service for the last three years due to the war crisis in Tigari, making it difficult to retrieve prescription information. Overuse of injectable medicine may lead to a higher probability of transmission of hepatitis, human immunodeficiency virus/acquired immunodeficiency syndrome (HIV/AIDS) and other blood borne diseases [5].
Regarding essential medicine prescription, the percentage of medicines prescribed from the Ethiopian EML was relatively frequent (98.7%). Although this value did not meet the WHO optimal value (100%), it is higher than the WHO African regional value of 89.0% [22]. Similar findings to our result were reported as 98.8% in Pakistan [9] and 99.2% in Dire Dawa, Ethiopia [35]. In contrast to our finding, some previous studies carried out in Jordan [7], Sri Lanka [4] and Ghana [28] showed lower values (54.1 – 88.1%). Prescribing medicines from the EML is a crucial step to provide safe, efficacious and cost effective medicines to the individual patient and to the community at large [1, 21]. In resource limited health facilities like in our study area, prescribing medicines from the EML is particularly important for the patients as far as the cost of medicines is concerned. The relatively high practice of prescribing medicines from EML observed in this study is, therefore, quite promising, which needs further encouragement.
In this study, a total of 340 antibiotics were prescribed. The percentage of prescriptions with least one antibiotic prescribed was 44.5%. This is almost twice the average WHO standard value of 20–26.2%. The current finding is also higher than the result of studies done in different parts of Ethiopia, which was 24.85% in southwest Ethiopia [37], 27.62% in Dire Dawa [36], 32.05% in Mizan-Tepi [38], 32% in north Ethiopia [39] and 37.5% in Gondar [40]. But, our finding is close to previous findings reported from Dire Dawa [35] and from systematic review of 11 African countries [22], where percentage of prescriptions with antibiotics were 47.8% and 46.8%, respectively. On the other hand, inconsistent with our result, higher percentage of encounters with antibiotics were reported from different parts of the world as; 88.0% in Tanzania [41], 52.4% in Pakistan [12], 59.9% in Ghana [28], 58.2% in Mekelle, Ethiopia [23] and 78% in Bangladesh [42].
The discrepancy in the rate of antibiotics prescriptions could be due to potential differences between our study and the contrasted studies in terms of level of vigilance of prescribers, epidemiology of the infectious diseases, the sample size, number of health facilities included, prescribing guidelines and socio-demographics of the study populations. Unlike to our study, some of the aforementioned studies included more than one health facility [23, 28, 37, 41], while the other studies used sample size either < 600 prescription encounters [36, 38, 39, 42] or > 600 prescription encounters [12]. These could contribute for the observed differences in patterns of antibiotics prescription.
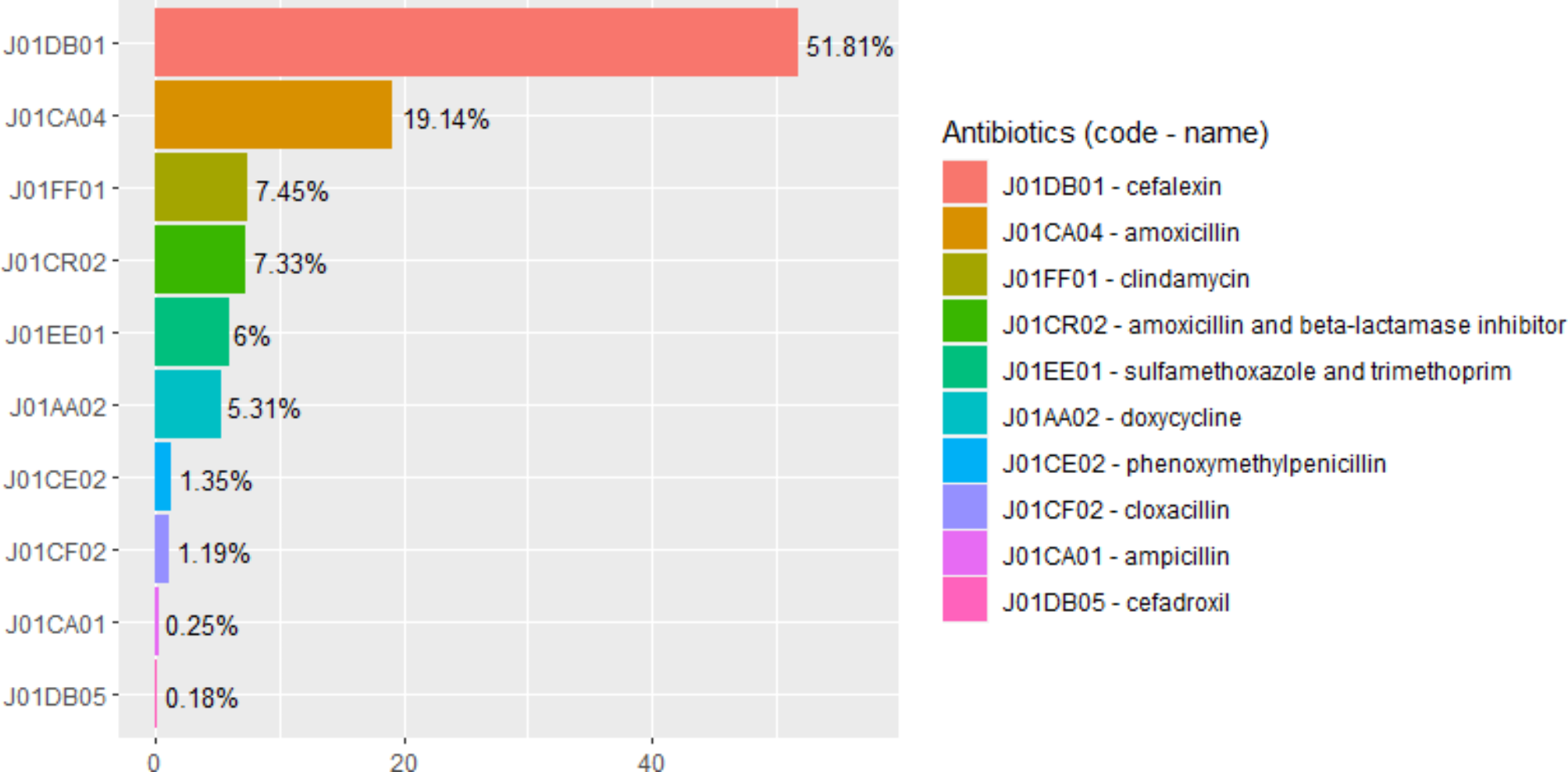
Penicillins (J01C) (34.4%), macrolides (J01F) (23.8%) and fluoroquinolones (J01M) (17.1%) were the most commonly prescribed antibiotics classes in the present study, which combinely covered 75.5% of the total antibiotics prescribed. Moreover, amoxicillin (22.4%), azithromycin (19.4%) and ciprofloxacin (13.8%) were the top three frequently prescribed at single antibiotic level. Consistent with our finding, previous studies from southwest Ethiopia [24], Tanzania [43], Botswana [44] and Addis Ababa [45] reported that penicillins were the first commonly prescribed classes of antibiotics (32.7 − 51.9%). In contrast, previous study found that cephalosporins as a class and ceftriaxone at drug level covered 81.5% and 71.8% of the antibiotic prescriptions, respectively [12]. On the other hand, the most commonly prescribed drug was amoxicillin in both the studies from Botswana (28.4%) [44] and Addis Ababa (44.8%) [45]. This is similar to our finding. Besides, ciprofloxacin (21.1%), amoxicillin (11.8%) and azithromycin (10.6%) were the top three frequently prescribed in previous study [24], which is similar to our finding despite the order of these three drugs.
The current study indicates that almost three-fourth (75.5%) of the antibiotics prescription was covered only by three classes of antibiotics, namely, penicillins, macrolides and fluoroquinolones. Besides, amoxicillin, azithromycin and ciprofloxacin combinely accounted for more than half (55.6%) of the total antibiotic prescriptions. Such excesive use of antibiotics only from few types of antibiotics can worsen the emergence of resistant bacteria against these antibiotics in our setting.
Clinicians’ practice to prescribe antibiotics merely based on assessment of patient’s symptoms is a common cause for over prescription of antibiotics, especially in resource limited countries. This is, in part, due to scarcities of modern diagnostic tests to confirm infectious diseases [14]. Use of antibiotics for self-limiting diseases is also other factor for over prescription of antibiotics [11]. The perception of both health professionals and the public as antibiotics are powerful medicines may also contribute to the over-prescription of antibiotics [28].
But in context of our study, the high rate of antibiotics prescription may also indicate the high burden of infectious diseases in Tigrai, Ethiopia. So, the results should be interpreted carefully. Neverthless, indiscriminate use of antibiotics is a key driver for the emergence of AMR, which obligates us to sake new drugs. Unfortunately, a truly new class of antibiotics has not been discovered in the last decades, and there are still commercial challenges to develop new antibiotics [11, 46]. The excessive use of antibiotics may aggravate the rapidly emerging AMR in Ethiopia [47], including in Tigrai region of Ethiopia [48]. So, the prescribers herein the study area should adhere antibiotics guidelines and be vigilant that antibiotic prescriptions should be supported by up-to-date surveillance.
“AWaRe” classification of antibiotics
In the current study, the “Access” group covered 54.4% of the antibiotics, whereas the “Watch” group accounted for the rest 45.6% of the total antibiotics prescription as per the “AWaRe” classification. No antibiotic was prescribed from the “Reserve” group. This result is close to a study done in eastern Ethiopia which found that 55.3% and 43.1% of the antibiotics were from the “Access” and Watch” groups, respectively [35]. Higher proportion of antibiotics in the “Access” group was reported in some African countries (73.9 – 90%) [44, 45, 49, 50], which is inconsistent with our finding. However, no antibiotic was in the “Reserve” group in all these studies, which is similar to the current study. The use of antibiotics in the “Watch” category was 50.69% in a study from southwest Ethiopia [24], which is higher than our result.
The “Access” antibiotics have narrow spectrum of activity with lower potential for antimicrobial resistance. Whenever appropriate, antibiotics in the “Access” group should be preferred over “Watch” groups concerning the spread of antibiotic resistance [51, 52]. The “Watch” group antibiotics, on the other hand, have higher resistance potential and hence, they should be prioritized as key targets of antibiotics stewardship programmes and monitoring to prevent their overuse [16]. The use of “Watch” antibiotics should be discouraged unless clearly clinically required [18]. Hence, the WHO recommends that at least 60% of all antibiotics use should be from the “Access” group to contain trising AMR and make antibiotic use more effective [11, 52].
The current study showed that the use of “Watch” group antibiotics in the study hospital was relatively high. This may be an alarm for clinicians to focus on the evidence based use of these very crucial antibiotics found in the “Watch” group. Besides, ciprofloxacin and azithromycin accounted for 33.5% and 42.6% of total antibiotics in the “Watch” group, respectively. This may indicate that the appropriate use these drugs should be closely monitored in the outpatient setting of the hospital.
Predictors of antibiotic prescribing
Our analysis using multivariate logistic regression showed that age of patients was significantly associated with antibiotics prescribing (P < 0.001). In individuals under 18 years old, the odds ratio of antibiotics prescribing increased by almost 10 times compared to those \(\:\ge\:\) 65 years old. This is in line with the studies from Addis Ababa [45], Dire Dawa, Ethiopia [35], Eritrea [30] and Ghana [28]. In these studies, antibiotics prescribing pattern decreased significantly with increase in patient’s age, which is consistent with our finding. The high level of antibiotics prescribing in this age group (in our study) could be partly due to the high burden of lower respiratory tract infection in the pediatric patients in Ethiopia [53]. This is further supported by our finding that this disease showed significant association with antibiotics prescribing. But, unlike to our result, patient’s age did not show statistically significant association with antibiotics prescribing in previous studies [41, 54]. Apart from the risk of AMR, children are more vulnerable for adverse drug reactions than adult patients due to that they can react differently to drugs than adult populations attributed to pharmacokinetics differences [55]. So, the clinicians in our study area should remain vigilant especially when prescribing antibiotics to the pediatrics age group.
In previous similar studies, gender was significantly associated with antibiotics prescribing [41, 50], which is inconsistent with our study. The current study showed that prescribing two medicines per prescription had significant association with antibiotics prescribing. Accordingly, the odds ratio of prescribing antibiotics was increased by almost 3 times in subjects with two medicines prescribed compared to those having only one medicine. This is similar to previous studies done in Eritrea [30] and elsewhere in Ethiopia [35] where the odds of antibiotics prescribing was significantly inceased as the number of medicines per prescription increased.
In the present study, being diagnosed with diseases of the respiratory system (J00–J99) increased the odds of prescribing antibiotics by almost 3.8-fold (AOR: 3.75, CI: 2.136–6.584) compared when there was no diagnosis of this disease. In previous study, individuals diagnosed with respiratory tract infection had increased odds of antibiotics prescribing by about 7.3 (AOR: 7.27, CI: 1.86, 11.99) compared to those with no diagnosis of respiratory tract infection, which is in line with the finding of the present study. In the current study, lower respiratory tract infection (pneumonia) was the most prevalent disease for which antibiotics were prescribed. This could be attributable to the high level of antibiotics prescribing for diseases of the respiratory system. But, inappropriate use of antibiotics to treat self-limiting upper respiratory tract infections like otitis media could be other reason, as our analysis was done to determine the association between antibiotics prescribing and diseases of the respiratory system in general [11].
On the other hand, some of the ICD-10 diseases were protective against antibiotics prescribing in our study. Subjects with no diagnosis of endocrine, nutritional and metabolic diseases were about 16 times more likely to receive antibiotics. There was also increased odds of prescribing antibiotics with the absence of diseases of the nervous system (AOR: 16.693, CI: 3.461–80.522), mental and behavioral disorders (AOR: 14.124, CI: 2.710 − 73.610) and diseases of the circulatory system (AOR: 8.681, CI: 3.094–24.362).







留言 (0)