Proper hand-washing practice at critical times is are components of personal hygiene that helps prevent diseases, save lives, promote good health, and contribute to a country’s social and economic growth [1, 2].
According to the Center for Disease Control, the critical times for proper hand washing are: after toilet, after changing diapers, after caring for a sick person, after handling raw meat, fish or poultry, and after handling waste [3]. Public health guidelines recommend handwashing with water and soap before cooking food, before feeding a child, before eating food, after defecation, and after cleaning a child who has defecated [4, 5].
Diarrhoea and pneumonia are the leading causes of death among children below 5 years old due to inadequate sanitation and hygiene, resulting in approximately 1.8 million deaths worldwide annually [6]. In Ethiopia, more than 70,000 children die each year due to diarrheal diseases [7].
Worldwide, the mortality rates of under-five aged children remain high. In 2013, 6.3 million children were documented to have died before the age of five. Of these, 51.8% (3.26 million) died due to infectious causes. If current trends continue, 4.4 million children under the age of five are expected to die by 2030. Furthermore, Sub-Sahara African countries will have 33% of births and 60% of deaths [8].
Mothers and other children caretakers engage in various activities such as washing their children’s bottoms, maintaining a clean home and yard, interacting with domestic animals, and visiting restrooms where their hands come into contact with microorganisms. The adherence of mothers to proper hand-washing practice can reduce the incidence of pneumonia and diarrhea among children under-five years old [9].
A recent study has shown that proper hand washing at critical times can significantly reduce bacterial infections and new confirmed cases of COVID-19 [10].
The Sustainable Development Goals aim to ensure healthy lives for all children and decrease the number of deaths among under-five children by 10 million between 2017 and 2030. This can be achieved by improving good hand-washing practice at critical times, as the hands play a central part in our daily activities. The uses of contaminated hands during cooking and eating increases the transmission of microbes that can cause illness [11].
According to the 2019 joint WHO-UNICEF report, hand hygiene is often neglected at critical times due to the lack of access to hand washing facilities in key areas [12]. Recent report showed that an estimated 40% of the world’s population lack basic handwashing facilities at home. Over 50% of the population in sub-Saharan Africa and Oceania do not have access to a facilities equipped with water and soap [12].
Proper hand-washing is rarely practiced in low-income countries such as Ethiopia. Previous research findings suggested that proper hand-washing at critical times such as after defecation or cleaning an infant’s perineum is not a common practice[13].
The proportion of proper hand-washing practice at critical times among mothers of children under-five age was different across countries around the world. It was 76% India [9], 41.6% in Nigeria [14], 21% in Indonesia [15], 67% in Bangladesh [16], in Uganda ranges from 28.5% to 71.4% [17] and 65% in Kenya [18].
Evidence showed that different factors affect the practice of good handwashing practice at critical times among mothers of children under-five years of age. Educational status, knowledge, attitude, availability of water and family size greater than five were significantly associated with good handwashing practice at critical times [19,20,21,22].
A research studies conducted in Ethiopia examining good handwashing practice at critical times among mothers of children under-five reported inconsistent results, ranged from 19.8% [23] to 74.4% [24]. Hence, this review and meta-analysis aimed to estimate the pooled proportion of good hand-washing practice at critical times and its associated factors in Ethiopia. The result of this study will provide evidence for policymakers and for program evaluators.
Methods
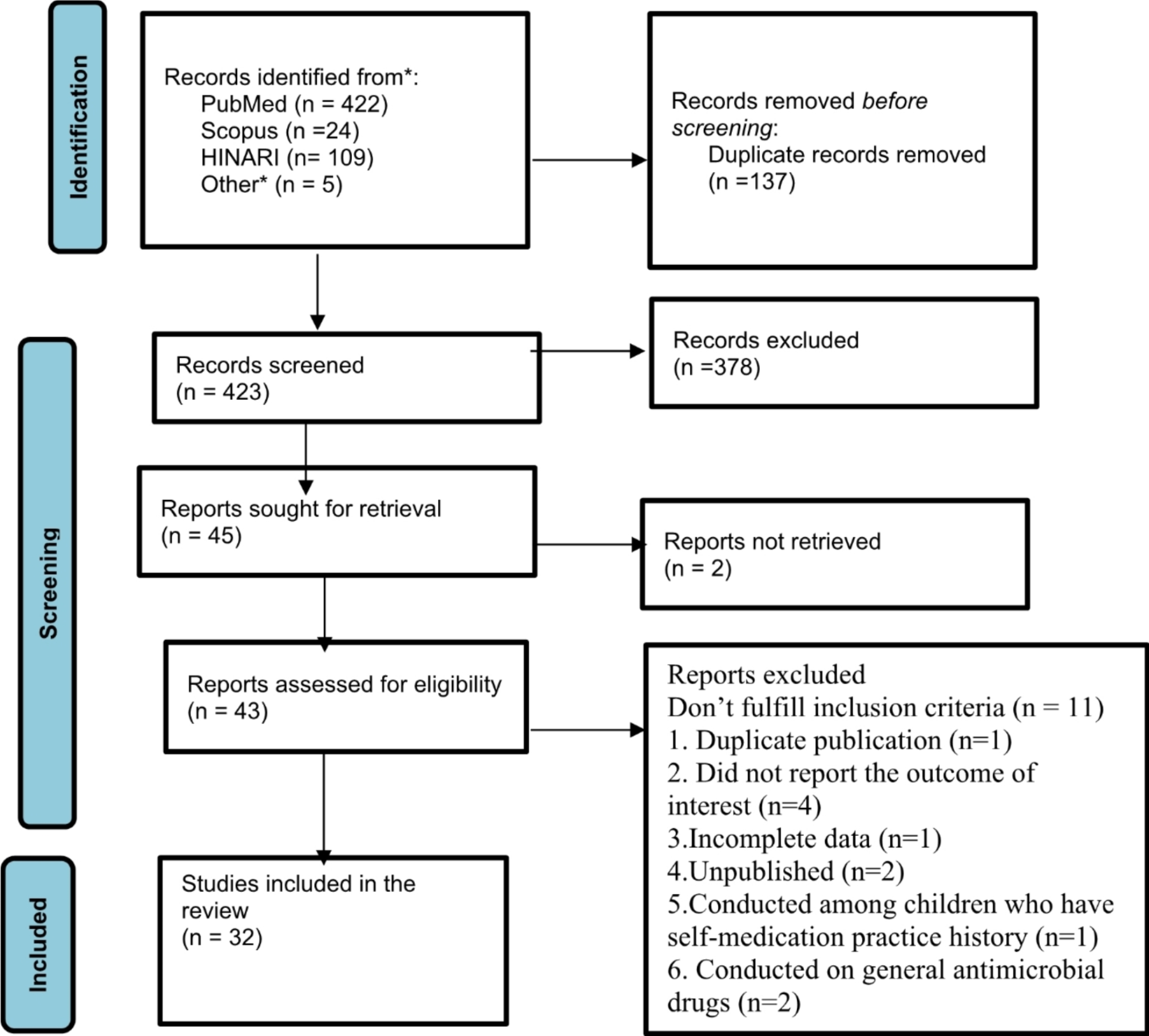
This systematic review and meta-analysis was performed according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 guidelines [25].
Search strategies
A comprehensive search of relevant studies published in English language was undertaken in various databases such as PubMed, DOJA, Embase, Science Direct, Cochrane Library, African Journals online, Google scholar, and Web of Science). Initially,studies were comprehensively searched using the full title (“The proportion and associated factors of hand-washing practice at critical times among mothers of children under-five in Ethiopia”) and keywords (“magnitude,” “proportion,” “hand-washing practice at critical times,” hand-cleaning”, “hand-hygiene”, “determinant factors,” “associated factors,” “predictors,” “in Ethiopia”). Boolean operators “OR” or “AND” were used in combination or independently to connect these keywords and to establish the search terms. Additionally, thereference lists of all included studies were to identify other missed publications.
Eligibility criteria
To determine the inclusion and exclusion criteria for this systematic review and meta-analysis, population, intervention, comparison, and outcomes technique was employed, which involved the uses of condition, context, and population questions for prevalence studies [26].
Inclusion criteria
Study area: studies conducted in Ethiopia.
Population: Low-risk mothers of children below 5 years old
Study setting: Studies conducted in health care facilities or community-based settings.
Study design: All observational studies (cross-sectional, cohort, and case–control studies that reported either the proportion or magnitudes and associated factors or predictors of handwashing practice at critical times.
Exclusion criteria
Qualitative studies that didn’t provide quantitative evidence and those that used different operational definitions and measurements of good hand-washing practice at critical times were excluded from this review and meta-analysis.
Data extraction
Data from the selected studies were separately extracted using a predesigned data extraction form in Microsoft Excel version 2016. The spreadsheet included the first author’s name, year of the data collection conducted, year of publication, study design, study area, study setup, sample size, and the proportion good practice of hand-washing at critical times. Any discrepancies between the data extractors were resolved through discussion and re-evaluation of the studies.
Quality assessment
The Joanna Briggs Institute (JBI) Critical appraisal checklist was used to evaluate the methodological quality of the included studies [27]. There are nine parameters in the tool. The two authors separately ranked the quality of the included studies.
Each item was evaluated as low, moderate or high risk of bias. A composite quality index was categorized and the risk of bias was ranked as low (0–2), moderate (3 or 4), or high (≥ 5).
Outcomes
This study had two outcomes (proportion and associated factors of good hand-washing practice at critical times among mothers of children under-five in Ethiopia. Based on the operational definition of the included studies; good hand-washing practice at critical times was considered when the respondents who scored above the mean of the practice related questions.
Data management and statistical analysis
Data were extracted using a Microsoft Excel spreadsheet and analysed using the Stata 17 statistical software. The Higgins \(^\) statistic and Cochran’s Q-test were used to examine the presence of statistical heterogeneity among the included studies. A random-effects model using the DerSimonian-Laird method was used to estimate the pooled prevalence of proper handwashing practices at critical times. The adjusted odds ratios (AORs) and 95% confidence intervals (CIs) were extracted from the included studies. A random- or fixed-effects model was used to calculate the pooled AORs. Lastly, the pooled estimates for proper handwashing practices at critical times and the associated factors, as well as their corresponding 95% CIs, were presented in forest plots.
Subgroup analyses and heterogeneity
To identify the potential sources of heterogeneity among the included studies, subgroup analyses were conducted based on the sampling method, geographic region, and year of the study.
Publication bias
Publication bias was visually examined using funnel plots and statistical methods, including Egger’s and Begg’s tests.
Sensitivity analysis
To assess the impact of individual studies on the overall prevalence of proper handwashing practices at critical times, a sensitivity analysis was performed using a random-effects model.





留言 (0)