
記住我







This single-center study was performed as a retrospective observational study at a tertiary care academic medical center. The following criteria were applied to determine the study population: (a) mCRPC with tumoral PSMA expression above liver uptake in PSMA-PET; (b) approval of the interdisciplinary tumor board for RLT with [177Lu]PSMA-617; (c) patients received at least 2 cycles of RLT as well as restaging after the second cycle; (d) applicable medical records and imaging follow up; (e) age > 18 years. This study was approved by the local ethics committee (No. 2019–711-f-S). This study has been carried out in accordance with the ethical standards outlined in the 1964 Declaration of Helsinki and its subsequent revisions.
A total of 288 consecutive patients between 2015 and 2021 (to ensure sufficient follow-up time) underwent [177Lu]PSMA-617 therapy. 188 of 288 patients (65%) met the aforementioned inclusion criteria. The flow chart in Fig. 1 displays a comprehensive patient selection process.
Fig. 1
Patient selection process
PSMA-PET imagingAll patients underwent serial imaging with either PSMA-PET computed tomography (PET-CT) or magnetic resonance imaging (PET-MRI). PET imaging was performed prior to RLT (initial PET), 6–8 weeks after the second cycle, and 6–8 weeks after the fourth cycle. Examination was performed using either a Biograph mCT 128 or a 3T Biograph mMR system (Siemens Healthcare, Erlangen, Germany). Patients were imaged with inhouse produced radiolabeled [68Ga]PSMA-11 or [18F]PSMA-1007 as described before [21, 22]. For a valid comparison, patients underwent serial imaging using either [68Ga]PSMA-11 or [18F]PSMA-1007.
[177Lu]PSMA-617 and WBS imagingAll patients received [177Lu]PSMA-617 (ABX GmbH, Radeberg, Germany) based on literature recommendations [23]. The radiosynthesis procedure and quality control parameters were conducted in-house as previously described [24]. [177Lu]PSMA-617 was slowly administered intravenously over a period of 30 s in our therapy unit.
A planar WBS (anterior / posterior) was obtained for each cycle 48 h after injection using a Discovery NM/CT 670 Pro System (General Electric Company Boston, Massachusetts, USA) or a Symbia T2 (Siemens Healthcare, Erlangen, Germany). Image acquisition was performed with parallel collimators in a continuous scanning mode with a zoom of 1.0, utilizing a 2.21 mm pixel size and a speed rate of 15 cm/min with a photopeak at 113.0 and 208.0 keV (± 10%).
Image analysisAll imaging data were reviewed by two experienced nuclear medicine physicians in consensus. Both reviewers were blinded to the clinical outcome as well as other collected parameters (i.e., PSA progression / regression).
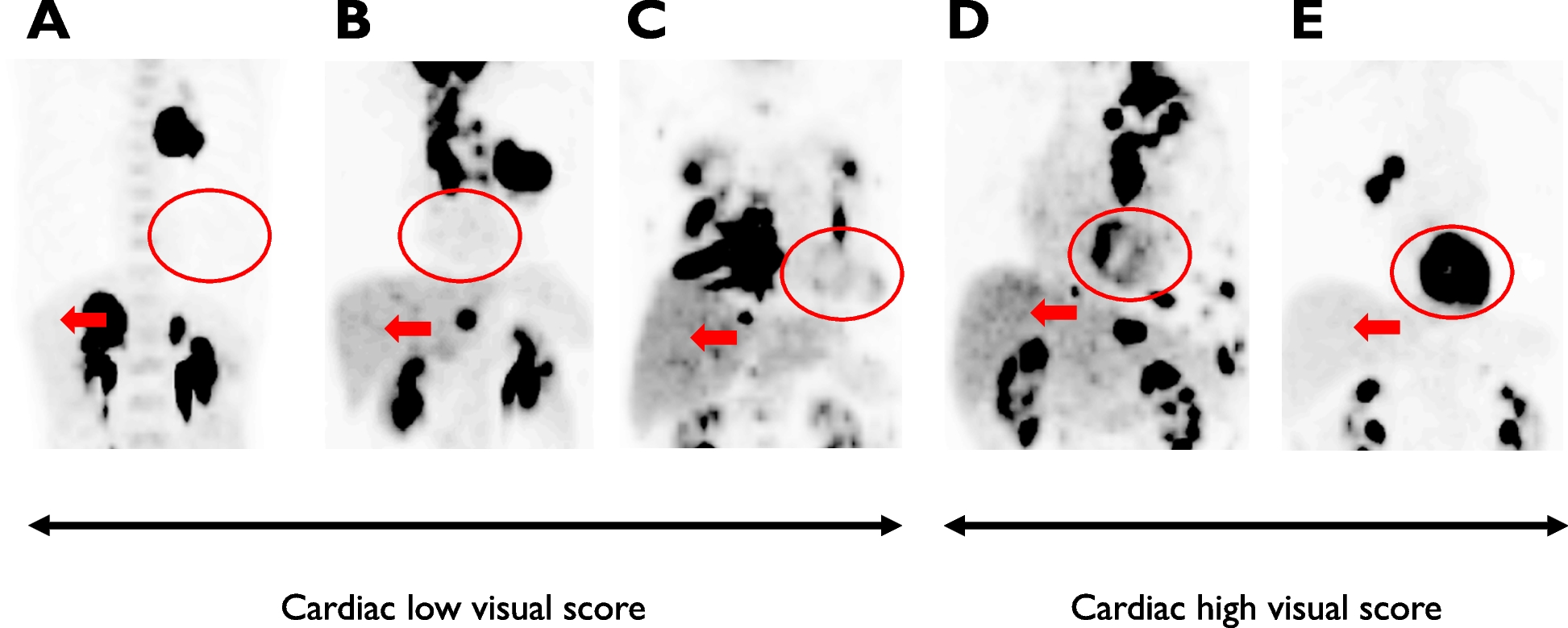
The images were visually interpreted based on the uptake of the radiotracer. For this purpose, the lesional uptake was categorized according to the PROMISE V2 criteria as follows: (0) equal to or lower as blood pool; (1) equal to or lower than liver and higher than blood pool; (2) equal to or lower than parotid gland and higher than liver; (3) higher than parotid gland. In the case of [18F]PSMA-1007 with high liver excretion, the spleen was employed as the reference organ in accordance to PROMISE V2 [16]. This assessment included the maximum intensity projection (MIP) of the initial PET and the PET after two cycles of RLT, as well as planar WBS after first, second and third cycle, if applicable. The PROMISE V2 PSMA-expression score was reported for the entire tumor burden (overall), as well as for the lesions with the highest and lowest uptake.
PROMISE V2-scores were correlated between initial PET and first cycle WBS, as well as between third cycle WBS and PET after the second cycle.
Response assessmentWBS after first, second and third cycle, and restaging PET scans after two and four cycles were compared to initial PSMA-PET. Response was defined as follows: complete response (CR) was defined as the absence of PSMA uptake in all lesions that were previously avid. Partial response (PR) was defined as the absence of PSMA uptake in more than two previously avid lesions or obviously reduced PSMA-avid tumor volume. Progressive disease (PD) was defined as the occurrence of new PSMA-avid lesions or obviously progressed PSMA-avid tumor volume. Stable disease (SD) was defined as neither aforementioned CR, PR, or PD criteria [16]. Disease control rate (DCR) for imaging response assessment was defined as CR, PR, or SD and progress as PD.
The imaging response correlation was used to compare the two different modalities (PET and WBS) in terms of DCR and progression. A correlation analysis was performed between PET after two cycles of RLT and the second cycle WBS, as well as a correlation between the PET after four cycles of therapy and third cycle WBS.
A decline of at least 50% in their PSA levels is considered as biochemical response (PSA50), in line with the previously published studies on mCRPC patients undergoing RLT with [177Lu]PSMA-617 using a cutoff of 50% PSA-decline [10]. A correlation analysis was conducted to investigate on the relationship between early biochemical response and imaging response. The analysis involved the PET after two cycles of RLT / WBS of the third cycle and PSA50.
Statistical and survival analysisClinical and demographic data are presented as total number, median, percentage, range and 95% confidence interval (95%CI). Binary and ordinary variables were correlated with Cramer V (cφ) and Spearman (rs) test. Values of greater than 0.20, 0.40, 0.60 and 0.80 for cφ and rs correspond to low, intermediate, strong, and very strong positive correlation. OS analyses were tested for their prognostic value with log rank test and Kaplan-Meier survival analysis. Hazard ratios (HR) with 95%CI were calculated using a stratified Cox proportional hazard model. Null hypothesis was rejected if P-value was less than 0.05 (two-sided for correlation tests). Statistical analysis was performed using SPSS Statistics version 28.0.1.1. (SPSS Inc.).
留言 (0)