
記住我

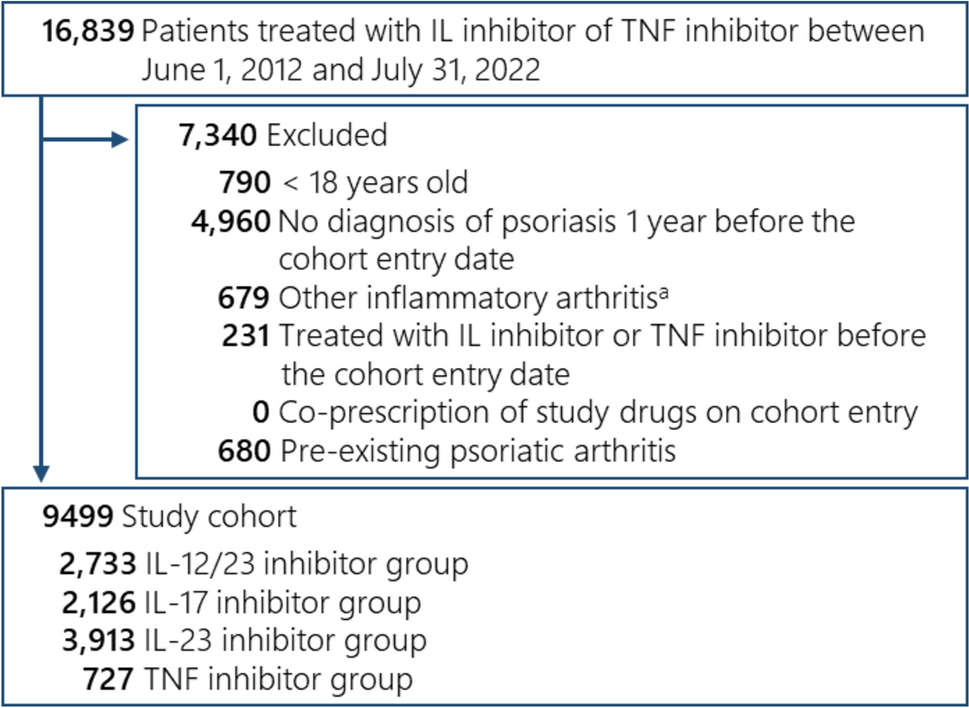




Searches conducted on 29 September 2023 identified 9942 records. After deduplication and title/abstract screening, 178 articles were selected for full-text retrieval and were reviewed, and 29 were included. Of the 29 studies, 18 reported on adverse outcomes, including hypersensitivity (n = 2), 7 reported on pharmacology, and 15 reported on antibodies, of which 6 reported only on anti-PEG antibodies and 9 reported on both anti-PEG antibodies and antibodies against the PEGylated drug. A summary of the study characteristics, patient characteristics, and outcomes is presented in Table 3. Most studies were observational (n = 16) or prospective clinical trials (n = 10). The most common disease areas were acute lymphoblastic leukemia (ALL; n = 7) and hepatitis C virus (HCV; n = 5) (Fig. 1); the most common study locations were USA (n = 8) and Germany (n = 6), and most studies were conducted in adult populations (n = 17).
Table 3 Overview of the 29 studies and their outcomesFig. 1
Included studies by disease area. ALL acute lymphoblastic leukemia, BrCa breast cancer, CTCL cutaneous T-cell lymphoma, HCV hepatitis C virus, N/A not available, T1D type 1 diabetes
3.2 Safety Outcomes3.2.1 Adverse Events (AEs)3.2.1.1 Hematologic ComplicationsIn six studies of patients with HCV or cancer, hematologic AEs were associated with a PEGylated versus non-PEGylated product (Table 3) [22,23,24,25,26,27]. A study of adolescents and adults with newly diagnosed acute lymphoblastic leukemia (ALL) reported a longer duration of coagulation dysfunction (p = 0.002) and agranulocytosis (p < 0.01) in patients treated with PEGylated asparaginase (PEG–ASP) compared with E. coli asparaginase (l-ASP), which the authors attributed to the longer half-life and decreased immunogenicity of PEG-ASP compared with l-ASP [22]. In a multicenter, open-label, randomized phase 3 study of adults with melanoma, the rates of granulocytopenia (p < 0.0001) and leukocytopenia (p = 0.0001) were 3 and 5 times higher, respectively, in patients receiving PEGylated interferon (PEG-IFN) versus IFN [25]. The authors suggested that, in addition to differences in PK, the higher rates of AEs may be due to differences in dosing between PEG-IFN (100 µg per week) and IFN [3 million units (MU) 3× per week], which could have resulted in a higher overall dose in the PEG-IFN arm [25]. Leukopenia also occurred in more than twice as many patients receiving PEG-IFN compared with IFN [56% versus 23.5%; p = not reported (NR)] in another phase 3 study in adult patients with melanoma [23]. An observational study of adult patients with hepatitis C virus (HCV) reported neutropenia in a significantly higher proportion of patients treated with PEG-IFN + ribavirin versus IFN + ribavirin (48% versus 9%; p = 0.0009) [27]. Two Cochrane systematic reviews of patients with HCV also reported that those treated with PEG-IFN + ribavirin had more than twice the risk of developing neutropenia [risk ratio (RR): 2.15; 95% CI 1.76, 2.61; p < 0.0001 [24], and RR: 2.25; 95% CI 1.58, 3.21; p = NR [26]] compared with those treated with IFN + ribavirin. The Cochrane reviews also reported that patients receiving PEG-IFN + ribavirin had more than twice the risk of developing thrombocytopenia (RR: 2.28; 95% CI 1.14, 4.54; p = NR [26], and RR: 2.63; 95% CI 1.68, 4.11; p < 0.0001 [24]) than patients receiving IFN + ribavirin.
3.2.1.2 Hepatic ToxicityIn four studies of patients with diabetes or cancer, hepatic toxicity was significantly associated with a PEGylated versus non-PEGylated product [23, 28,29,30]. In one of the phase 3 trials of patients with melanoma, rates of liver enzyme elevation were at least twice as high in the PEG-IFN arm compared with the IFN arm [alanine transaminase (ALT): 33.0% versus 16.5%, p = NR; aspartate transaminase (AST): 19.1% versus 9.4%, p = NR] [23]. In adults with high-risk, Philadelphia chromosome-negative ALL, the rates of grade 3 or 4 hepatic toxicity were higher in patients receiving PEG-ASP compared with l-ASP, both during induction therapy (p = 0.055) and consolidation therapy (p = 0.009). The authors attributed the differences in AE rates in the consolidation period to differences in the duration of activity between PEG-ASP and l-ASP [30]. In two randomized phase 3 trials in adults with type 1 diabetes (T1D), a significantly higher proportion of patients receiving basal insulin peglispro (BIL) had an ALT elevation ≥ 3× upper limit of normal (ULN) versus those receiving insulin glargine (GL), and ALT levels were significantly higher at 26, 52, and 78 weeks (all p < 0.001) in patients receiving BIL versus GL. The authors noted consistent findings in other studies of PEGylated drugs, but did not propose an explanation for these observations [28, 29].
3.2.1.3 Other AEsInjection site reactions (ISRs): In four studies of patients with HCV or diabetes, ISRs were associated with a PEGylated versus non-PEGylated product [24, 26, 28, 29]. Two Cochrane reviews reported a higher risk of ISRs in patients with HCV receiving PEG-IFN + ribavirin compared with IFN + ribavirin (RR: 1.71; 95% CI 1.50, 1.93; p < 0.0001 [24] and 2.56; 95% CI 1.06, 6.22; p = NR [26]). A significantly higher proportion of ISRs was also reported in two randomized phase 3 trials in adults with T1D receiving BIL compared with those receiving GL (p < 0.001 for both trials), possibly due to factors affecting injection site location and the slow absorption of BIL through the lymphatic system [28, 29].
Bone and/or joint pain: Three studies of cancer or HCV reported bone pain or arthralgia [24, 26, 31]. In patients with breast cancer, bone pain occurred in a higher proportion of patients with PEGylated granulocyte colony-stimulating factor (PEG-G-CSF) compared with G-CSF (p = 0.09) [31]. Cochrane reviews of patients with HCV also reported a higher proportion of patients with arthralgia in patients receiving PEGylated therapy versus non-PEGylated therapy (30% versus 24%; RR: 1.19; 95% CI 1.05, 1.35; p = 0.01) [24, 26].
Gastrointestinal AEs, including nausea and vomiting: In two studies of patients with breast cancer and melanoma, gastrointestinal effects (p = 0.005) and nausea or vomiting (p = 0.003) occurred in a significantly higher proportion of patients treated with PEGylated versus non-PEGylated therapy [25, 31]. Grob et al. suggested that dosing differences between the PEG-IFN arm and the IFN arm, which possibly corresponded to a higher dose in the PEG-IFN arm, may have contributed to higher rates of toxicities with the PEGylated treatment [25]. The Cochrane review of patients with chronic HCV reported a significantly greater risk of nausea with PEG-IFN + ribavirin versus IFN + ribavirin (RR: 1.13; 95% CI 1.01, 1.26; p = 0.03) [24].
Infections: A study of patients with HCV reported higher rates of infection with PEG-IFN + ribavirin vs. IFN + ribavirin, as well as an increased risk of all infections [hazard ratio (HR): 4.6; 95% CI 1.7, 12.0; p = 0.0019], non-respiratory infections (HR: 9.2; 95% CI 2.1, 39.3; p = 0.003), and respiratory infections (HR: 1.49; 95% CI 0.35, 6.3; p = NR) [27].
In a study of patients with cutaneous T-cell lymphoma, a significantly higher risk of ophthalmological side effects was observed with PEG-IFN compared with IFN (p = 0.0035) [32]. In the clinical trial of patients with T1D, BIL resulted in significantly increased serum triglycerides compared with GL (p < 0.001), possibly because of the increased fatty acids in the liver resulting from lipolysis of adipocyte triglycerides due to the decreased peripheral insulin activity of BIL [28]. In the Cochrane review of patients with HCV, dermatologic symptoms were reported in a higher proportion of patients treated with PEG-IFN + ribavirin versus IFN + ribavirin (36% versus 20%; RR: 1.78; 95% CI 1.15, 2.73) [26]. In the clinical trial of patients with melanoma, a significantly higher proportion of patients treated with PEG-IFN versus IFN reported fatigue (p = 0.0003) and weight loss (p = 0.04), which the authors theorize may be due to dosing differences and differences in PK between the two treatment arms [25].
3.2.2 Severe Adverse Events (SAEs)Four studies reported significant associations between PEGylated therapeutics and severe AEs. The rate of grade 3 or 4 AEs in patients with melanoma receiving PEG-IFN was almost twice that of patients receiving IFN (p < 0.0001) [25], while the rate of grade 4 or 5 infections was more than three times higher among those treated with PEG-ASP versus l-ASP (p = 0.018) [22]. Grade 3 or 4 allergic reactions were also significantly more frequent in patients with ALL treated with PEG-ASP versus l-ASP (p = 0.028) [33], as were rates of grade 3 or 4 hepatic toxicity during consolidation therapy (p = 0.009), possibly because of the differences in the duration of PEG-ASP and l-ASP activity during the consolidation period [30].
3.2.3 AE-Related Discontinuations and Dose ModificationsThree studies reported higher rates of AE-related dose reductions or discontinuations with PEGylated versus non-PEGylated therapeutics. In one study of patients with melanoma, more patients treated with PEG-IFN discontinued treatment due to an AE versus patients treated with IFN (19.4% versus 12.8%; p = NR) during months 0–18 of treatment, which the authors suggested could be because of differences in PK as well as dosing differences between the PEG-IFN arm and the IFN arm [25]. The intended 36-month treatment in the PEG-IFN arm was not possible due to high rates of discontinuation, resulting in a median treatment duration of 19.2 months [25]. Approximately half of the PEG-IFN treatment interruptions were AE-related, with a large proportion of reasons for discontinuations remaining unclear, suggesting difficulty coping with treatment, possibly due to loss of motivation resulting from decreased quality of life (QoL) [25]. In another study of patients with melanoma, a significantly greater proportion of patients treated with PEG-IFN did not receive the full dosage and duration of treatment due to AEs (26% vs. 13%; p < 0.001) [23]. In a study of patients with HCV, almost twice as many patients treated with PEG-IFN required a dose reduction due to AEs compared with those treated with IFN (p < 0.05). A similar pattern was observed for dose reductions due to anemia and leukopenia specifically, with more than twice as many patients in the PEG-IFN group experiencing a reduction versus the IFN group (p < 0.05), possibly due to the increased half-life of PEG-IFN [34].
3.3 ImmunogenicityTable 3 presents an overview of the immunogenicity findings of this review. Fifteen studies reported on antibodies to different components of the PEGylated drug, of which six studies reported only on anti-PEG antibodies [17, 35,36,37,38,39] and nine studies differentiated antibodies specific to PEG, the PEGylated drug, and the native drug or linker molecule (Table 4) [19, 33, 40,41,42,43,44,45,46].
Table 4 Immunogenicity: studies reporting on antibody types detected in humans3.3.1 Prevalence of Pre-existing Antibodies to PEGFour studies reported on the prevalence of pre-existing anti-PEG antibodies in the healthy population, which ranged from 23% to 72%, and no study found any correlation between the concentrations of immunoglobulin G (IgG) and immunoglobulin M (IgM) antibodies [17, 35, 36, 38]. The prevalence of anti-PEG antibodies was higher in females than males for both IgG (p = 0.018) and IgM (p < 0.0001) [35, 36]. Both studies reported a higher prevalence of anti-PEG antibodies in the younger population, with one study reporting an anti-PEG IgG prevalence of up to 60% for 20-year-olds versus 20% for age > 50 years [35, 36]. A negative correlation for anti-PEG IgG concentration was reported with age in females (p = 0.0073) and males (p = 0.026) [35].
3.3.2 Frequency and Prevalence of Antibody TypesOne clinical trial of pediatric patients with ALL reported on the frequency of differentiated antibodies specific to PEG, the PEGylated drug, and the native drug. Of the 11.5% of samples that tested positive for anti-PEG-ASP in the study, 80.1% were positive for anti-PEG alone, 15.5% were positive for both anti-PEG and anti-l-ASP, and 1.5% were positive for anti-l-ASP alone [33]. In another study of pediatric patients with ALL, the prevalence of pre-existing anti-PEG antibodies was higher prior to first administration of PEG-ASP (IgG 13.9%; IgM 29.1%) and decreased following administration of PEG-ASP (IgG 4.2%; IgM 4.5%) [37].
3.3.3 Treatment-Emergent Antibody ResponseTwo clinical trials of patients with T1D reported a significantly higher proportion of patients experiencing a treatment-emergent antibody response with the PEGylated product BIL versus non-PEGylated GL (p = 0.002 and p < 0.001) [28, 29].
3.3.4 Hypersensitivity Reactions
留言 (0)