
記住我
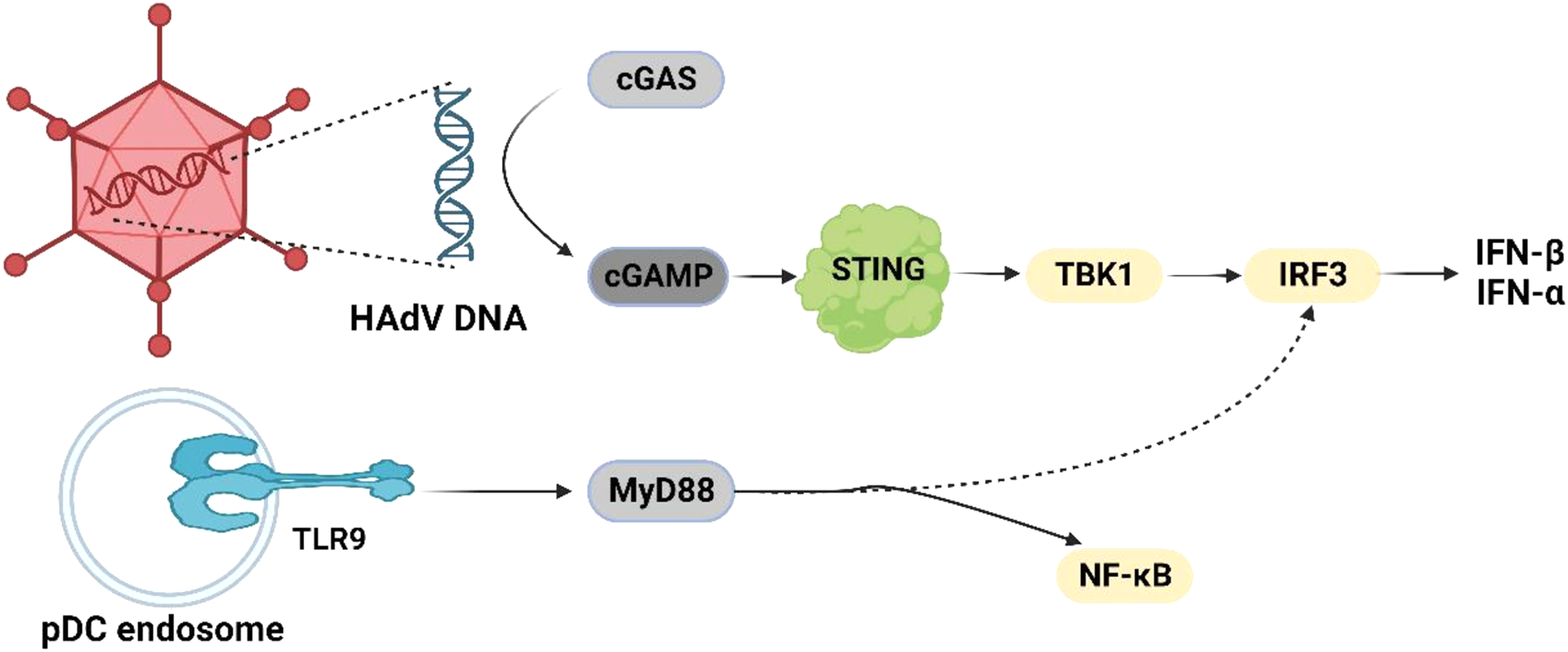




During the study period, 287 preterm infants with gestational age < 34 weeks were admitted to the NICU and treated with caffeine within 24 h after birth, among whom 66 did not meet the inclusion criteria (Fig. 1). Consequently, this study included 221 preterm infants with gestational ages ranging from 24 to 34 weeks and a median gestational age of 32.1 (30.29, 33.29) weeks. The birth weight of the preterm infants ranged from 650 g to 2570 g, with a median birth weight of 1650 g (1314–1920 g). Among them, 123 (55.7%) infants were male (Table 1).
Fig. 1
Flow diagram for preterm infants selection. AOP: apnea of prematurity
Table 1 Comparison of baseline characteristics between the response group and non- response groupThere were 61 preterm infants in the non-response group and 160 preterm infants in the response group. There was no statistically significant difference in maternal age, diabetes, hypertension or preeclampsia, chorioamnionitis, or premature rupture of membranes (> 18 h) between the two groups (P > 0.05). However, gestational age, birth weight and the 5-min Apgar score of the preterm infants were significantly lower in the non-response group than in the response group (P ≤ 0.001). In addition, the incidence of PDA and NRDS was significantly higher in the non-response group than in the response group (P < 0.001 and P = 0.006, respectively). There was no statistically significant difference in sex, mode of delivery, use of antenatal steroids, and SGA between the two groups (P > 0.05; Table 1).
Treatment and clinical outcomesNotably, the 221 preterm infants had a total oxygen supplementation time of 19 days (10.56–38.61 days) and underwent NIV for 13.43 days (6.43–29.43 days). In addition, 18.1% (40) of the preterm infants underwent IMV for a duration of 2.9 days (1.45–5.66 days). The time of invasive high-frequency mechanical ventilation was 2.0 days (0.1–3.6 days), and the rate of re-intubation after extubation was 2.3% (5). The mean maintenance dose of caffeine citrate was 5.13 mg/kg/day (5–5.46 mg/kg/day), and the median duration of caffeine citrate use was 15.5 days (9–28 days). The incidence rates of BPD (mild, moderate, and severe), NEC, ROP, and brain injury were 35.7% (79), 2.3% (5), 41.2% (91), and 14.9% (33), respectively. The mortality rate was 0.5% (1). The length of hospital stay was 30 days (21–47 days).
At initial admission, the non-response group had 9 preterm infants who did not undergo oxygen therapy, 39 underwent NIV, and 13 IMV. There were 20 premature infants who had escalated oxygen therapy due to AOP, including 5 who were transitioned from NIV to IMV. The response group had 20 preterm infants who did not undergo oxygen therapy, 118 underwent NIV, and 22 underwent IMV. There was no significant difference between the groups of admission without oxygen therapy, NIV, and IMV (P > 0.05).
Preterm infants in the non-response group had a longer total supplementation time (P < 0.001), longer NIV time (P < 0.001), longer IMV time (P = 0.039), higher rate of IMV (P < 0.01), and higher rate of re-intubation after extubation (P = 0.032). Preterm infants in the non-response group also had a higher average maintenance dose and longer duration of caffeine citrate use (P < 0.001). The incidence of BPD (P < 0.001), mild BPD (P < 0.001), moderate and severe BPD (P < 0.001), ROP (P < 0.001), and brain injury (P = 0.039) was higher in the non-response group, whereas the incidence of NEC and death did not significantly differ between the groups (P > 0.05). The length of hospital stay was also longer in the non-response group (P < 0.001; Table 2).
Table 2 Comparison of treatment information and complications between the response group and non-response groupThe association between caffeine citrate response and gene polymorphismsAmong the 22 SNPs, rs6279 and rs2283265 did not conform to the Hardy–Weinberg equilibrium, and rs144999500 did not detect mutations; therefore, these SNPs were excluded from further analysis, and 19 SNPs were finally included.
ADORA1 rs10920573 (PFDR = 0.049, recessive model), ADORA2B rs2015353 (PFDR = 0.049, super-dominant model), ADORA3 rs10776728 (PFDR = 0.049, recessive model), DRD3 rs7625282 (PFDR = 0.049, super-dominant model), and DRD3 rs6280 (PFDR = 0.049, super-dominant model) were found to be associated with caffeine citrate response in preterm infants.
In the univariate logistic regression analysis, the CC genotype of ADORA1 rs10920573 (TT / TC vs. CC: OR, 2.89; 95% CI, 1.30–6.40), TC genotype of ADORA2B rs2015353 (TT / CC vs. TC: OR, 2.56; 95% CI, 1.28–5.12), AG genotype of DRD3 rs7625282 (AA / GG vs. AG: OR, 2.15; 95% CI, 1.17–3.96), and CT genotype of DRD3 rs6280 (CC / TT vs. CT: OR, 2.36; 95% CI, 1.29–4.30) were identified as risk factors for non-response to caffeine citrate in preterm infants. Conversely, the AA genotype of ADORA3 rs10776728 (TT / TA vs. AA: OR, 0.30; 95% CI: 0.11–0.80) was identified as a protective factor for caffeine citrate response in preterm infants (Table 3).
Table 3 Genotype distribution of adenosine and dopamine receptor gene polymorphisms among caffeine citrate response and non-response preterm infantsModel for predicting caffeine citrate responseIn the multiple logistic regression analysis adjusted for genotypes (ADORA1 rs10920573, ADORA2B rs2015353, ADORA3 rs10776728, DRD3 rs7625282, and rs6280), gestational age, birth weight, Apgar score, prenatal hormones, NRDS and PDA, the CC genotype of ADORA1 rs10920573 (aOR, 3.51; 95% CI, 1.34–9.25) and CT genotype of DRD3 rs6280 (aOR, 3.19; 95% CI, 1.53–6.65) were identified as independent risk factors for non-response to caffeine citrate in preterm infants. Conversely, higher gestational age (aOR, 0.63; 95% CI, 0.53–0.75) was identified as an independent protective factor for caffeine citrate response in preterm infants (Table 4).
Table 4 Multivariable logistic regression analysis to identify independent risk and protective factors of non-responseWe developed a nomogram to predict caffeine citrate response in preterm infants on the basis of multivariable logistic regression analyses, including the genotype of ADORA1 rs10920573, the genotype of DRD3 rs6280, and gestational age (Fig. 2). The area under the curve (AUC) of the receiver operating characteristic (ROC) curve was 0.764, and the concordance index was 0.764 (95% CI: 0.687–0.842; Fig. 3a). The calibration curve showed a high level of agreement between the predicted and actual probabilities, and this curve was close to the diagonal line (Fig. 3b). The clinical decision curve showed better net benefit in the predictive model (Fig. 3c).
Fig. 2
Nomogram for the prediction of caffeine citrate non-response in preterm infants
Fig. 3
a: ROC curves. ROC receiver operating characteristic, AUC area under the ROC curve. b: Calibration curve for predicting probability of caffeine citrate non-response in preterm infants. c: Decision curve analysis in prediction of caffeine citrate non-response in preterm infants
留言 (0)