
記住我
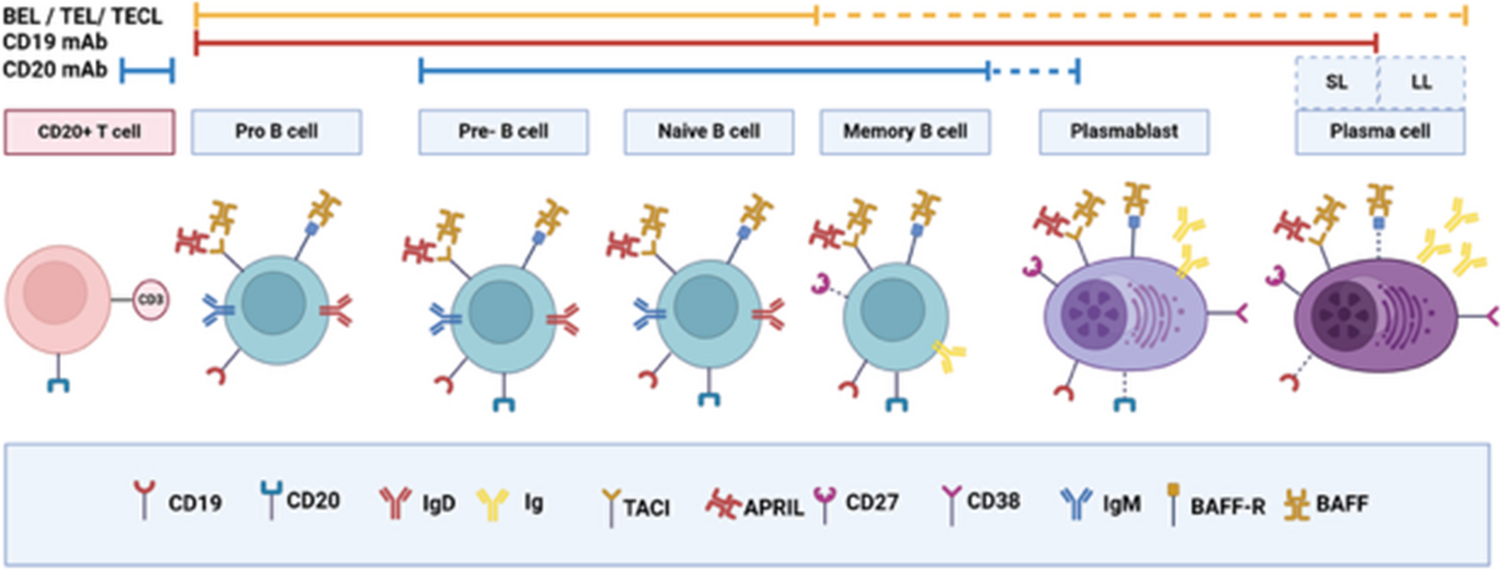





PXVX0317 is a VLP vaccine that was initially developed by the US National Institutes of Health Vaccine Research Center. The vaccine (Fig. 2) contains recombinant CHIKV structural proteins capsid, E3, E2, 6K, and E1, which were derived from Senegalese CHIKV strain 37997, a member of the West African genotype. Following in vitro expression of the CHIKV structural gene cassette, the structural proteins self-assemble into a particle that is highly similar to wild-type CHIKV but that cannot replicate because of the absence of a viral genome [34]. The rationale for the VLP approach is that structural proteins enable attachment, entry, and fusion into host cells to resemble a CHIKV virion and induce NAb responses that are similar to wild-type CHIKV. In initial studies, NHP immunized with VLP-generated NAb and were protected from viremia after a wild-type CHIKV challenge [34]. These data served as the precedent for further development of this vaccine, discussed in detail below.
Fig. 2
Design of the PXVX0317 virus-like particle (VLP) vaccine. The chikungunya virus (CHIKV) non-structural genes were removed and the structural proteins: capsid, E2 and E1, along with accessory proteins E3 and 6K, were expressed from a human cytomegalovirus (CMV) R vector that comprises the human CMV early enhancer/promotor, a human T-cell leukemia virus-1 R region containing a splicing donor, a CMV immediate early-splicing acceptor, and a bovine growth hormone poly A signal. nsP is non-structural protein. A publishing license was granted for the image created in Biorender
7.1 Pre-Clinical Evaluations7.1.1 Immunogenicity and Efficacy in Animal ModelsMice Initial immunogenicity studies for PXVX0317 were performed in female BALB/C mice aged 6–8 weeks that were injected intramuscularly in the right and left quadricep muscles two times with a 1-month interval in between injections [34]. For some animals, the immune stimulatory adjuvant Ribi was also included together with PXVX0317. Compared with mice that received saline, mice administered adjuvanted PXVX0317 developed high titer NAb responses against the homologous 37997 strain and a heterologous CHIKV LR2006-OPY1 strain. Mice that received non-adjuvanted PXVX0317 also mounted NAb responses, although titers were lower than in mice that received adjuvanted vaccine.
Non-Human Primates Immunogenicity studies for PXVX0317 were performed in rhesus macaques [34]. Adult animals aged 3–4 years were administered PXVX0317 intramuscularly three times at weeks 0, 4, and 24. All developed NAb against homologous and heterologous CHIKV after the first immunization and titers increased with second and third immunizations. To assess protective efficacy, 15 weeks after the third immunization, animals were challenged intravenously with heterologous CHIKV LR2006-OPY1. Vaccinated animals did not develop detectable viremia 2 days post-inoculation, the time of peak viremia non-vaccinated rhesus macaques. Monocyte levels were also unchanged in vaccinated animals, contrasting with non-vaccinated controls, which showed increased levels. To evaluate the protective role of antibody after VLP vaccination, purified total IgG from immunized or control animals was passively transferred via an intravenous infusion into immunodeficient mice with defective type 1 interferon signaling (interferon-α/β receptor-1 knockout, Ifnar1–/–), followed by a challenge with a lethal dose of CHIKV LR2006 OPY-1 1 day later. Mice that received IgG from vaccinated macaques did not develop detectable viremias and were protected from lethal disease, demonstrating the protective role of vaccine-stimulated IgG against CHIK.
7.1.2 Animal ToxicologyNo publicly available data evaluate the toxicology of PXVX0317.
7.2 Clinical Trials7.2.1 Design and Protection from DiseaseSafety and immunogenicity of PXVX0317 were evaluated in three clinical trials that were conducted at vaccine trial sites across the USA comprising a combined total of nearly 1000 healthy participants aged 18 years and older. These data are reported in three publications describing the trials and three additional publications reporting on antibody responses, all of which are detailed below.
In the first study [53], a phase I dose-escalation, open-label clinical trial (ClinicalTrials.gov NCT04189358) was performed to evaluate the safety and tolerability of PXVX0317, which was named VRC-CHKVLP059-00-VP at the time. A total of 25 healthy adults aged 18–50 years were enrolled at the NIH Clinical Center, Bethesda, MD, USA in 2011–12. Participants received three sequential doses of 10 μg, 20 μg, or 40 μg administered intramuscularly in the deltoid on weeks 0, 4 and 20, and a follow-up at 44 weeks. Safety monitoring was similar to parameters used for IXCHIQ clinical trials and was performed via clinical and laboratory assessments. Vaccine injections were well tolerated with no serious adverse events. Thirty-six percent (9/25) of participants reported local reactogenicity and 40% (10/25) reported systemic reactogenicity at least once, usually manifest as malaise, headache, chills, nausea, fever, or joint pain.
Following success of the phase I trial, a phase II clinical trial for PXVX0317 (ClinicalTrials.gov NCT02562482) was performed next [54], in the period from 2015 to 2018. The trial was a randomized, placebo-controlled, double-blind study in male and female individuals at clinics in Dominican Republic, Guadeloupe, Haiti, Martinique, and Puerto Rico with 400 healthy adults aged 18–60 years as participants. The goal of the study was to evaluate the safety and tolerability of the vaccine in people in CHIKV endemic regions. Study participants received two intramuscular injections of VLP 20 μg 28 days apart (N = 201) or placebo (N = 199) and were followed for up to 72 weeks (1.5 years). Safety monitoring was similar to metrics from the phase I study and included laboratory parameters, adverse events, and tolerability based on local and systemic reactogenicity. As the study was conducted in CHIKV endemic regions, CHIKV infection was also evaluated. Candidate subjects were excluded from the study if they showed CHIKV IgG/IgM antibodies prior to enrollment. Similar to the phase I study, PXVX0317 was well tolerated with no serious vaccine-related adverse events reported. Thirty two percent (64/201) of participants in the vaccine group reported local reactogenicity, including pain or tenderness and swelling, compared with 19% (37/199) in the placebo group. Solicited symptoms reported included malaise, headache, myalgia, chills, nausea, fever, and joint pain, with 44% (87/201) of vaccinees reporting at least one symptom, which was higher than in the placebo groups. Unsolicited adverse events included neutropenia, bradycardia, hypotension, viral infection, rash, chest pain, dry lips, light headedness, fever, myalgia, gastroenteritis, abdominal pain, anemia, increased alanine aminotransferase, and hematoma, and were more common in the vaccine group (75%, 12/16) compared with the placebo (25%, 4/16) group. Despite being in a CHIKV endemic area, CHIK was not reported in any study participants during the trial.
A second phase II trial [55] (ClinicalTrials.gov NCT03483961) was next performed for PXVX0317 from 2018 to 2020, with a goal of informing selection of dose, adjuvant formulation, and immunization schedule for phase III trials. Instead of using unadjuvanted PXVX0317 as in the prior two clinical trials, PXVX0317 was prepared in an aluminum hydroxide-adjuvanted formulation. Adjuvants are intended to produce higher, earlier, and longer lasting immune responses when added to vaccines compared with non-adjuvanted formulations; the specific adjuvant selected for this study was intended to increase the efficiency of antigen uptake and release at the injection site. The study consisted of a randomized, double-blinded, parallel-group trial and was conducted at three clinics in the USA in healthy male and female CHIKV-naïve adults aged between 18 and 45 years, with a 2-year timeline between the first vaccination and study end. Participants were assigned to one of eight vaccination groups: two doses of unadjuvanted PXVX0317 28 days apart (2 × 20 μg; standard); adjuvanted PXVX0317 at two doses 28 days apart (2 × 6 μg, 2 × 10 μg, or 2 × 20 μg); a booster dose 18 months after the first active injection (40 μg; standard plus booster); two doses 14 days apart (2 × 6 μg, 2 × 10 μg, or 2 × 20 μg; accelerated); or one dose (1 × 40 μg; single). Immunogenicity and safety were study endpoints. In most groups, the majority of vaccinated participants reported solicited adverse events including injection-site and systemic reactions, where events were more common after the first vaccination. The most common solicited adverse event was injection-site pain, reported in 15–49% of participants, depending on the vaccine group. Common solicited adverse reactions were fatigue, headache, and myalgia across all dose groups and more common after the first vaccination. No treatment-related severe adverse events were reported. Significant differences in adverse events across vaccine groups were not reported.
A multi-center, randomized, double-blind, placebo-controlled, parallel-group phase III trial was performed next (ClinicalTrials.gov NCT05072080); some unpublished results are available [56]. Study subjects aged 12–64 years received VLP (2790 participants) or placebo (464 participants) as a single intramuscular injection. Ninety eight percent (2503/2559) of vaccinated participants achieved 80% neutralization test (NT80) serum neutralizing antibody titers of ≥ 100 by 22 days after vaccination; by contrast, only 1% (5/424) of placebo-treated participants achieved this NT80 serum neutralizing antibody level. Antibody responses were detected in all age groups. The most common adverse events were myalgia, fatigue, and headache.
7.2.2 Immunogenicity, Breadth, and Durability of ProtectionIn the phase I trial [53], immunogenicity was evaluated by measuring CHIKV-specific NAb titers using heterologous genotype CHIKV antigens or viruses at multiple intervals in the study timeline. Neutralizing antibodies were detected in all dose groups after the second vaccination and levels were boosted after the third. One month after the third vaccination, the GMT of the half-maximum inhibitory concentration was 8745 for participants who received 10 μg, 4525 for the 20-μg group, and 5390 for the 40-μg group. A second study [57] evaluated antibody responses generated by vaccinated participants in the phase I trial against nine CHIKV strains representing West African (homologous to PXVX0317 VLP strain 37997), ECSA, and Asian genotypes. The goal was to evaluate whether vaccination elicits cross-reactive NAb against all three genotypes (where the fourth genotype identified in the introduction of this review, Indian Ocean Lineage, is derived from the ECSA genotype), which would suggest that the vaccine cross-protects against all CHIKV across the globe. Serum from 12 study participants 44 weeks after enrollment and 24 weeks after the third vaccination was analyzed in cross-neutralization assays with several CHIKV strains from each of the three genotypes. Genotype-specific differences in neutralization potency were not measured, showing that the West African strain used in PXVX0317 produces a cross-reactive NAb response against the two other genotypes. Serum samples after the first and second vaccination were also evaluated and cross-neutralized CHIKV strains from heterologous genotypes, indicating that three PXVX0317 immunizations were not necessary to achieve neutralization breadth.
In the Phase II PXVX0317 trial [54], CHIKV NAb responses were measured in serum from blood collected at intervals after vaccination using Asian genotype CHIKV strain 181/25. All but 1 of the 192 participants (99.5%) who received both vaccinations developed NAb. The GMT in the vaccine group increased from baseline to week 8 and was higher than in the placebo group. At the 72-week study endpoint, 88% of the participants in the vaccine group who were seronegative at baseline had at least a 4-fold increase in NAb titer, and 96% were seropositive as assessed by a neutralization assay. Even though the study attempted to pre-screen and exclude participants who were CHIKV seropositive, there were regional differences in baseline NAb titers, where participants from 2 of the sites (Dominican Republic and Haiti) had higher baseline levels. Baseline timepoints were up to 56 days prior to enrollment, and many were IgG and IgM positive by IgG/IgM enzyme-linked immunosorbent assay, suggestive of either failure to exclude CHIKV participants who were seropositive at enrollment or CHIKV infection in the interval between blood collection at enrollment and vaccination. In participants who were CHIKV seropositive when vaccinated, NAb responses increased 2-fold, showing immunogenicity in spite of prior CHIKV exposure. In additional post hoc analyses from the trial [58], antibody responses post-vaccination were compared between 39 study participants with CHIKV neutralizing antibodies and 155 baseline seronegative participants. Baseline seropositive vaccinees showed stronger post-vaccination neutralizing antibody responses (peak GMT of 3594) compared to seronegative participants (1728), which persisted for 17 months. CHIKV seropositive vaccinees more frequently reported vaccine injection site swelling (10%) compared to seronegative recipients (0.6%). These data suggest that although it more frequently causes reactogenicity after administration VLP vaccine is immunogenic in people previously infected with CHIKV.
Similar to the clinical trials that preceded it, the immunology endpoint in the second Phase II trial [55] with adjuvanted PXVX0317 was assessed by measuring the GMT of CHIKV NAb, which was evaluated 28 days after the last vaccination. Neutralizing antibody titers in all vaccine groups rose within 7 days after PXVX0317 vaccination and persisted to the study end, 2 years, and a booster dose administered 18 months after the first dose augmented NAb levels. The adjuvant enhanced the magnitude of GMT 28 days after the first vaccination, with titers significantly higher in participants who received adjuvant formulations of either 2 × 10 μg or 2 × 20 μg at a 28-day interval, or 2× 20 μg at a 14-day interval, compared with the group that received 2 × 20 μg at a 28-day interval without an adjuvant. The adjuvanted formulations showed no advantage over the non-adjuvanted formulation after the second dose was administered. Geometric mean NAb titers were higher in groups that received 28 day compared with 14-day dosing intervals. Based on the results of this study, a single 40-μg injection of adjuvanted PXVX0317 is being further investigated in two phase III clinical trials. In trial NCT05072080 that was completed on 30 April, 2023, a safety, immunogenicity, and lot-consistency trial of PXVX0317 in healthy adults and adolescents was performed, for which the results are not yet available as of 29 August, 2024.
Using samples from the phase II adjuvant PXVX0317 trial, another study [59] characterized the B-cell response to evaluate the breadth of neutralization for three genotypes of CHIKV and related arthritogenic alphaviruses. This study used serum collected 1, 29, and 57 days, corresponding to baseline before vaccination, 28 days after the first vaccination, and 28 days after the second vaccination, respectively, in 20 study participants who received 2 × 20 μg adjuvant VLP at the 28 day interval. Beginning 29 days after vaccination, antibody in serum was strongly and equally neutralizing against CHIKV strains from all three genotypes. Some of the participant sera also showed >50% or 80% neutralization tests against related alphaviruses including ONNV, MAYV, and RRV, where the magnitude of PRNT50 or PRNT80 titers and rates of positivity in the 20 participants paralleled genetic distance from CHIKV in the order ONNV>MAYV>UNAV or RRV. To evaluate induction and persistence of humoral responses, CHIKV-specific B cells were isolated from peripheral blood mononuclear cells at the times above and also at 182 days, which was 153 days after the second vaccination. Chikungunya virus-specific B cells were detected in day 29, 57, and 182 sera, where cells at the last time indicate activation markers consistent with a memory phenotype.
The study also identified broadly neutralizing monoclonal antibodies (mAbs) that bind multiple sites on the E2 glycoprotein, which could reduce potential for viral escape via mutation(s) at just a single antigenic site. When passively transferred 1 day prior to challenge with CHIKV LR2006-OPY1, some of the mAbs with neutralizing activity also protected against lethal disease in Ifnar1–/– mice; mAbs with reduced in vitro neutralizing capacity were less protective. A subset of the mAbs administered to C57BL/6 mice prophylactically reduced footpad swelling, virus levels in target tissues such as the ankle and calf, and histopathologic changes in myositis compared with isotype control mAbs. Using the same approach but for other alphaviruses, two of the mAbs that showed the greatest breadth of binding and cross-neutralization reduced virus levels and swelling in joints of mice after MAYV but not RRV infection, indicating that a greater cross-neutralizing potency is needed to achieve cross-protection against RRV, which is not unexpected given RRV is more distantly related to CHIKV than MAYV.
7.3 Components and StorageThe PXVX0317 VLPs are produced by transfection of human embryonic kidney VRC293 cells with a DNA plasmid encoding the CHIKV structural genes. VRC293 cells are a suspension cell line adapted to grow without serum that were derived from HEK-293 cells, which derive from human embryonic kidneys. VRC293 cells do not contain adventitious agents and lack tumorigenicity, which are criteria for use for vaccine production based on FDA guidance [60]. After the enveloped VLPs self-assemble, they are released into the culture medium as particles. The VLPs are concentrated and purified using centrifugation, filtration, and chromatography, then formulated at the appropriate dosage and stored in sterile vials before administration. The VLP manufacturer has not published storage requirements but in prior studies [59] purified VLPs were stored at −80 °C prior to use.
留言 (0)