In an online survey of bariatric surgical members of the international bariatric club (IBC), 64 of 93 responders operated on bariatric tourists with 22% of bariatric surgeons reporting complications [5]. VTE complications were 7.8% and only 12.7% of all patients maintained follow-up until the removal of stitches. More strikingly, only 72.6% recommended follow-up with bariatric teams in the country of origin [5]. In comparison, registry data suggests a VTE complication rate of 0.33–2.99% in patients undergoing bariatric surgery [6, 7]. In our cases, these patients had not been referred to a bariatric team for follow-up and a thromboprophylaxis management plan was not provided. Post-operative surgical follow-up was absent and language barriers were faced.
Daigle et al. [8] showed that of eight specific complications following bariatric surgery which included bleeding, VTE, leak, wound infection, pneumonia, urinary tract infection, myocardial infarction and stroke, VTE had the greatest effect on readmission and mortality [8]. Moreover, according to previous estimates, VTE is the cause of 17% of postoperative deaths following bariatric surgery [9]. In view of this, many bariatric surgery centres provide post-operative VTE prophylaxis following surgery, especially since Porto-mesenteric thrombosis (PMT) following bariatric surgery has previously been reported and has the potential to be organ or life-threatening [10].
Obesity in itself is an independent risk factor for VTE [11]. Hotoleanu et al. [12] showed that obesity was associated with a 6.2-fold increase in risk for VTE with the highest risk for those with class II and III obesity [12]. In the obese state, multiple signalling pathways are activated to stimulate an inflammatory response. Adipose tissue is a known inflammatory mediator and IL-1,IL-6, IL-8 and TNF-α are cytokines that are inducers of the acute phase response that can be released by human adipose cells [13]. It is thought that 15–35% of systemic IL-6 is produced from white adipose tissue [14]. IL-6 works with other interleukins to increase thrombopoietin and stimulate megakaryocytopoiesis leading to an increased platelet count [15]. Furthermore, obesity is associated with elevations in coagulation and von Willebrand factor as well as impaired fibrinolysis [16, 17]. Bureau et al. [18] found that central obesity is associated with portal vein thrombosis (PVT) in patients without liver cirrhosis [18]. Given these factors, patients undergoing bariatric surgery are already at a higher risk for VTE.
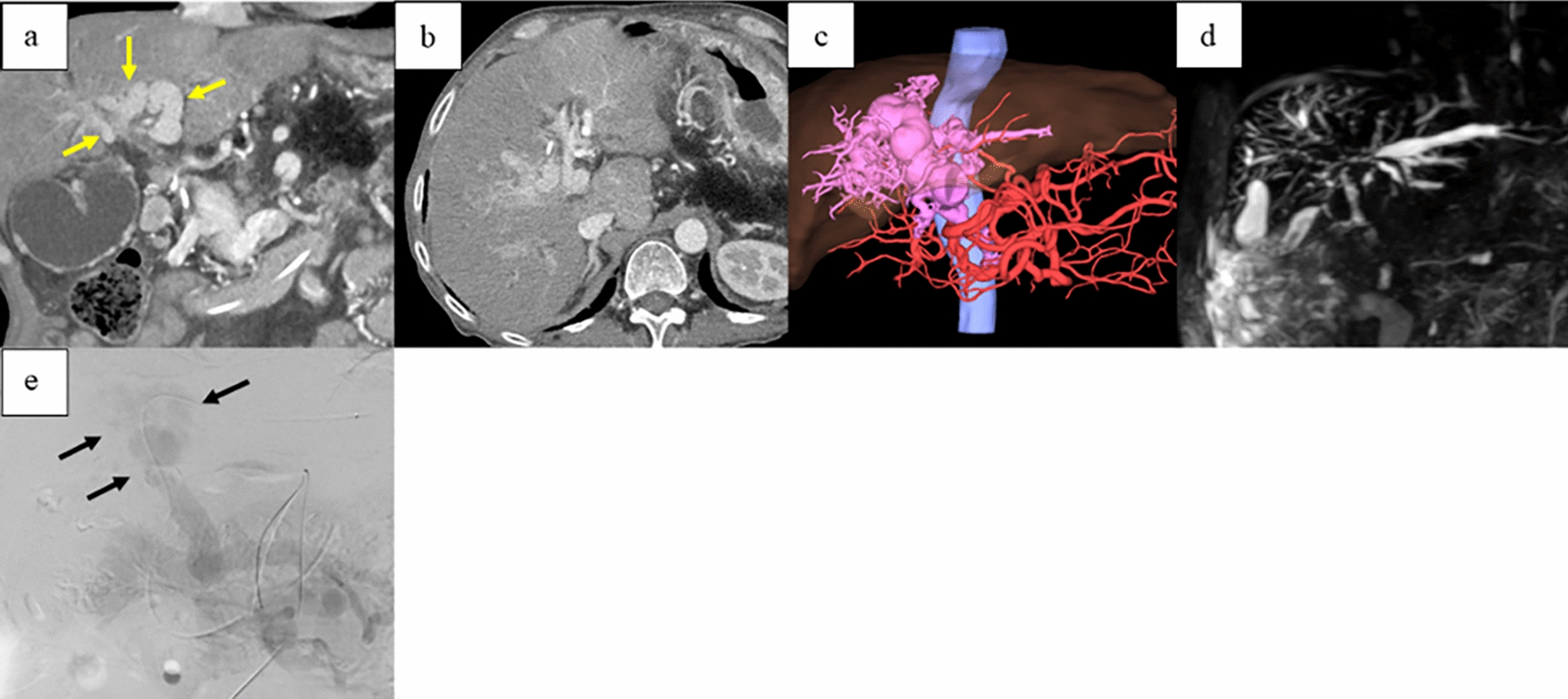
PMT, defined as partial or complete occlusion of the portal venous system, may involve intra and extrahepatic veins, extending distally to involve the splenic or mesenteric veins. The Yerdel classification is a commonly used method to stage the extent of PVT involvement and this correlates well to clinical severity. Critically, acute PVTs can lead to intestinal infarction and carry a mortality rate of up to 50% [19]. Its associations with a variety of conditions including intra-abdominal infection, cirrhosis, malignancy and a consequence of abdominal surgery are well established. With the advancement of medicine, other risk factors such as inherited thrombophilias and other causes of acquired prothrombotic states are increasingly recognised as causes of PVT. Over the last several decades, reports of PVT have emerged following laparoscopic surgery that did not involve the portal-venous system [20]. The incidence of PVT following bariatric surgery is thought to be between 0.3 and 1% [21,22,23].
Surgical sleeve gastrectomy is the most practised method of weight loss surgery and constitutes up to 60% of bariatric procedures worldwide [24, 25]. During this surgery, the gastroepiploic and short gastric vessels are usually dissected [26] along with a significant portion of the stomach which may result in abnormal vascular flow in the remnant tissue [21]. Therefore, this surgical technique likely results in an increased risk of PMT compared to other methods of weight loss surgery [27]. In contrast, the Roux-en-Y gastric by-pass method preserves the main body of the stomach and its natural anatomy, and adjustable gastric bands avoid transection of the stomach and injury to gastric vessels which may explain the markedly lower occurrences of PMT observed with these techniques [27]. Bilio-pancreatic diversion, another method of weight loss surgery, is now infrequently used [21] but there have also been reports of PMT after these procedures [28]. Nonetheless, it is important to consider that the comparatively higher volumes of surgical sleeve gastrectomies may be a confounding factor.
Clinical presentation typically may include abdominal pain, fever, diarrhoea and gastrointestinal bleeding. When thrombosis extends to the mesenteric or splenic veins, patients may present unwell with signs of bowel ischaemia, septic shock and multi-organ failure. The median onset of diagnoses may range from day 1 post-surgery to day 28 [29]. Diagnoses are typically made following cross-sectional abdominal imaging. Chronic PVT may have profound lifelong complications including non-cirrhotic portal hypertension with ascites and varices. It is, therefore, necessary that management not only include lifesaving treatment, but one must also consider how to prevent lifelong complications if possible.
Besides the pathophysiological factors discussed above, other important and common causes of postoperative complications in medical tourism include inconsistent safety standards and discontinuity in patient care [30, 31]. VTEs after sleeve gastrectomy and Roux-en-Y bariatric surgery can be prevented with extended anticoagulation and an enhanced recovery protocol [32]. None of our cases were provided notes of their operation and the recovery process, and only one patient received low-dose anticoagulation. Importantly, flying after recent surgery increases the risks of VTEs because patients are in a “pro-thrombotic” state and are less mobile than usual. As such, the UK Civil Aviation Authority recommends abstinence from flying for 3–4 weeks after major laparoscopic abdominal surgery like a laparoscopic cholecystectomy [33]. However, in these cases, the patients flew back to the UK within 7 days of surgery because they were not advised appropriately. Therefore, better safeguards are needed for patient protection as more patients turn to foreign medical service providers for bariatric surgery.
With regards to anticoagulation, the 2021 International Society on Thrombosis and Haemostasis guidelines do not recommend the use of direct oral anticoagulants (DOACs) for the treatment or prevention of VTE in the first 6–12 months following bariatric surgery however, this was based on studies involving small patient cohorts [34]. In a randomised clinical trial including 272 patients undergoing bariatric surgery, VTE prophylaxis with 10 mg rivaroxaban was found to be efficacious and safe [35]. Interestingly, the American Association for the Study of Liver Diseases (AASLD) recommends treatment of acute PVTs (within 6 months of presentation) with anticoagulation [36].
In conclusion, with the continuing rise of global obesity, the number of patients seeking bariatric surgery will increase in parallel. Unfortunately, without increased access to bariatric surgery in the public sector, longer waiting times will continue and patients may seek alternative options such as ‘’bariatric tourism’’ without fully understanding the risks that entails. Porto-mesenteric complications are significant and have profound lifelong consequences. Therefore, it is imperative that patient education is significantly improved, and more stringent regulations by health authorities are put in place to avoid the growing complications of negative health tourism.








留言 (0)