
記住我







The present case involves an 80-year-old female who was clinically diagnosed with ESCC. She had a history of accidental ingestion of caustic soda as a child (at 1 year of age). The patient has no history of alcohol consumption or smoking. In August 2012, the patient visited a clinic with the chief complaint of dysphagia. Esophagogastroduodenoscopy (EGD) revealed esophageal stenosis 20 cm from the incisors, surrounded by a white flattened, elevated lesion. There were no findings suggestive of reflux esophagitis. Consequently, the patient was referred to our hospital for thorough examination and treatment of the esophageal stricture.
During EGD in our department, the stenosis prevented the passage of a normal-sized oral endoscope with a diameter of approximately 1 cm (GIF-260 J, Olympus, Tokyo, Japan) (Fig. 1). Thirteen endoscopic balloon dilations (EBDs) of the stenoses were performed in April 2013. Once the dysphagia had improved, dilation was considered completed, and the patient was monitored. In November 2013, tongue cancer was diagnosed, and pathology results showed epithelial dysplasia carcinoma in situ, which was treated with small-source therapy using Au grains.
Fig. 1
The endoscopic image from 8 years ago of the site where the tumor was localized. The endoscopic image from 8 years ago did not reveal any tall elevated lesion. a Panoramic view of the stenotic area. b A close-up image of the stenotic area reveals a whitish, flat elevation on the oral side of the stenosis
In July 2018, the patient presented with dysphagia again, and EGD was repeated. This revealed a three-quarters circumferential white-toned, elevated lesion at 25–30 cm from the upper incisor dentition, with a flat elevation on the oral side, a taller elevation on the anal side, and narrowing of the lumen in the region (Fig. 2). The whitish ridges did not stain with iodine. Malignancy was considered a differential diagnosis; however, histopathological examination of the biopsy specimen showed that the basal layer of the superficial epithelium exhibited regenerative changes, and the superficial layer was hyperkeratotic with no evidence of malignancy. Three EBDs were performed, which did not alleviate the esophageal stenosis, and it was decided to monitor the patient after consultation.
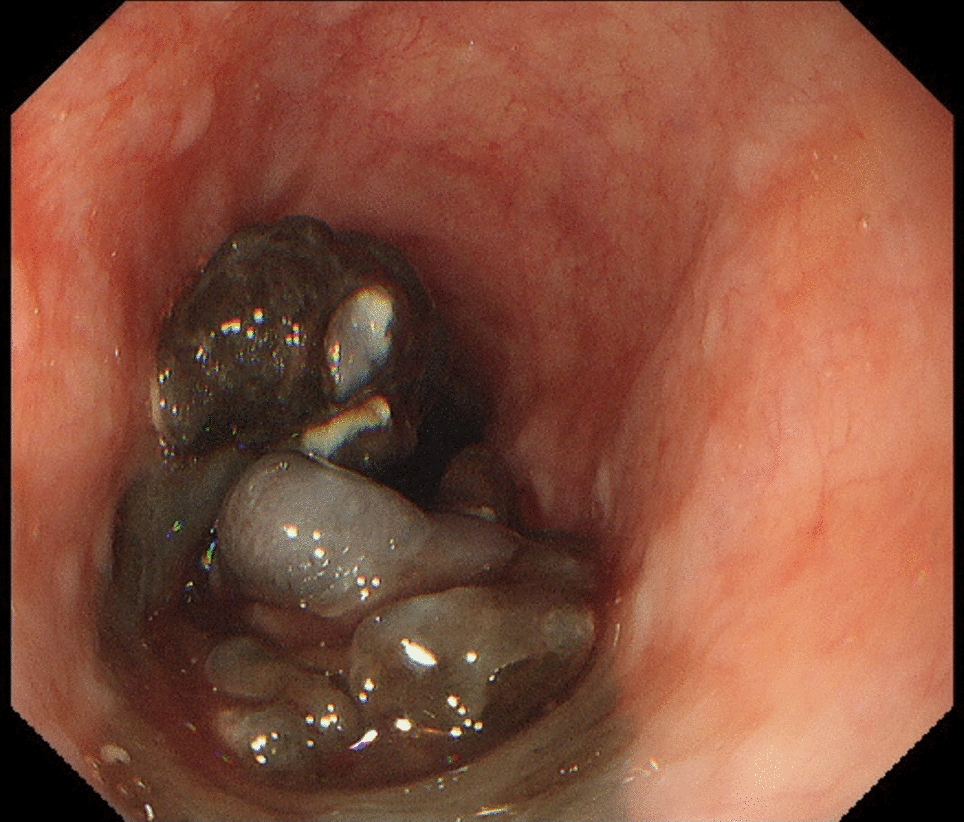
Fig. 2
Endoscopic findings of esophageal stenosis observed 2 years before endoscopic treatment when the patient presented again with dysphagia
In June 2023, during a screening EGD, biopsy tissue from this lesion showed atypical epithelium, and the patient was referred to us again. In the same month, EGD showed a complete circumferential white keratinizing epithelium with thick furrowing at 21–30 cm, a flat elevated white adherence at 25 cm from the incisors, and narrowing from 28 to 30 cm from the incisors, which did not allow passage of a normal-diameter scope (Fig. 3). The scope was changed to a narrow-diameter scope to observe the anorectal side. Histopathology showed that the epithelium was extraordinarily papillary, with hyperkeratosis and calcified degeneration in the superficial layers. The biopsy results showed no evidence of malignancy; however, the lesion was considered the cause of dysphagia; therefore, it was resected en bloc by endoscopic submucosal dissection (ESD) (Fig. 4a–c). After ESD, to prevent esophageal restenosis, 400 mg of triamcinolone was injected into the ulcer base three times: immediately after treatment, on the day after treatment, and 7 days after treatment. In addition, oral prednisolone was administered at 30 mg/day for 1 week, followed by dose reduction by 5 mg each week for 6 weeks. Despite this, dysphagia with a Dysphagia Score of 2 developed in November 2023, and EGD confirmed stenosis. Consequently, to relieve the stenosis, a total of 21 EBD procedures were performed starting in November 2023. Finally, the stenosis was resolved by June 2024.
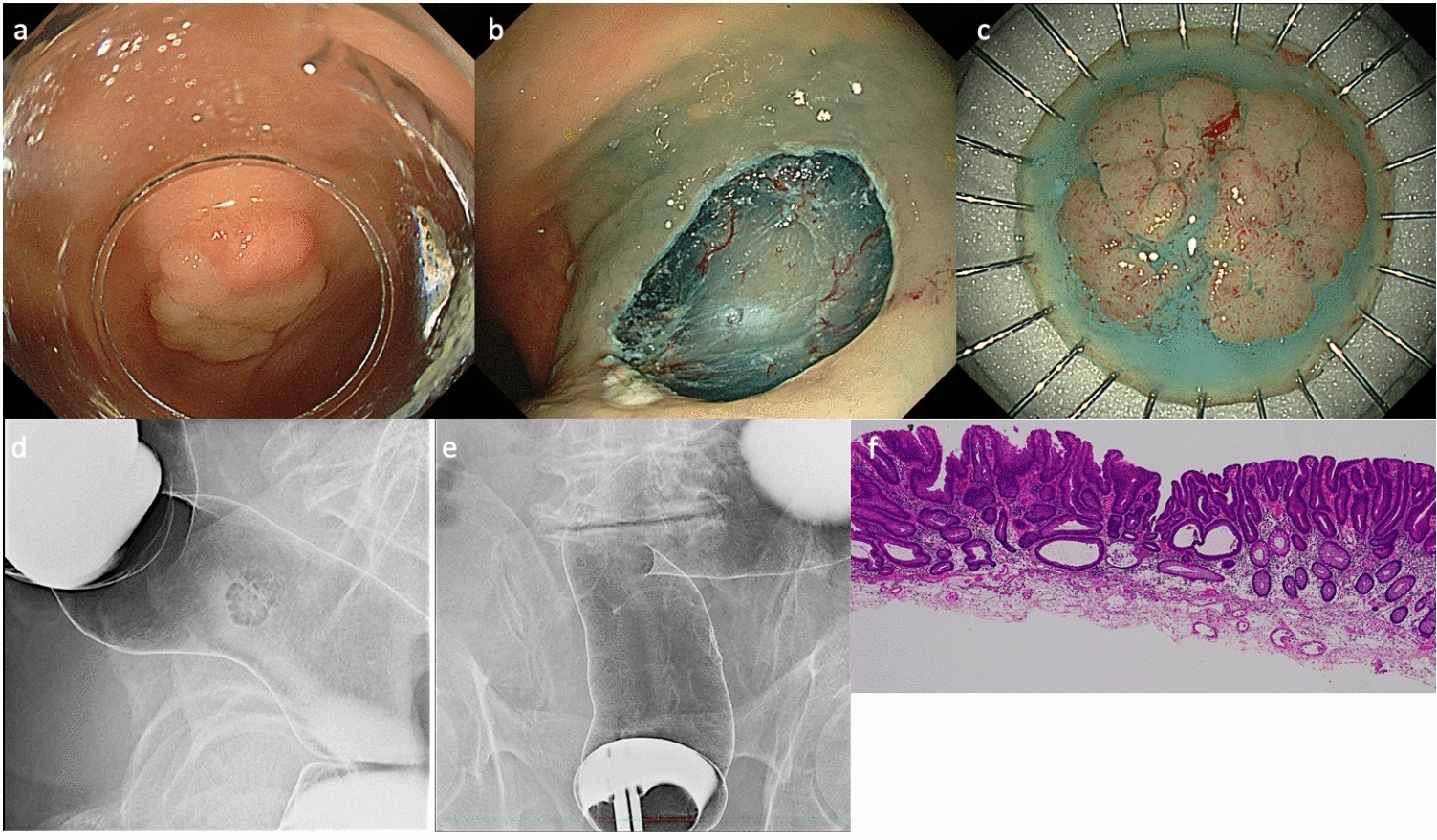
Fig. 3
Endoscopic findings of the lesion at endoscopic submucosal dissection. a Panoramic view of the lesion. b A close-up image of the lesion. In the lesion, a whitish, high-evaluated area and a squamous, flat elevated area are observed. c The high-evaluated area was stenotic. With a thin-diameter endoscope, a fringed keratinized substance is observed on the elevated area. d This lesion exhibits mild to lack of staining with Lugol’s iodine
Fig. 4
Macroscopic and pathological findings of endoscopic submucosal dissection (ESD) specimens. a The tumor was resected in a tubular fashion using ESD. b Gross finding after formalin fixation following ESD. c Iodine-stained findings of the resected specimen by ESD. d Histopathological findings of the elevated area (low magnification view). e At the margin of the elevated area, a distinctly separated thickened keratin layer and granular layer are observed, and these layers are clearly demarcated (low magnification view). f Exophytic and papillary proliferation of low-grade tumor cells within the stratified squamous epithelium is observed. g Immunohistochemical findings for p53: p53-positive staining is observed in a subset of tumor cells
The pathological findings of the ESD specimen showed a circumferential, white-toned, superficial elevated tumor, with a few atypical tumor cells showing exotropia and papillary growth within the stratified squamous epithelium and a thickened stratum corneum and granular layer on the tumor surface, which were distinctly separated from each other. Some of these layers were delaminating (Fig. 4d–f). Immunohistochemistry of this lesion showed positive results for p53, localized to the tumor area of the moderately differentiated component (Fig. 4g). The pathological diagnosis of this lesion was squamous cell carcinoma (pT1a-LPM, Ly0, v0, HM0, VM0) and ESCC with EEM.
We performed cancer multigene panel testing to investigate the etiology of the lesions. Formalin-fixed, paraffin-embedded (FFPE) specimens of the high-elevated area of the ESD specimen of this lesion were dissected into 10 µm-thick tumor tissue sections and mounted on microscopic slides, and DNA was extracted using a QIAamp DNA FFPE Tissue kit (QIAGEN, Valencia, CA, USA) according to the manufacturer’s instructions. DNA from this lesions and blood cells was confirmed to be of sufficient quality and quantity for next-generation sequence library calculations using Qubit 1.0 Fluorometer (Life Technologies, Grand Island, NY, USA) and Genomic DNA ScreenTape Analysis (Agilent Technologies, Santa Clara, CA, USA). Next, sequence libraries mounted on 468 cancer-related genes from the MSK-IMPACT Clinical Sequencing Cohort (Supplementary Table 1) were prepared using DNA from the lesions and blood cells using our sequence library method. The resulting pooled libraries were sequenced using paired-end reads on the HiSeq X platform (Illumina, San Diego, CA, USA). Sequencing reads were analyzed and annotated as described in the Supplementary Text.
Deep sequencing via cancer multigene panel testing revealed that the tumor contained point mutations, including PTPRD S1461*, TP53 I255del, and KDM6A R1279*. In addition, copy number variations were identified, such as the amplification of chromosome 7, which includes RAC1, ETV2, EGFR, MET, and BRAF; amplification of the long arm of chromosome 20 (20q), which includes BCL2L1 and AURKA; and amplification of FGFR1 and MYC (Table 1).
Table 1 Pathogenic mutations and alterations of this caseThis study was approved by the Institutional Review Board of Hiroshima University Hospital (approval number: E-1869) and was conducted in accordance with the principles of the Declaration of Helsinki. Written informed consent was obtained from the patient.
留言 (0)